Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Human brain wikipedia , lookup
Microneurography wikipedia , lookup
Axon guidance wikipedia , lookup
Environmental enrichment wikipedia , lookup
Embodied language processing wikipedia , lookup
Perivascular space wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Central pattern generator wikipedia , lookup
Development of the nervous system wikipedia , lookup
Aging brain wikipedia , lookup
Synaptogenesis wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Neural correlates of consciousness wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Synaptic gating wikipedia , lookup
Neuroanatomy of memory wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Substantia nigra wikipedia , lookup
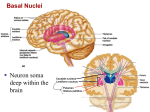
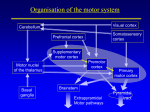
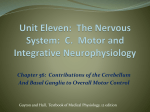
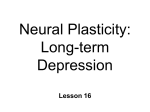
Neuroscience 7c - Basal Ganglia and Cerebellum Anil Chopra 1. Draw a diagram of the component structures of the basal ganglia and indicate how they interact. 2. Know the clinical signs of Parkinson’s disease and Huntington’s disease. 3. Explain which structures degenerate in Parkinson’s disease (PD) and Huntington’s disease (HD) and differentiate between the clinical signs of HD and PD. 4. Explain the “Alexander and Crutcher’s hypothesis” to describe the function of basal ganglia and how this can help to explain the symptoms seen in HD and PD. 5. Explain how the cerebellum contributes to the co-ordination of movement 6. Know the relevance of the pathways into and out of the cerebellum 7. Understand how the cellular organisation of the cerebellum relates to its functioning. 8. Define ataxia and explain how lesions in specific areas of the cerebellum relate to effects in the specific parts of the body. Both the basal ganglia and the thalamus act on the motor cortex to allow for smooth coordinated movement. Lesions in these areas result in movement disorders. Motor cortex via thalamus via thalamus basal ganglia cerebellum motor neurons & interneurons spinal cord Basal Ganglia caudate nucleus putamen globus pallidus GPe GPi subthalamic nucleus (STN) forebrain coronal view substantia nigra midbrain Parts of the Basal Ganglia The basal ganglia lies in the deep white matter of the cerebral cortex and consists of: Caudate Putamen (together with caudeate nucleus mane striatum). Internal and external segments of the globus pallidus (GPi and GPe) Pars reticulata and pars compacta of the substantia nigra (SNr and SNc) Subthalamic nucleus (STN) The nuclei modify movements on a minute to minute basis. They communicate with the motor cortex and the thalamus. The basal ganglia is normally inhibitory, as opposed to the cerebellum which is excitatory. The balance between the basal ganglia and cerebellum leads to smooth co-ordinated movements. Circuit of Basal Ganglia Diagram shows: Gutamatergic pathways as red (stimulatory) Dopaminergic pathways as magenta (stimulatory) GABA pathways as blue (inhibitory) Cerebral cortex stimulates striatum Pars compacta of substantia nigra stimulates striatum Striatum inhibit external globus pallidus, internal globus pallidus and pars reticular of the substantia nigra DIRECTLY. Striatum also inhibit internal globus pallidus INDIRECTLY via the external globus pallidus subthalamic nucleus internal globus pallidus. Internal globus pallidus and pars reticulum of the substantia nigra project to thalamus. They are the only outputs to the system. The thalamus projects to the cerebral cortex. (Specifically the premotor area and the supplementary motor area – the two regions involved in planning movement). The thalamus is inhibited normally, however, when the cerebral cortex wants to initiate a movement, it sets off a chain reaction which results in the inhibition of the nuclei that are inhibiting the thalamus. The thalamus therefore becomes stimulated and stimulates the parts of the cortex involved with the planning of a movement. Parkinson’s Disease In Parkinson’s disease, the pars compacta of the subsatntia nigra does not stimulate the striatum as much (due to problem with SNc or dopamine receptors on the striatum) and the thalamus is inhibited resulting in its inability to stimulate the pemotor/supplementary motor areas (PMA/SMA) of the cortex. Symptoms of Parkinson’s Disease Bradykinesia-sloweness of movements. o Difficulty in small movements: doing up buttons, handling a knife o Face hypomimic (expressionless, mask-like) o Akinesia- difficulty in the initiation of movements. Needs external sensory triggers to initiate movement: e.g. a visual trigger because cannot initiate movements internally. Tremor at rest - usually starts in one hand (asymmetry) “pill rolling” tremor, tends to spread with time to other parts of the body. Rigidity - (no to be confused with spasticity) a type of resistance to passive movements. To the physician passively moving the patient’s limb feels like bending a lead pipe- lead pipe rigidity Gait slow, small steps, reduced arm swing. Huntington’s Disease Huntington’s disease is caused by a defective “Huntington Gene” on chromosome 4. This results in the degradation of the spiny GABAergic neurons in the striatum. It is an autosomal dominant disease. Symptoms of Huntington’s Disease Choreic movements (Chorea): Rapid jerky involuntary movements of the body. o These normally affect the hands and face at first. o They can be masked into socially acceptable movements at first but they gradually increase over time and cause great distress to patients. Dementia develops later. Death usually after 10-15 years. Cerebellum It is divided horizontally into 3 lobes: - Anterior lobe - Posterior lobe - Flocculonodular lobe It is also vertically into 3 regions: - vermis - intermediate cerebellum - Deep cerebellum nuclei Superior cerebellar peduncle pon s Middle cerebellar peduncle Dentate nucleus interpose fastigi d al Inferior cerebellar peduncle l ateral cerebellum Purkinje cells Granule cell layer Parallel fibers magnified granule Mossy fibers Climbing fibers Purkinje cell To deep axons nuclei Layers of the Cerebellum: Molecular layer - Cell free – contains only axons and dendrites. Purkinje cell layer - Its axons are the only output of the cerebellum to the deep nuclei. Granule cell layer - Granule cells send the axons up to the molecular layer where they end in a T and run parallel to the surface- parallel fibers- and synapse with Purkinje cells. Mossy fibers : these are the inputs to the cerebellum: - 1. spinal cord - 2. vestibular nuclei - 3. brainstem reticular formation - 4. deep pontine nuclei. Climbing fibers - second source of input- from inferior olivary nuclei. Pathways Into and out of the Cerebellum There are 3 highways into and out of the cerebellum - the inferior, middle and superior cerebellar peduncles. There are 3 deep nuclei: Fastigal nucleus (involved in balance; has connections with vestibular and reticular nuclei) Interposed involved in voluntary movements with projections to the thalamus & red nucleus Dentate also involved in voluntary movements with projections to the thalamus & red nucleus There are 3 sources of input: Mossy fibres from the spinocerebellar pathways Climbing fibres from the inferior olive Mossy fibres from the pons bring information from the cerebral cortex and are known as corticopontine connections and cross over after synapsing at the pons Functions of the Cerbellar Divisions The cerebellum is involved in the co-ordination of movement. It compares what you thought you were going to do (according to the motor cortex) with what you are actually about to do (according to proprioceptive feedback). The Basic Circuit is the same in all parts of the cerebellum and has 3 parts to it: » Direct path – input projects directly to motor systems via deep cerebellar nuclei » Indirect side loop – mossy fibres input to granular cells through parallel fibres, to Purkinje cells and back to the cerebellar nuclei. This circuit is used to correct reflex responses Climbing fibres input – to Purkinje cells. This is the error detection input. This circuit is used for learning movements Vestibulo-cerebellum: - flocculonodular lobe Input: vestibular nuclei and vestibular nerve Output: Purkinje cell axons to legs, trunk, and eye muscles Function: It regulates gait and posture. It also coordinates head movements with eye movements. Disorders: a) ataxic gait:- wide based stance (looks drunk) b) imbalance when eyes closed (Romberg sign) c) nystagmus Spinocerebellum - vermis projects to fastigial nucleus - intermediate projects to interposed nucleus Input: spinal cord (somatosensory & muscle afferents) via dorsal and ventral spino-cerebellar tracts Output: Purkinje cells axons to fastigial and interposed nuclei and (via red nucleus, vestibular nuclei and reticular nuclei) to spinal cord. Function: tunes motor execution by adjusting muscle tone. Disorder: hypotonia Cerebrocerebellum - lateral cerebellum projects to dentate nuclei Input: from cerebral cortex via pontine nuclei (mossy fibers) and inferior olive (climbing fibers). Output: Purkinje cells axons to dentate nuclei and via thalamus to motor & premotor cerebral cortex. Function: tactics and coordination of skilled movements. Disorders: a) Inability to perform complex movements involving several muscle groups (dysmetria) b) Inability to coordinate rapid alternating movements (dysdiadochokinesia) c) Deficits are ipsilateral Ataxia The cerebellum is involved in co-ordinating movements and damage results in incurordination or ataxia. Lesions affect the same side of the body as the damage in the cerebellum and are related to functional areas. Flocculonodular lobe lesion results in impaired balance, but co-ordination is ok Vermus/intermediate area lesions such as from alcoholic cerebellar degeneration result in ataxia or proximal muscles and disorders of gait Lesions of the cerebellar hemispheres result in hypotonia and intention tremor, especially in distal muscles