Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Jatene procedure wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Immediate Hemodynamic Response of Patients
with Atrioventricular Block and Cardiac
Failure to Transvenous Pacing
By FREDARICK L. GOBEL, M.D., JOSE R. MEDINA, M.D.,
CLARENCE A. GUENTER, M.D., AND YANG WANG, M.D.
With the Technical Assistance of David P. Olds
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
SUMMARY
Immediate hemodynamic improvement in patients with complete heart block occurs
when the ventricular rate is increased by electrical pacing. During pacing, there is
reduction in the pulmonary artery wedge, right atrial, and left and right ventricular
filling pressures. The mean rate of ejection, stroke volume, and stroke work decreased
following pacing, whereas the ejection time per minute increased, and dye curves assumed a more normal configuration. Very little change was noted in the resting cardiac
output.
The paced heart is able to obtain greater increases in cardiac output, stroke volume,
and mean rate of ejection during exercise than when unpaced. In addition, pacing
tends to return elevated exercising filling pressures in the right and left ventricles toward
normal.
Additional Indexing Words:
Heart block
Hemodynamics
Exercise hemodynamics
Catheterization
IT IS well established that most symptomatic patients with complete heart block
improve clinically with cardiac pacing. There
have been few studies on the acute hemodynamic changes during electrical pacing or
specifically on patients in congestive failure,
with respect to left-sided pressure changes or
the exercise response. The present report consists of nine patients with atrioventricular
block studied by right and left heart catheterization before and immediately after
electrical pacing at rest and during exercise.
Pacing
had elevated filling pressures in either the right
left ventricle at rest or during exercise; most
of them had clinical evidence of congestive heart
failure. The ages ranged from 42 to 79 years.
There were four women and five men. Two
patients had atrioventricular block that varied
from 2:1 to complete heart block.- Seven patients
had unremitting complete heart block. Patient
2 had severe aortic insufficiency. None of the
patients had congenital or surgically induced
heart block.
or
Methods
Right and left heart catheterization was performed in each patient. A bipolar electrode catheter was introduced through an antecubital vein,
and the tip was positioned in the apex of the right
ventricle. Arterial catheters were positioned in the
left ventricle and the ascending aorta. The midchest level from the angle of Louis was used as
the zero reference.
An oscilloscopic photographic recorder* was
used for recording pressures and dye curves.
Material and Methods
Patients
All nine patients with atrioventricular block
From the Department of Medicine, University of
Minnesota Medical School, Minneapolis, Minnesota.
Supported by Grants 06314-04 and HE-5222 from
the National Institutes of Health, U. S. Public Health
Service and by the Minnesota Heart Association.
*Electronics for Medicine, White Plains, New York.
64
Circulation, Volume XXXIX, January 1969
65
HEMODYNAMIC RESPONSE TO TRANSVENOUS PACING
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
Statham P23 Db strain-gauge transducers were
used. The catheter-manometer-recording system
had an over-all frequency response flat to 15 to
25 cycles/sec.
Cardiac output was determined by the dyedilution technique with use of indocyanine
green* and a densitometer.t Dye was hand injected into the pulmonary artery as a 5-mg bolus
from a calibrated syringe. The ascending aorta
was the sampling site in all cases. Each patient
also had cardiac output determinations by the
Fick method. Electrical pacing was accomplished
with an external pulse generatort* Supine exercise
was carried out on a bicycle ergometer,§ having
a fixed workload. Studies at the idioventricular
rate preceded studies done during pacing. Twenty
minutes' recovery after exercise and' a 15-minute
period after pacing were allowed to elapse before
continuing the study.
Left ventricular minute work, in kg-m, was
calculated as the product of the cardiac output
(L/min), the planimeterized mean systolic aortic pressure (mm Hg), and 0.0144. The left ventricular stroke work, in g-m, was the product
of the stroke volume (ml), the mean systolic
aortic pressure and 0.0144. The ejection time
was determined from central aortic pressure tracing. The tension-time index was computed as the
product of the mean systolic aortic pressure and
the ejection time per beat or the ejection time
per minute and expressed as mm Hg seconds per
beat or mm Hg seconds per minute. Resistances
were calculated as the quotient of the mean
pressure and the cardiac output times 80, and
expressed as dynes sec cm-5. The mean rate of
ejection is the quotient of the stroke volume
and the ejection time per beat expressed in
milliliters per second.
Results
The unpaced ventricular rate varied between 30 and 45 beats/min at rest. Seven of
the nine patients were exercised. During unpaced exercise, patients 4 and 6, with varying
heart block, increased their ventricular rate
by 12 to 16 beats, respectively, whereas the
five patients with complete b rt block had an
average increase of 4 beats/miiin (range: 0 to
7 beats/min).
The cardiac output and cardiac index were
low throughout. The average resting cardiac
n
0ll
Co
0"0
-
o,
C100CI-
0
LO
0
.
'
.
c>
-C2D
Q
._,x w-z
Q
00
on=
m
COO
C.6 .6
.-~
r
0
oa
-.-
all,
3
V
-ea
t-
mC:)
bCocs:
CoCoN
.f~ .-~
-
-C
CO
n E
Qd a3.Zcl
once
t00b
C
toO
I-
C6 L6
C6
Ddi
_
to"0 00 N 0 Co COS
0
"00 kCl coC
COl
- 1- c:4O"0Co
C -l ~c -
el
20
on
0'
0
C0
N to CosCN Cl t Cl 00
to cO to Co to 0 Co to Co "
on
'0
v
on
Q)
a 0
0O.g
C'
"0 0 00 Cl 0 00 CO "t"
Co
[A)Can
on.
r--q
4.)
0
C)
P-4
4
el
E*
f
cl
N
OC O
oN
r
00 clto C
N NN N
COD
C
CZO to
to t 0C
t
no
-4
onCD
-4
Q.,con
_P
we~c
C.)
aM
a)
4
0)C)
N
x
rot
It
,c)
*0h
an
Co
Co
Cl
Cl
C
C0
"0
"0t
Co
e
C
b_{
°a
aD
3:1
c0
1--1
0
0
O
H~
-
¢,
Circulation, Volume XXXIX, January 1969
.o
Lo
on
~--
H-
O
H
- FI
Fi~
H-
LO
t-Nto
N
"I
q
H ~ \1
COC
C.0C. tD
ON
H
H
H
Q 11
4
-~-
O N
tII.
b
*Cardiogreen.
tWaters X-302.
tMedtronic, 5800. Minneapolis, Minnesota.
§Lanoog bicycle ergometer, with hyperbalic coupling.
C.
_.
c3
b.5
*a
4)5
On
-I--
,
t
C
N-
GOBEL ET AL.
66
Table 2
Stroke Volume Response to Cardiac Pactng
Stroke volume (ml/beat)
Rest
Change in stroke volume from rest to exercise
Unpaced
Paced
Change
Change
%
%
Change
(ml)
(ml)
Change
Exercise
Unpaced
(ml)
Paced
(ml)
%
Change
Unpaced
Paced
no.
(ml)
%
Change
1
2*
3
4
5
6
7
8
9
Mean
97
157
137
89
109
104
88
124
88
110
70
90
69
43
63
60
45
66
43
61
38
43
50
52
42
42
49
47
51
46
109
94
14
12
12
24
34
180
114
83
66
54
42
43
25
31
28
14
23
20
53
86
92
147
124
122
94
74
103
74
84
+9
20
30
40
27
-18
4
23
36
18
-17
5
19
41
17
34
29
37
31
27
57
64
56
72
51
Patient
(ml)
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
*Patient has severe aortic insufficiency and this reflects forward SV.
output for all nine patients was 4.1 L/min.
After electrical pacing, the cardiac output
rose to 4.8 L/min, which is not statistically
significant. Patient 2, with severe aortic insufficiency, had no increase in cardiac output
after increasing the ventricular rate, all others
had a slight increase. During unpaced exercise, the mean cardiac output was 4.9 L/min.
After increasing the ventricular rate the exercising cardiac output rose significantly to
6.3 L/min. (P<0.010), (table 1).
The stroke volume decreased by increasing
the ventricular rate both at rest and during
exercise (table 2). During, pacing, the mean
resting stroke volume decreased 46% (110 to
61 ml/beat); the mean exercising stroke volume decreased 27% (122 to 84 ml/beat).
The increase in stroke volume from rest to
exercise was greater after pacing. The mean
stroke volume increased 17% in response to
unpaced exercise, but, during pacing, the
mean stroke volume increased 51% in response
to exercise over the resting paced value.
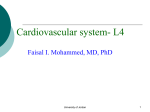
The left ventricular end-diastolic (LVED)
pressure decreased at rest in response to pacing in five of six patients in which it was
measured, the mean decreasing from 16.6
mm Hg to 10.2 mm Hg. During exercise
the LVED pressure was directly measured in
four patients and in each there was a reduction after pacing, the mean pressure decreasing from 21.3 to 15.3 mm Hg (fig. 1).
ac2,
28
24 _
20 _
CE
16
-j
12
8
4
-
Mean unpaced /6.6
/0.2
Mean poced
nl
0
20
40
60
80
0
20
40
60
80
100
Heori Rote (beoats/min)
Figure 1
Response of left ventricular end-diastolic (LVED)
pressure to electrical pacing.
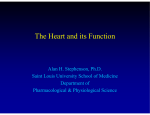
The resting pulmonary artery wedge
(PAW) pressure decreased consistently in
response to increasing the ventricular rate,
the mean pressure decreasing from 13.8 to 9.9
mm Hg. Duri-u- exercise the PAW pressure
was elevated in all six of the patients studied.
The exercising mean PAW pressure decreased
from 18.3 mm Hg to 14.0 mm Hg with pacing
(fig. 2).
The mean aortic pressure increased slightly
with increasing ventricular rates both at rest
and during exercise, the resting mean increased from 91 to 102 mm Hg and the exercising mean increased from 98 to 113 mm
Circahation, Volume XXXIX, Janzuary 1969
67
HEMODYNAMIC RESPONSE TO TRANSVENOUS PACING
Table 3
Changes in the Tension-time Index (TTI) in Response to Right Ventricular Pacing
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
1
2
3
4
5
6
7
8
9
Mean
Exercise
Rest
Exercise
Rest
Patient
no.
TTI/min
(mm Hg sec/min)
Exercise
Rest
Aortic mean systolic pressure
(mm Hg)
Ejection time
(sec/min)
U*
Pt
U
P
U
P
U
P
U
P
U
P
15
20
11
13
17
14
13
14
10
14
23
29
19
20
21
20
19
25
19
22
13
23
212
109
112
1787
1961
2267
2296
21
15
16
14
16
23
22
21
19
21
114
134
157
192
145
129
157
139
167
146
4050
3538
1739
1881
3323
2213
1717
2639
2394
2610
4876
130
114
2380
2538
1230
1152
2772
1642
1544
2102
1306
1852
2323
21
21
180
122
94
95
159
109
89
106
128
120
176
14
17
163
125
116
90
166
114
117
146
128
129
2428
2037
2543
2630
2244
2915
3391
2919
3123
3112
*Unpaced.
tPaced.
28
28,
REST
*
EXERCISE
MMean unpaced /0.5
6.3
Mean paced
24
24
6
/3,4
Mean unpoced
Mean paced
7.7
20-
20
77
E
E
16
E
E
12
4
-
3
73
- Mean
unpaced /38.
0
20
~
~
~
~
~~
6
8 h.<
Mean unpaced /8.3
/4.0
Meon paced
9.9
Mean poced
C)
~
EXERCISE
REST
4
~~
~
12
-~~~~~~~
~~~~~~8
_
16
(r
I,
40
60
80
o
20
40
60
4
80
1IU
0
20
40
6o
50
0
20
40
60
50
10o
Heart Rate (beats/min)
Heart Rate (beats/min)
Figure 2
Response of pulmonary artery wedge (PAW)
to electrical pacing.
9
Figure 3
pressure
Response of right ventricular end-diastolic (RVED)
pressure to electrical pacing.
Hg. The mean aortic systolic pressure, however, remained essentially unchanged in response to pacing at rest and during exercise
ercise. After increasing the ventricular rate,
the resting mean right atrial pressure decreased from 8.4 to 5.9 mm Hg; during exercise the mean right atrial pressure decreased from 10.9 to 6.7 mm Hg (fig. 4).
The mean pulmonary artery pressure did
not change appreciably at rest (18 mm Hg)
or during exercise (25 mm Hg) in response to
pacing.
Although there was a slight decrease in
the systemic and pulmonary resistance both
at rest and during exercise in response to
pacing, this was not statistically significant.
The resting mean systemic resistance decreased from 1,951 dynes sec cm-5 to 1,802
(table 3).
With the exception of one patient who did
not change during exercise (no. 7), the right
ventricular end-diastolic (RVED) pressure
decreased in all patients in response to electrical pacing both at rest and during exercise.
The resting mean RVED pressure decreased
from 10.5 to 6.3 mm Hg and during exercise
the mean RVED pressure decreased from 13.4
to 7.7 mm Hg during pacing (fig. 3).
The right atrial pressure consistently decreased in response to pacing at rest and exCirculation, Volume XXXIX, January 1969
68
GOBEL ET AL.
.70 r
.60
REST
k
EKERC/SE
.39
Meon unpoced
Mean paced
Mean unpaced .38
Mean paced
.28
.28
.50
E
.40
n
2
12
~~~~~~~2
9
.30_
5~~~~~~~
w0
6
.20_
.10
0
20
40
60
80
0
20
40
60
80
100
0
20
40
Heart Rate (beats/min)
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
cm-5 following pacing. The resting
mean pulmonary resistance decreased from
384 dynes sec cm-5 to 320 dynes sec cm-5
after pacing. The pulmonary arteriolar resistance changed inconsistently.
The ejection time per beat decreased with
pacing, but the ejection time per minute increased. The resting and exercise mean ejection time per beat decreased from 0.39 and
0.38 sec, respectively, to 0.28 sec after pacing. After pacing, however, with the increase
in heart rate the resting ejection time per
minute increased from 14.1 seconds per minute to a more nearly normal 21.6 seconds per
minute. An identical increase occurred during
exercise (figs. 5 and 6).
The mean rate of ejection per beat de-
no.
1.
2.
3.
4.
5.
6.
7.
8.
9.
Mean
SD
20
40
80
60
0oo
Figure 5
Response of aortic ejection time (AoET) to electrical
pacing.
32,
sec
Table 4
Mean Rate of Ejection per Beat (ml/sec)
Patient
0
Heart Rate (beats/min)
Figure 4
Response of right atrial (RA) pressure to electrical
pacing.
dynes
I_
IL
80
60
Rest
Unpaced
Paced
211
349
428
223
287
289
220
335
259
289
72
226
231
300
165
263
231
167
220
165
219
47
Exercise
Unpaced
Paced
266
294
28
24
2
.E
20
0
,
r
EXERCISE
RES T
Meon anpoced 14. /
Mean poced 2/. 6
4
Mean unpoced /5.8
Mean paced
2/.2
l-
0
20
40
60
80
0
20
40
60
s0
100
Heort Rote (beots/min)
Figure 6
Response of aortic ejection time (AoET) to electrical
pacing.
creased after pacing, both at rest and during
exercise (table 4). The increase in the exercising mean rate of ejection over the resting value was significantly greater following
pacing (219 ml/sec to 297 ml/sec; P <0.001).
Since the mr
aortic
systolic pressure
did
not change appreciably, the tension-time in474
292
319
244
226
242
408
335
320
92
324
247
367
285
297
44
dex per beat decreased in all patients in
response to electrical pacing both at rest and
during exercise. The tension-time index per
minute (TTI/ min) however, increased
all
patients both at rest and during exercise in
in
response to electrical pacing. The resting
mean TTI/min increased from 1,852 to 2,615
mm Hg sec, and the exercising mean value
Circeation, Volume XXXIX, January 1969
HEMODYNAMIC RESPONSE TO TRANSVENOUS PACING
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
increased from 2,244 to 3,112 mm Hg sec
after increasing the ventricular rate. These
changes are not statistically significant.
The resting mean left ventricular minute
work was 7.69 kg-m before pacing and 8.41
kg-m after pacing, which is not a significant
increase (P <0.55). The exercising mean left
ventricular minute work increased from 10.19
kg-m to 13.26 kg-m after pacing, which represented an increase in five of the seven patients studied (P < 0.095) (table 5).
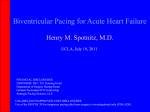
During pacing the left ventricular stroke
work decreased in all patients at rest. The
resting mean left ventricular stroke work decreased from 206.2 g-m/beat, to 106.7 g-m/
beat following pacing (P < 0.001). The exercising mean left ventricular stroke work decreased from 255.7 g-m/beat to 177.3 g-m/beat
during pacing (fig. 7).
69
280 rRest
240-
8
Exercise
* U.piced
200
160_
, E
8
2oL
,/
;
80-
W1
40
0
d z
-.--- _
0
8
16
24
32
0
8
16
24
Relationship of left ventricular stroke work and left
ventricular end-diastolic pressure in response to electrical pacing.
rate within
the physiological
range
ular rate from the idioventricular rate to
70 to 80 beats/min. This may in part be due
to severe myocardial decompensation or to
the fact that these were acute studies, since
cerebral, renal and cardiorespiratory function
clinically improves with the time following
pacing.7 The cardiac output reached after 15
minutes of pacing is thought likely to have
reached a plateau, as judged by the studies
been apparent for years, despite relatively
small changes usually seen in cardiac output.1-6 A few patients, however, may increase their cardiac output up to 50% when
the heart rate is increased from the idioventricular rate to more normal levels." 3 5 Little
change in cardiac output has been demonstrated by increasing the resting ventricular
'able 5
External WVork in Response to Cardiac Pacing
LVMW (kg-m)
no.
1.
2.
3.
4.
5.
6.
7.
8.
9.
LVSW (g-m)
Exercise
Exercise
Rest
U*
Pt
U
P
U
P
U
P
7.22
12.59
7.23
3.69
11.63
6.81
13.17
11.96
7.52
4.41
12.85
7.35
4.13
8.52
5.81
8.41
3.50
8.98
20.68
286.0
10.34
8.05
334.1
187.7
129.4
106.4
7.93
7.08
14.71
12.51
13.57
177.6
156.9
94.8
59.4
141.4
93.3
57.5
99.3
80.0
106.7
42.6
277.0
11.91
8.19
224.1
282.4
230.5
114.8
259.2
171.8
147.3
262.1
163.2
206.2
58.6
140.7
176.8
332.2
341.7
255.7
85.6
171.3
165.8
204.8
176.7
4.99
10.17
4.86
Mean 7.69
SD
3.13
10.19
2.86
12.11
15.27
12.83
13.26
4.01
177.3
57.8
Abbreviations: LVMW = left ventricular minute work; LVSW = left ventricular stroke work.
*Unpaced
tPaced.
Circulation, Volume XXXIX, January 1969
(70 to
110 beats/min). In our group of patients,
little change in the uniformly low cardiac
outputs was noted by increasing the ventric-
That patients with atrioventricular block
improve clinically after electrical pacing has
Patient
40
Figure 7
Discussion
Rest
32
Left Ventricular End Diastolic Pressure
(m H1g)
GOBEL ET AL.
70
five patients by Sowton,5 which demonstrated that changes in cardiac output after
pacing occur rapidly and stabilize to the new
level in a few minutes. In our group, elevated
ventricular filling pressures decreased consistently after pacing, perhaps because of the
decrease in diastolic filling time. The pulmonary artery wedge pressure, and right atrial
pressure reflecting ventricular diastolic events
also decreased consistently following pacing
and this was frequently associated with a
volunteered statement that exercise and
breathing were easier. With pacing, the TTI/
beat decreases because the ejection time is
decreased with little change in mean systolic
aortic pressure. The TTI/min, however, inon
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
creases as
ejection time
per
minute increases.
With pacing, the TTI/min increased to about
the same extent as left ventricular work. If
one assumes that the TTI/min is an index of
myocardial oxygen consumption (MV02),
then the ratio of MVO2 to left ventricular
work shows little change.8 9
A striking change was noted in the contour
of the dye-dilution curves after pacing. At
the idioventricular rhythm the disappearance
slope of the curves was greatly prolonged
with a low peak concentration. After pacing,
the dye curves assumed a more normal configuration, with a steeper disappearance slope
and a higher peak concentration. Since the
cardiac output does not change appreciably,
this suggests that the dye was diluted in a
smaller mixing volume.
The ejection time and the mean rate of
ejection decrease in response to pacing and
appear to follow the normal pattern of response to a resting tachycardia as described
by Weissler and associates.10 This may be
due to a decrease in the velocity of contraction, perhaps secondary to a decreased ventricular end-diastolic volume.
In normal subjects, the stroke volume
changes very little in response to supine
exercise at increasing work loads,"' 12 while
in complete heart block the stroke volume increases
in
response
to mild exercise."' 12 In
this group of patients the stroke volume increased slightly in response to modest supine
exercise, but during pacing, the patients were
able to increase their stroke volume by 50%
in response to the same external work load.
The paced exercising cardiac output increased by 32% over that of unpaced exercise
at the same work load. In normal subjects the
velocity of contraction and mean rate of ejection per beat increase with exercise and there
is a decrease in end-diastolic volume.13' 14 In
the present study the increase in the exercising
mean rate of ejection over the resting value
was greater after pacing. This suggests that
during exercise, the paced myocardium is
able to respond to exercise with a greater increase in the velocity of contraction than
when unpaced.
One patient (no. 2) had severe aortic insufficiency and had a striking decrease in
his filling pressures following pacing with no
change in cardiac output or left ventricular
minute work. The systolik ejection period per
minute increased by 50% with pacing and
hence reduced the diastolic filling period
markedly.
References
1. JUDGE, R. D., WILSON, W. S.,
AND
SIEGEL, J. H.:
Hemodynamic studies in patients with implanted cardiac pacemakers. New Eng J Med
270: 1391, 1964.
2. JOHANSSON, B. W.: Complete heart block: Clinical, hemodynamic, and pharmacological
study in patient with and without artificial
pacemaker. Acta Med Scand 180: Suppl 451,
1966.
3. BEVEGARD, S., JOHNSON, B., KARLOF, I., LAGERGREN, H., AND SowTON, E.: Effect of changes
in ventricular rate on cardiac output and central pressures at rest and during exercise in
patients with artificial pacemakers. Cardiov
Res 1: 21, 1967.
4. SAMET, P., BERNSTEIN, W. H., MEDOW, A., AND
NATHAN, D. A.: Effect of alterations in ventricular rate on cardiac output in complete
heart block. Amer J Cardiol 1: 10, 1965.
5. SowTON, E.: Hemodynamic studies in patients
with artificial pacemakers. Brit Heart J 26:
737, 1964.
6. PADER, E., AND LEVY, H.: Clinical and electrocardiographic studies in complete heart block.
J Chronic Dis 19: 1101, 1966.
7. HUMPHRIEs, J. O., HINMAN, E. J., BERNSTEIN,
L., AND WALKER, W. G.: Effect of artificial
Circulation, Volume XXXIX, January 1969
HEMODYNAMIC RESPONSE TO TRANSVENOUS PACING
pacing of the heart on cardiac and renal
function. Circulation 36: 717, 1967.
8. GORLIN, R., COHEN, L. S., ELLIOTT, W. C.,
KLEIN, M. D., AND LANE, F. J.: Effect of
supine exercise on left ventricular volume and
oxygen consumption in man. Circulation 32:
361, 1965.
9. SARNOFF, S. F., BRAUNWALD, E., WELcH, G. H.,
CASE, R. B., STAINSBY, W. N., AND MAREX,
R.: Hemodynamic determinants of oxygen
consumption of the heart with special reference to the tension-time index. Amer J Physiol
192: 148, 1958.
10. WEISSLER, A. M., PEELERS, R. G., AND RoEMLL,
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
W. H.: Relationships between left ventricular ejection time, stroke volume and heart
rate in normal individuals and patients with
cardiovascular disease. Amer Heart J 62:
367, 1961.
Circoda:ion, Volume XXXIX, January 1969
71
1 1. CHAPMIAN, C. B., FISHER, J. N., AND SPROULE,
B. J.: Behavior of stroke volume at rest and
during exercise in human beings. J Clin Invest
39: 1208, 1960.
12. WANG, Y., MARSHALL, R. J., AND SHEPHERD,
J. T.: Effect of changes in posture and of
graded exercise on stroke volume in man. J
Clin Invest 39: 1051, 1960.
13. BRAUNWALD, E., FRYE, R. L., AND Ross, J.:
Studies on Starling's law of the heart: Determinants of the relationship between left ventricular end-diastolic pressure and circumference. Circulation Research 8: 1254, 1963.
14. BRAUNWALD, E., GOLDBLATT, A., HARRISON,
D. C., AND MASON, D. T.: Studies on cardiac
dimensions in intact, unanesthetized man: III.
Effects of muscular exercise. Circulation Research 13: 460, 1963.
Immediate Hemodynamic Response of Patients with Atrioventricular Block and
Cardiac Failure to Transvenous Pacing
FREDARICK L. GOBEL, JOSE R. MEDINA, CLARENCE A. GUENTER, YANG
WANG and David P. Olds
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
Circulation. 1969;39:64-71
doi: 10.1161/01.CIR.39.1.64
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1969 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://circ.ahajournals.org/content/39/1/64
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles
originally published in Circulation can be obtained via RightsLink, a service of the Copyright
Clearance Center, not the Editorial Office. Once the online version of the published article for
which permission is being requested is located, click Request Permissions in the middle column of
the Web page under Services. Further information about this process is available in the Permissions
and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/