Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
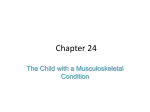
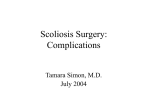
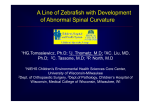
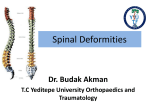
Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis Title Page Title: Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis: A Review of the Literature Type of Article: Review article Key words: Neuromuscular diseases, cerebral palsy, Duchenne muscular dystrophy, scoliosis, surgery, bracing, orthoses. Word Count: 3556 words Ethical approval: None required. Number of Figures: 10 (Fig. 1, Fig. 2a-d, Fig. 3a-d, Fig. 4) Number of Tables: 2 Number of References: 83 Authors: 1. Simon B Roberts ECAT Fellow/Specialist Registrar Trauma and Orthopaedics, 2. Athanasios I Tsirikos Consultant Orthopaedic and Spinal Surgeon Authors’ Institutional Address/Affiliations: University of Edinburgh/Scottish National Spinal Deformity Centre, Royal Hospital for Sick Children, Edinburgh, EH9 1LF, UK First Author: S B Roberts MBChB, BSc, MSc, MRCS(Ed); postal address - 12 Littlejohn Avenue, Edinburgh, EH10 5TG, UK; email - [email protected]; tel – 07832084911. Corresponding author: Mr Athanasios I Tsirikos; postal address - Scottish National Spinal Deformity Centre, Royal Hospital for Sick Children, Edinburgh, EH9 1LF, UK; email – [email protected]; tel – 0131 536 0784; fax – 0131 536 0924. 1 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis Abstract Neuromuscular scoliosis (NMS) is the second most prevalent spinal deformity (after idiopathic scoliosis) and is usually first identified during early childhood. Cerebral palsy (CP) is the most common cause of NMS, followed by Duchenne muscular dystrophy (DMD). Progressive spinal deformity causes difficulty with daily care, walking and sitting, and can lead to back and rib pain, cardiac and pulmonary complications, altered seizure thresholds, and skin compromise. Early referral to specialist spinal services and early diagnosis of NMS is essential to ensure appropriate multidisciplinary patient management. The most important goals for patients are preservation of function, facilitation of daily care, and alleviation of pain. Nonoperative management includes observation or bracing for less severe and flexible deformity in young patients as a temporising measure to provide postural support. Surgical correction and stabilisation of NMS is considered for patients with a deformity >40-50o, but may be performed for less severe deformity in patients with DMD. Postoperative intensive care, and early mobilisation and nutritional supplementation aim to minimise the rate of post-surgical complications, which are relatively common in this patient group. However, surgical management of NMS is associated with good longterm outcomes and high satisfaction rates for patients, their relatives and carers. 2 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis 1. Introduction Scoliosis is defined as a coronal plane spinal curvature of at least 10 degrees. A scoliotic deformity arising in the clinical setting of muscle imbalance due to an underlying neuropathic or myopathic disease can be diagnosed as neuromuscular scoliosis. Neuromuscular scoliosis is the second most prevalent spinal deformity, after idiopathic scoliosis. Patients with neuromuscular scoliosis frequently also have cardiac, gastrointestinal, and respiratory compromise in addition to other musculoskeletal and neurological disorders. Management of the scoliosis is therefore complex and requires careful multidisciplinary care. This review will focus on the diagnosis, management, and outcomes following the treatment of scoliosis in patients with neuromuscular conditions. 2. Epidemiology and Aetiology The incidence of scoliosis in the most common neuromuscular conditions is shown in Table 1. Cerebral palsy is the most prevalent cause of neuromuscular scoliosis, followed by Duchenne muscular dystrophy (DMD). Children with neuromuscular conditions develop spinal deformities due to a combination of poor muscular control across the trunk and pelvis, inherent muscle weakness, and occasionally spasticity. The abnormal curvature develops as a consequence of the effect of gravity on the vertebral column, which is inadequately supported due to generalised weakness of the posterior spinal and abdominal muscles during a period of accelerated skeletal growth. The degree of spinal deformity in these patients is therefore directly related to the degree of neuromuscular involvement and the child’s ambulatory ability. Wheelchair-bound growing patients with any underlying aetiology are much more likely to develop 3 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis scoliosis that demonstrates a high risk of rapid progression, and which often also affects the pelvis, than children who still retain walking capacity [1]. 3. Clinical Manifestations and Presentation 3.1. Types of Deformity Neuromuscular scoliotic deformities are generally first identified during early childhood. Initially, a flexible postural curve develops which is correctable with the patient lying flat or on suspension. This often progresses into a torsional rigid deformity during late child life and the pubertal growth and finally into a stiff curve of larger magnitude before growth is complete [1]. The typical curvature of neuromuscular scoliosis is a long, collapsing C-shaped curve affecting the thoracic and lumbar spine (Figure 1) [2]. The deformity often extends to include the pelvis, producing pelvic obliquity with the elevated one-half of the pelvis corresponding to the concave side (inside) of the curve. Asymmetric hip positioning due to hip contractures, subluxation or dislocation, as well as unbalanced function of the trunk and pelvic muscles may also cause pelvic deformity and accentuate the underlying scoliosis. If a severe scoliosis and pelvic obliquity co-exist with associated hip subluxation/dislocation, it is generally preferable to treat the spino-pelvic deformity first in order to produce a horizontal pelvis before surgical treatment to relocate the displaced femoral head within the dysplastic hip joint is planned. Finally, a kyphotic deformity with collapse of the trunk often in conjunction to the scoliosis is also common in neuromuscular conditions [3]. In contrast, isolated lumbar hyperlordosis or a severe lordoscoliosis is less frequent but produces major trunk imbalance, sitting intolerance and persistent pain, which necessitates surgical treatment [4]. 4 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis 3.2. Clinical signs and symptoms Deformity progression leads to significant trunk and spino-pelvic imbalance with consequent loss of function and increasing difficulty with daily care. Walking and sitting ability may become difficult, leading to pain or the patient becoming confined to bed. Rotation and shortening of the trunk occurs and can lead to compression of the heart and lungs, reduced mobility of the ribs and restriction of breathing capacity. If tilting of the pelvis develops, mechanical back or rib impingement pain can result, as well as cardiac or pulmonary complications. Feeding can also be affected and exacerbation of pre-existing swallowing disorders or gastro-oesophageal reflux can occur. Seizure activity may become worse due to uncontrolled pain. Asymmetrical loading in the area of the buttocks due to pelvic obliquity can cause pressure sores, especially in patients with impaired skin sensitivity (myelomeningocele, occasionally cerebral palsy) [1]. Many patients are also unable to articulate their symptoms, which can lead to a delay in presentation and diagnosis. Due to the universal progressive nature of neuromuscular scoliosis, early diagnosis of deformity is essential to optimise the multidisciplinary management. Early referral to specialist spinal centres of any patient with a neuromuscular condition and suspected spinal deformity is recommended. 4. Clinical Evaluation Patients with a neuromuscular scoliosis are initially assessed by clinical review in order to identify the severity of the spinal deformity followed by a systemic examination to identify associated co-morbidities or medical problems related to the development of the curve. Upper and lower limb function is assessed and evaluation of lower limb deformities is performed as these may contribute to the development of spino-pelvic 5 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis imbalance. Whole-spine postero-anterior and lateral radiographs are then performed. Sitting radiographs may be obtained if the patient is unable to stand. Supine x-rays in maximum traction can be useful to assess curve flexibility. Curve magnitude (as measured by the Cobb method) [5], spinal balance, pelvic obliquity, curve flexibility and curve progression are all closely monitored. An MRI scan of the whole spine is required if there is suspicion of intraspinal pathology. A patient with established neuromuscular scoliosis requires at least annual follow-up examination to assess curve progression, but more frequent reviews, usually every 6 months, are required during periods of rapid skeletal growth and for more severe or progressive curves. 5. Risk Factors for Disease Progression In general, there is a proportional relationship between the severity of neurological or myopathic involvement and curve severity, as well as the risk for deformity progression. For example, quadriplegic cerebral palsy typically causes a more severe and progressive scoliosis compared to hemiplegic or diplegic cerebral palsy. The progression of scoliosis in patients with cerebral palsy treated with intrathecal baclofen is not significantly different from cerebral palsy patients not receiving baclofen therapy [6]. For patients with DMD, later age at loss of walking ability and greater duration of corticosteroid therapy are related to later onset of scoliosis, whereas asymmetry of the hips and forced vital capacity at age 11-12 years are directly correlated with subsequent severity of scoliosis [7]. While the rate of curve progression is highly variable, the average progression for children with cerebral palsy has been reported as 0.8 degrees each year for curves that are less than 50 degrees and 1.4 degrees each year for curves that are more than 50 degrees [8]. During periods of rapid growth such as the pubertal growth spurt, much more rapid progression can occur, with curves increasing as much 6 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis as 2-4 degrees each month, resulting in rapid deterioration of spinal deformity and the patient’s function [9, 10]. 6. Nonoperative Management 6.1. Aims of Treatment Several factors need to be considered during the global planning of disease management in patients with neuromuscular scoliosis. The most important goals for patients are preservation of function, facilitation of daily care, and alleviation of pain. Nonoperative management of patients with neuromuscular spinal deformities should be directed at maximising sitting ability and postural control in order to facilitate motor function and interaction to the environment. Due to the lack of randomised controlled trials investigating treatment modalities for spinal deformity in neuromuscular patients, much of the management of neuromuscular scoliosis derives from results of cohort studies, comparative cohort studies, anecdotal evidence and expert opinion. Growing patients with mild, flexible curves can be managed by observation only. For patients with DMD, corticosteroids may delay the development and progression of scoliosis and may be considered for this purpose, though the optimal dosing regimen remains to be determined [11-14]. 6.2. Bracing If progression of neuromuscular scoliosis occurs, bracing may be considered. It is generally accepted that spinal bracing is ineffective in significantly altering progression of deformity in patients with neuromuscular disease. Although bracing may not ultimately prevent the need for surgical intervention, bi-valved or soft full-body contact thoraco-lumbo-sacral braces can be used in patients in whom surgery is contra- 7 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis indicated or declined, and in young children with small, flexible curves. In these circumstances, bracing can help to manage the spinal deformity by providing postural support, maintaining sitting position, improving muscle balance, and augmenting function, while permitting further growth to occur prior to surgical intervention [1517]. Furthermore, bracing may limit complications such as impaired pulmonary development, and therefore reduce the risks associated with any future surgery [3]. However, bracing is often ineffective due to shortening duration of brace wear, skin irritation, and respiratory problems, as well as the aggressive nature of the deformity. Cognitive impairment associated with cerebral palsy may also reduce a patient’s tolerance of bracing. It is important that the potential advantages, disadvantages, and expected outcomes of bracing are clearly understood by the patients, their family and carers if it is used [9, 18]. 6.3. Orthotics Wheelchair adaptations can be used in addition to, or as an alternative to, bracing. These adaptations include offset lateral chest supports, shoulder/waist harnesses, modular seating systems, and moulded shells. The latter permit the patient to lie and be tilted, and may be better tolerated than braces, are simple to use for carers, permit free access to the abdomen if gastrostomy feeding is required, and do not restrict respiratory movements, which is particularly important for children at high risk for chest infections [15]. There is conflicting evidence regarding the role of knee-ankle-foot orthoses in prolonging functional walking, and any association with subsequent progression of scoliosis. Therefore knee-ankle-foot orthoses cannot be recommended for the purpose of preventing development or progression of scoliosis in neuromuscular patients [19, 8 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis 20]. Braces and orthoses that protect all functions are not available, and therefore their selection and use must be tailored to the needs of each individual patient. 6.4. Physiotherapy Physiotherapy, including regular stretching, is widely performed and important in the general care of neuromuscular patients, but does not improve any aetiological factors for neuromuscular scoliosis or prevent progression of an established scoliosis. Physiotherapy can be helpful to prevent any adverse effects from prolonged brace use, prevent the onset of joint contractures, and maintain both chest mobility and respiratory excursion [21]. 6.5. Other Non-operative Treatments There is no evidence to support electrical stimulation or botulinum toxin injections to manage spinal deformity in patients with neuromuscular conditions. The use of lycra suits may be beneficial in patients who retain some degree of muscle function and who develop small and flexible postural curves as an alternative to a conventional brace due to the fact that they are usually better tolerated and in order to stimulate upright posture and preserve function [22]. 7. Operative Management 7.1. Aims of Surgical Intervention The decision to proceed with operative correction and stabilisation of neuromuscular scoliosis is dependent on individual patient-specific factors, in particular the nature of the underlying neuromuscular condition and the patient’s current level of function. The patient’s individual needs, overall medical state and long-term prognosis of the 9 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis underlying neuromuscular condition have to be taken into account and the decision for scoliosis surgery has to be individualised and discussed thoroughly with the patients and their families. For higher-functioning patients, operative intervention aims to provide a more normal spinal balance and alter the progression of disease with the goal of preserving function with respect to ambulatory capacity. In wheelchair-dependent patients, the aim is to maintain sitting independence, promote more physiological respiratory and gastrointestinal functioning, and facilitate overall care [23]. 7.2. Indications for Surgery and Surgical Techniques In general, surgical intervention is considered for patients with a curve greater than 40 or 50 degrees and significant deterioration in function (Figure 2). Such curves will deteriorate even after the patients have completed their skeletal growth. An exception to this is DMD scoliosis in which, due to the natural history of the disease, surgery is considered for progressive spinal curvatures greater than 25 degrees in order to prevent respiratory compromise produced by the deformity. Surgical treatment will aim to correct the spinal deformity and pelvic obliquity, restore coronal and sagittal spinal balance, and achieve a solid spinal fusion. This is usually performed using a posterior surgical approach to the spine, with instrumentation to correct the curvatures, and autologous and allograft bone to achieve a bony fusion [24-26]. This typically results in up to 75-80% overall correction of deformity [27-29]. For patients with severe curves, which may be permitted to develop in patients with cerebral palsy, the challenge is to manage spinal growth while controlling the deformity. For curves of 60-90 degrees magnitude, surgery is considered when the deformity becomes stiff on clinical and radiographic examination. If the spine remains flexible, surgery may be delayed until the curve reaches approximately 90 degrees of magnitude, and this can usually be 10 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis corrected by posterior spinal fusion in the advent of modern segmental pedicle screw instrumentation techniques (Figure 3). For stiff curves or those greater than 90 degrees with fixed pelvic obliquity, surgical release and fusion of the anterior column of the spine may be required to increase flexibility of the deformity and allow for better correction in addition to posterior spinal fusion; this combined procedure increases the potential morbidity and complications associated with surgery. The instrumentation and fusion of the deformity in neuromuscular scoliosis usually extends from the upper thoracic spine (T2 vertebra) proximally to the sacrum/pelvis distally as this prevents the development of recurrent deformities above and below the instrumentation that can occur with further skeletal growth if a shorter fusion is performed [26, 30-33]. In the absence of significant pelvic deformity the lower lumbar spine may be selected as the lower extent of the spinal fusion to preserve the patient’s lumbosacral flexibility [34, 35]. Growth preservation techniques (growing rods) may be considered in young patients with severe but flexible curves as a temporising measure spanning the levels of the deformity across the spine and often extending down to the pelvis. The benefits of preserving spinal growth and delaying the need of the definitive spinal fusion for a later age have to be balanced over the considerable risk of major complications in the need of serial operations which is increased due to the underlying medical co-morbidities and inherent bone weakness. Control of scoliosis and spinal growth with growing rod surgery has been reported as an effective strategy in patients with spinal muscular atrophy [36]. 11 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis 8. Perioperative Care 8.1. Perioperative Risks and Preoperative Planning The risks associated with surgery for neuromuscular scoliosis are correlated with the severity of neurological impairment and associated co-morbidities. Factors that are strongly associated with increased risk of postoperative complications include non-oral feeding, severe cognitive impairment, inability to communicate vocally, presence of seizures, and non-independent sitting ability. As patients with neuromuscular disease often have varied and complex medical conditions, pre-operative assessment requires a multidisciplinary involvement. In particular, it is important to recognise and optimise any seizure activity, cardio-respiratory problems, gastro-intestinal reflux or dysmotility, feeding and nutritional difficulties. As the risk of surgery is greatly increased by cardiac dysfunction or arrhythmias associated with DMD, pre-operative assessment by a paediatric cardiologist and anaesthesiologist is mandatory [37]. Preoperative pulmonary function tests positively correlate with the incidence of postoperative pulmonary complications, with values below 30-40% of predicted vital capacity providing the best indication of a high risk of major postoperative respiratory complications [38]. Spinal stabilisation can, however, be performed safely in patients with low vital capacity and those with pre-existing respiratory failure requiring nocturnal non-invasive ventilation [39, 40]. The use of preoperative non-invasive ventilation may be helpful for patients with forced vital capacity less than 40% of predicted values or dependent on arterial blood gas results. Further specific anaesthetic measures beneficial in the peri-operative management of patients with neuromuscular scoliosis include hypotensive anaesthesia, use of cell salvage, tranexamic acid, haemodilution, haemodynamic monitoring, and careful 12 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis maintenance of normothermia [41-44]. A summary of preoperative investigations for neuromuscular patients undergoing spinal stabilisation is provided in Table 2. To protect function, spinal cord monitoring is performed intra-operatively with transcranial motor and somatosensory evoked potentials for patients who are ambulatory, can stand, or have purposeful lower extremity movement or for those patients with normal bladder and bowel function. Spinal cord monitoring is therefore utilised intra-operatively for patients with muscular causes and mild cerebral palsy, but may not be appropriate, for example, in patients with severe quadriplegic cerebral palsy or severe spinal cord dysfunction. When performed together, transcranial motor and somatosensory evoked potentials have 95-100% reliability and permit motor function testing intra-operatively and adaptation of recording sites to the relevant motor function for each patient [45-47]. Patients, family and caregivers should be fully informed regarding the potential for prolonged and complex intensive care and in-patient stay postoperatively (additional education resources are shown in Figure 4). Furthermore, resuscitation decision-making should also be discussed preoperatively with the patient and their family as appropriate. 8.2. Postoperative Care Patients may remain in an intensive care unit, often still intubated, for several days postoperatively, for close monitoring of cardio-respiratory and haemodynamic status, before returning to standard ward care. The required duration of postoperative ventilation is determined individually and is usually no more than 36 hours. Early reinstigation of nutritional intake, often with the use of nasogastric, nasojejunal or gastrostomy tubes and nutritional supplementation, is important in the postoperative period. This is particularly important perioperatively for patients with cerebral palsy 13 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis who are often malnourished prior to surgery [48]. Patients are encouraged to mobilise out of bed or in a wheelchair as soon as medically safe following surgery. Patients are usually able to mobilise using a wheelchair by day 2-5 postoperatively [42, 49]. Adjustments to patients’ wheelchairs can also be made during this period as necessary and by assessment of an orthotist. Patients are usually advised to avoid rotation of the spine or flexion of the hips beyond 90 degrees for 4-6 months postoperatively, and appropriate techniques are learnt with the assistance of a physiotherapist. Consideration should be given to the need of a hoist for patient transfers during subsequent rehabilitation. Postoperative trunk support in the form of a brace is usually not required following the use of modern spinal stabilisation techniques. Following discharge, children can usually return to school within 3-4 weeks. 9. Outcomes of Treatment 9.1. Patient Satisfaction and Quality of Life With modern medical care, the life expectancy of patients with complex neuromuscular conditions has been considerably prolonged. Therefore, treatment of their spinal deformities is now becoming a greater necessity in order to maintain functional abilities and preserve quality of life. For patients with severe neuromuscular disease, careful consideration must be given on whether or not the risks of an extensive surgical procedure in the presence of complex medical problems outweigh any anticipated benefits. Surveys following surgical correction for patients with total-bodyinvolvement spastic cerebral palsy and scoliosis demonstrated that 85-96% of parents and caregivers are satisfied with the outcomes for the patient after surgery and would choose the procedure again [29, 50, 51]. Surgery resulted in improved sitting ability, function, activities of daily living, physical appearance, comfort, ease of care, and self- 14 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis image [52-55]. Such improvements may positively affect quality of life for these patients, which is important as the mean patient survival following surgical correction for scoliosis secondary to severe cerebral palsy has been reported as 11.2 years [56]. Similar satisfaction rates have been demonstrated in surveys of patients treated for DMD scoliosis, who also report improvements in breathing, digestion and posture postoperatively [57]. In DMD scoliosis, early surgical correction improves the deformity, and may have a positive impact on survival [58, 59]. 9.2. Effect of Surgical Intervention on Respiratory Function Prior to surgery, patients with neuromuscular disease and scoliosis have lower pulmonary function parameters than those without scoliosis and healthy controls [60]. In a prospective study including neuromuscular patients, pulmonary function declined up to 60% immediately following surgery, reaching a nadir at 3 days postoperatively, but returning to preoperative values between 1 and 2 months after surgery [61]. One year following spinal stabilisation, peak cough flow and end tidal CO2 measurements are reportedly well maintained in neuromuscular patients [62]. However, the long-term effect of surgical stabilisation of scoliosis on respiratory function is incompletely understood and existing evidence is conflicting, with studies reporting both no difference in subsequent rate of decline and other studies indicating a reduced rate of decline in respiratory function [63-69]. The effect of spinal stabilisation on gastric emptying, upper gastrointestinal symptoms and clinical nutritional state has been reported as minimal [70]. 9.3. Complications of Treatment 15 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis The incidence of complications following surgical correction of neuromuscular scoliosis has been estimated as ranging from 18% to 68%. Complications should therefore be actively anticipated, especially in patients with DMD who have higher overall rates [71, 72]. Non-ambulatory status and severe preoperative curve magnitude greater than 60o are associated with increased risk for major postoperative complications [73]. The most common complications include superficial and deep wound infections (13.1%), non-surgical site infections (10%), pseudoarthrosis, (1.9%), problematic instrumentation (3.4%), and pulmonary/respiratory complications (19.4%) [42, 74-76]. The most frequent postoperative complication in patients with cerebral palsy is pulmonary infection, with a particular risk of aspiration pneumonia. Pulmonary complications are also common following surgical correction in patients with DMD; postoperative atelectasis is relatively frequent in DMD patients, and the incidence of pulmonary infection has been estimated at 7-8% [62, 72]. Wound infections also occur at a similar frequency in patients with DMD, but are less common in patients with cerebral palsy [72, 77]. In patients with spinal cord dysfunction, particular care must be given to surgical site and general skin pressure management due to insensate skin, and also to care of the urinary system to avoid urosepsis. Other recognised complications include postoperative ileus, pancreatitis, and superior mesenteric artery syndrome, while neurological complications are rare [78]. However, surgical complications rarely cause any permanent problem for the patient or caregivers, but rather extend the need for inpatient care. Indeed, the mean hospital stay 16 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis for surgical correction of neuromuscular scoliosis can be prolonged and this has been previously reported as between 14 and 19.6 days [42, 56]. 10. Conclusion Scoliosis is common in patients with neuromuscular conditions. The spinal deformity is progressive and can lead to loss of ambulation, difficulty sitting, feeding disorders, pain, poor self-image, and increasing difficulty with daily care. Non-operative treatment cannot control the deformity but may be used while significant spinal growth remains. Early referral of patients with neuromuscular conditions and suspected spinal deformity to specialist spinal centres is essential to optimise the multidisciplinary management and long-term outcomes. Surgical correction and stabilisation of the spinal deformity is effective, but it is associated with significant risks that are usually manageable. Surgical management of neuromuscular scoliosis is associated with good long-term outcomes and high satisfaction rates among patients, their families and caregivers. Acknowledgements Both authors contributed to the design and writing of the article. The authors have no relevant interests to declare. This study has no conflict of interest. No funding was received for this work. 17 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis References 1. Tsirikos AI. Development and treatment of spinal deformity in patients with neurological or myopathic conditions. Orthopaedics and Trauma. 2011;25(6):425-34. 2. Lonstein JE, Akbarnia A. Operative treatment of spinal deformities in patients with cerebral palsy or mental retardation. An analysis of one hundred and seven cases. The Journal of bone and joint surgery American volume. 1983;65(1):43-55. 3. Vialle R, Thevenin-Lemoine C, Mary P. Neuromuscular scoliosis. Orthopaedics & traumatology, surgery & research : OTSR. 2013;99(1 Suppl):S124-39. 4. Karampalis C, Tsirikos AI. The surgical treatment of lordoscoliosis and hyperlordosis in patients with quadriplegic cerebral palsy. The bone & joint journal. 2014;96-B(6):800-6. 5. Cobb JR. Outline for the study of scoliosis. Instructional course lectures. 5: Ann Arbor: JW Edwards; 1948. 6. Shilt JS, Lai LP, Cabrera MN, Frino J, Smith BP. The impact of intrathecal baclofen on the natural history of scoliosis in cerebral palsy. Journal of pediatric orthopedics. 2008;28(6):684-7. 7. Kinali M, Main M, Eliahoo J, Messina S, Knight RK, Lehovsky J, et al. Predictive factors for the development of scoliosis in Duchenne muscular dystrophy. European journal of paediatric neurology : EJPN : official journal of the European Paediatric Neurology Society. 2007;11(3):160-6. 8. Thometz JG, Simon SR. Progression of scoliosis after skeletal maturity in institutionalized adults who have cerebral palsy. The Journal of bone and joint surgery American volume. 1988;70(9):1290-6. 18 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis 9. Miller A, Temple T, Miller F. Impact of orthoses on the rate of scoliosis progression in children with cerebral palsy. Journal of pediatric orthopedics. 1996;16(3):332-5. 10. Saito N, Ebara S, Ohotsuka K, Kumeta H, Takaoka K. Natural history of scoliosis in spastic cerebral palsy. Lancet. 1998;351(9117):1687-92. 11. Alman BA, Raza SN, Biggar WD. Steroid treatment and the development of scoliosis in males with duchenne muscular dystrophy. The Journal of bone and joint surgery American volume. 2004;86-A(3):519-24. 12. Yilmaz O, Karaduman A, Topaloglu H. Prednisolone therapy in Duchenne muscular dystrophy prolongs ambulation and prevents scoliosis. European journal of neurology : the official journal of the European Federation of Neurological Societies. 2004;11(8):541-4. 13. Manzur AY, Kuntzer T, Pike M, Swan A. Glucocorticoid corticosteroids for Duchenne muscular dystrophy. The Cochrane database of systematic reviews. 2008(1):CD003725. 14. Lebel DE, Corston JA, McAdam LC, Biggar WD, Alman BA. Glucocorticoid treatment for the prevention of scoliosis in children with Duchenne muscular dystrophy: long-term follow-up. The Journal of bone and joint surgery American volume. 2013;95(12):1057-61. 15. Kotwicki T, Jozwiak M. Conservative management of neuromuscular scoliosis: personal experience and review of literature. Disability and rehabilitation. 2008;30(10):792-8. 16. Duport G, Gayet E, Pries P, Thirault C, Renardel-Irani A, Fons N, et al. Spinal deformities and wheelchair seating in Duchenne muscular dystrophy: twenty years of research and clinical experience. Seminars in neurology. 1995;15(1):29-37. 19 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis 17. Heller KD, Forst R, Forst J, Hengstler K. Scoliosis in Duchenne muscular dystrophy: aspects of orthotic treatment. Prosthetics and orthotics international. 1997;21(3):202-9. 18. Terjesen T, Lange JE, Steen H. Treatment of scoliosis with spinal bracing in quadriplegic cerebral palsy. Developmental medicine and child neurology. 2000;42(7):448-54. 19. Rodillo EB, Fernandez-Bermejo E, Heckmatt JZ, Dubowitz V. Prevention of rapidly progressive scoliosis in Duchenne muscular dystrophy by prolongation of walking with orthoses. Journal of child neurology. 1988;3(4):269-74. 20. Bakker JP, de Groot IJ, Beckerman H, de Jong BA, Lankhorst GJ. The effects of knee-ankle-foot orthoses in the treatment of Duchenne muscular dystrophy: review of the literature. Clinical rehabilitation. 2000;14(4):343-59. 21. Ferrari A, Ferrara C, Balugani M, Sassi S. Severe scoliosis in neurodevelopmental disabilities: clinical signs and therapeutic proposals. European journal of physical and rehabilitation medicine. 2010;46(4):563-80. 22. Matthews M, Crawford, R. The use of dynamic Lycra orthosis in the treatment of scoliosis: a case study. Prosthetics and orthotics international. 2006;30(2):174-81. 23. Mehta JS, Gibson, M.J. The treatment of neuromuscular scoliosis. Current Orthopaedics. 2003;17:313-21. 24. Brown JC, Zeller JL, Swank SM, Furumasu J, Warath SL. Surgical and functional results of spine fusion in spinal muscular atrophy. Spine. 1989;14(7):76370. 25. Aprin H, Bowen JR, MacEwen GD, Hall JE. Spine fusion in patients with spinal muscular atrophy. The Journal of bone and joint surgery American volume. 1982;64(8):1179-87. 20 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis 26. Miller F, Moseley CF, Koreska J. Spinal fusion in Duchenne muscular dystrophy. Developmental medicine and child neurology. 1992;34(9):775-86. 27. Westerlund LE, Gill SS, Jarosz TS, Abel MF, Blanco JS. Posterior-only unit rod instrumentation and fusion for neuromuscular scoliosis. Spine. 2001;26(18):19849. 28. Tsirikos AI, Mains E. Surgical correction of spinal deformity in patients with cerebral palsy using pedicle screw instrumentation. Journal of spinal disorders & techniques. 2012;25(7):401-8. 29. Tsirikos AI, Lipton G, Chang WN, Dabney KW, Miller F. Surgical correction of scoliosis in pediatric patients with cerebral palsy using the unit rod instrumentation. Spine. 2008;33(10):1133-40. 30. Errico TJ, Petrizzo, A. Introduction to Spinal Deformity. In: Errico TJ, Lonner, B. S., Moulton, A. W., editor. Surgical Management of Spinal Deformities. Philadelphia: Elsevier; 2009. p. 3-12. 31. Tsirikos AI, Chang WN, Shah SA, Dabney KW, Miller F. Preserving ambulatory potential in pediatric patients with cerebral palsy who undergo spinal fusion using unit rod instrumentation. Spine. 2003;28(5):480-3. 32. Gaine WJ, Lim J, Stephenson W, Galasko CS. Progression of scoliosis after spinal fusion in Duchenne's muscular dystrophy. J Bone Joint Surg Br. 2004;86(4):5505. 33. Alman BA, Kim HK. Pelvic obliquity after fusion of the spine in Duchenne muscular dystrophy. J Bone Joint Surg Br. 1999;81(5):821-4. 34. Sengupta DK, Mehdian SH, McConnell JR, Eisenstein SM, Webb JK. Pelvic or lumbar fixation for the surgical management of scoliosis in duchenne muscular dystrophy. Spine. 2002;27(18):2072-9. 21 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis 35. Mubarak SJ, Morin WD, Leach J. Spinal fusion in Duchenne muscular dystrophy--fixation and fusion to the sacropelvis? Journal of pediatric orthopedics. 1993;13(6):752-7. 36. Chandran S, McCarthy J, Noonan K, Mann D, Nemeth B, Guiliani T. Early treatment of scoliosis with growing rods in children with severe spinal muscular atrophy: a preliminary report. Journal of pediatric orthopedics. 2011;31(4):450-4. 37. Wollinksy KH, Weiss, C., Gelowicz-Maurer, M., Geiger, P., Mehrkens, H.H., Naumann, T. Preoperative risk assessment of children with Duchenne muscular dystrophy and relevance for anesthesia and intra- and postoperative course. Med Klin (Munich). 1996;91(Suppl 2):34-7. 38. Kang GR, Suh SW, Lee IO. Preoperative predictors of postoperative pulmonary complications in neuromuscular scoliosis. Journal of orthopaedic science : official journal of the Japanese Orthopaedic Association. 2011;16(2):139-47. 39. Harper CM, Ambler G, Edge G. The prognostic value of pre-operative predicted forced vital capacity in corrective spinal surgery for Duchenne's muscular dystrophy. Anaesthesia. 2004;59(12):1160-2. 40. Gill I, Eagle M, Mehta JS, Gibson MJ, Bushby K, Bullock R. Correction of neuromuscular scoliosis in patients with preexisting respiratory failure. Spine. 2006;31(21):2478-83. 41. Milne B, Rosales JK. Anaesthetic considerations in patients with muscular dystrophy undergoing spinal fusion and Harrington rod insertion. Canadian Anaesthetists' Society journal. 1982;29(3):250-4. 42. Benson ER, Thomson JD, Smith BG, Banta JV. Results and morbidity in a consecutive series of patients undergoing spinal fusion for neuromuscular scoliosis. Spine. 1998;23(21):2308-17; discussion 18. 22 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis 43. Fox HJ, Thomas CH, Thompson AG. Spinal instrumentation for Duchenne's muscular dystrophy: experience of hypotensive anaesthesia to minimise blood loss. Journal of pediatric orthopedics. 1997;17(6):750-3. 44. Larsen UT, Juhl B, Hein-Sorensen O, de Fine Olivarius B. Complications during anaesthesia in patients with Duchenne's muscular dystrophy (a retrospective study). Canadian journal of anaesthesia = Journal canadien d'anesthesie. 1989;36(4):418-22. 45. Owen JH, Sponseller PD, Szymanski J, Hurdle M. Efficacy of multimodality spinal cord monitoring during surgery for neuromuscular scoliosis. Spine. 1995;20(13):1480-8. 46. DiCindio S, Theroux M, Shah S, Miller F, Dabney K, Brislin RP, et al. Multimodality monitoring of transcranial electric motor and somatosensory-evoked potentials during surgical correction of spinal deformity in patients with cerebral palsy and other neuromuscular disorders. Spine. 2003;28(16):1851-5; discussion 5-6. 47. Langeloo DD, Journee HL, Polak B, de Kleuver M. A new application of TCE- MEP: spinal cord monitoring in patients with severe neuromuscular weakness undergoing corrective spine surgery. Journal of spinal disorders. 2001;14(5):445-8. 48. Perenc L, Przysada G, Trzeciak J. Cerebral Palsy in Children as a Risk Factor for Malnutrition. Ann Nutr Metab. 2015;66(4):224-32. 49. Cotton LA. Unit rod segmental spinal instrumentation for the treatment of neuromuscular scoliosis. Orthop Nurs. 1991;10(5):17-23. 50. Comstock CP, Leach J, Wenger DR. Scoliosis in total-body-involvement cerebral palsy. Analysis of surgical treatment and patient and caregiver satisfaction. Spine. 1998;23(12):1412-24; discussion 24-5. 23 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis 51. Legg J, Davies E, Raich AL, Dettori JR, Sherry N. Surgical correction of scoliosis in children with spastic quadriplegia: benefits, adverse effects, and patient selection. Evidence-based spine-care journal. 2014;5(1):38-51. 52. Bulman WA, Dormans JP, Ecker ML, Drummond DS. Posterior spinal fusion for scoliosis in patients with cerebral palsy: a comparison of Luque rod and Unit Rod instrumentation. Journal of pediatric orthopedics. 1996;16(3):314-23. 53. Sussman MD, Little D, Alley RM, McCoig JA. Posterior instrumentation and fusion of the thoracolumbar spine for treatment of neuromuscular scoliosis. Journal of pediatric orthopedics. 1996;16(3):304-13. 54. Larsson EL, Aaro SI, Normelli HC, Oberg BE. Long-term follow-up of functioning after spinal surgery in patients with neuromuscular scoliosis. Spine. 2005;30(19):2145-52. 55. Ersberg A, Gerdhem P. Pre- and postoperative quality of life in patients treated for scoliosis. Acta orthopaedica. 2013;84(6):537-43. 56. Tsirikos AI, Chang WN, Dabney KW, Miller F, Glutting J. Life expectancy in pediatric patients with cerebral palsy and neuromuscular scoliosis who underwent spinal fusion. Developmental medicine and child neurology. 2003;45(10):677-82. 57. Suk KS, Lee BH, Lee HM, Moon SH, Choi YC, Shin DE, et al. Functional outcomes in Duchenne muscular dystrophy scoliosis: comparison of the differences between surgical and nonsurgical treatment. The Journal of bone and joint surgery American volume. 2014;96(5):409-15. 58. Galasko CS, Delaney C, Morris P. Spinal stabilisation in Duchenne muscular dystrophy. J Bone Joint Surg Br. 1992;74(2):210-4. 24 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis 59. Bentley G, Haddad F, Bull TM, Seingry D. The treatment of scoliosis in muscular dystrophy using modified Luque and Harrington-Luque instrumentation. J Bone Joint Surg Br. 2001;83(1):22-8. 60. Inal-Ince D, Savci S, Arikan H, Saglam M, Vardar-Yagli N, Bosnak-Guclu M, et al. Effects of scoliosis on respiratory muscle strength in patients with neuromuscular disorders. The spine journal : official journal of the North American Spine Society. 2009;9(12):981-6. 61. Yuan N, Fraire JA, Margetis MM, Skaggs DL, Tolo VT, Keens TG. The effect of scoliosis surgery on lung function in the immediate postoperative period. Spine. 2005;30(19):2182-5. 62. Chong HS, Moon, E.S., Kim, H.S., Ankur, N., Park, J.O., Kim, J.Y., Kho, P.A.B., Moon, S.H., Lee, H.M., Seul, N.H. Comparison betwen operated muscular dystrophy and spinal muscular atrophy patients in terms of radiological, pulmonary and functional outcomes. Asian Spine Journal. 2010;4(2):82-8. 63. Miller F, Moseley CF, Koreska J, Levison H. Pulmonary function and scoliosis in Duchenne dystrophy. Journal of pediatric orthopedics. 1988;8(2):133-7. 64. Kennedy JD, Staples AJ, Brook PD, Parsons DW, Sutherland AD, Martin AJ, et al. Effect of spinal surgery on lung function in Duchenne muscular dystrophy. Thorax. 1995;50(11):1173-8. 65. Velasco MV, Colin AA, Zurakowski D, Darras BT, Shapiro F. Posterior spinal fusion for scoliosis in duchenne muscular dystrophy diminishes the rate of respiratory decline. Spine. 2007;32(4):459-65. 66. Galasko CS, Williamson JB, Delaney CM. Lung function in Duchenne muscular dystrophy. Eur Spine J. 1995;4(5):263-7. 25 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis 67. Jenkins JG, Bohn D, Edmonds JF, Levison H, Barker GA. Evaluation of pulmonary function in muscular dystrophy patients requiring spinal surgery. Critical care medicine. 1982;10(10):645-9. 68. Miller RG, Chalmers AC, Dao H, Filler-Katz A, Holman D, Bost F. The effect of spine fusion on respiratory function in Duchenne muscular dystrophy. Neurology. 1991;41(1):38-40. 69. Granata C, Cervellati S, Ballestrazzi A, Corbascio M, Merlini L. Spine surgery in spinal muscular atrophy: long-term results. Neuromuscular disorders : NMD. 1993;3(3):207-15. 70. Jalanko T, Helenius I, Pakarinen M, Puisto V, Salminen P, Peltonen J, et al. Effects of surgical correction of neuromuscular scoliosis on gastric myoelectrical activity, emptying, and upper gastrointestinal symptoms. Journal of pediatric gastroenterology and nutrition. 2014;58(1):38-45. 71. Mohamad F, Parent S, Pawelek J, Marks M, Bastrom T, Faro F, et al. Perioperative complications after surgical correction in neuromuscular scoliosis. Journal of pediatric orthopedics. 2007;27(4):392-7. 72. Duckworth AD, Mitchell MJ, Tsirikos AI. Incidence and risk factors for post- operative complications after scoliosis surgery in patients with Duchenne muscular dystrophy : a comparison with other neuromuscular conditions. The bone & joint journal. 2014;96-B(7):943-9. 73. Master DL, Son-Hing JP, Poe-Kochert C, Armstrong DG, Thompson GH. Risk factors for major complications after surgery for neuromuscular scoliosis. Spine. 2011;36(7):564-71. 26 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis 74. Lipton GE, Miller F, Dabney KW, Altiok H, Bachrach SJ. Factors predicting postoperative complications following spinal fusions in children with cerebral palsy. Journal of spinal disorders. 1999;12(3):197-205. 75. Mackenzie WG, Matsumoto H, Williams BA, Corona J, Lee C, Cody SR, et al. Surgical site infection following spinal instrumentation for scoliosis: a multicenter analysis of rates, risk factors, and pathogens. The Journal of bone and joint surgery American volume. 2013;95(9):800-6, S1-2. 76. Thacker M, Hui JH, Wong HK, Chatterjee A, Lee EH. Spinal fusion and instrumentation for paediatric neuromuscular scoliosis: retrospective review. Journal of orthopaedic surgery. 2002;10(2):144-51. 77. Ramo BA, Roberts DW, Tuason D, McClung A, Paraison LE, Moore HGt, et al. Surgical site infections after posterior spinal fusion for neuromuscular scoliosis: a thirty-year experience at a single institution. The Journal of bone and joint surgery American volume. 2014;96(24):2038-48. 78. Roberts SB, Tsirikos, A.I. Peri-operative management of major spinal surgery. Orthopaedics and Trauma. 2013;27(4):220-8. 79. Kanga I, Wong JJ, Stern PJ. Detection of syringomyelia in a pediatric patient with mild scoliosis: a case report. The Journal of the Canadian Chiropractic Association. 2014;58(1):16-23. 80. Akbarnia BA, Yazici M, Thompson GH. The growing spine : management of spinal disorders in young children. Heidelberg ; New York: Springer; 2011. xxv, 629 p. p. 81. Horacek O, Mazanec R, Morris CE, Kobesova A. Spinal deformities in hereditary motor and sensory neuropathy: a retrospective qualitative, quantitative, genotypical, and familial analysis of 175 patients. Spine. 2007;32(22):2502-8. 27 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis 82. Bar-On E, Floman Y, Sagiv S, Katz K, Pollak RD, Maayan C. Orthopaedic manifestations of familial dysautonomia. A review of one hundred and thirty-six patients. The Journal of bone and joint surgery American volume. 2000;82A(11):1563-70. 83. Guille JT, Sarwark JF, Sherk HH, Kumar SJ. Congenital and developmental deformities of the spine in children with myelomeningocele. J Am Acad Orthop Surg. 2006;14(5):294-302. 28 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis Table 1. Scoliosis Research Society classification and incidence of spinal deformity in neuromuscular conditions. Classification Diagnosis Co-incidence of Scoliosis Central neurological Cerebral palsy 25-74% Central motor neuron Friedreich’s ataxia 80% involvement Syringomyelia 25-85% [79] cause Other (encephalopathy, Rett’s syndrome) Peripheral neurological Acute anterior poliomyelitis 17-65% [80] Peripheral motor Spinal muscular atrophy 67% neuron involvement Hereditary motor and sensory 26% [81] causes neuropathy Hereditary sensory and vegetative 86% [82] neuropathy (familial dysautonomia) Mixed central and Traumatic paralysis (before 10 100% peripheral neurological years of age) causes Myelodysplasia 60% Myelomeningocele 52-89% [83] Neuromuscular junction Myasthenia Unknown Muscular causes Duchenne Muscular Dystrophy 90% Arthrogryposis 30-67% [80] Other muscular dystrophies 29 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis Table 2. Preoperative clinical and radiological investigations for patients undergoing surgical correction of neuromuscular scoliosis Role of Investigation for Neuromuscular Scoliosis Investigation Assessment of Spinal Pathology Whole spine radiographs (PA, lateral & supine maximum traction) Whole spine MRI (if any suspicion of intraspinal pathology) Hips & pelvic radiographs Anaesthetic & FBCs, U&Es, LFTs Medical Assessment Blood cross-match Albumin/calcium/vitamin D Coagulation screen Chest radiograph ECG, echocardiogram PFTs, ABGs, sleep studies, spirometry Nutritional assessment Urinalysis, urine culture & sensitivities Neurological assessment Keys: FBC (full blood count), MRI (magnetic resonance imaging), U&Es (urea & electrolytes), PFTs (pulmonary function tests), ABG (arterial blood gases), ECG (electrocardiogram), LFTs (liver function tests), PA (posteroanterior). 30 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis Figure Captions Figure 1. Spinal deformity patterns in cerebral palsy associated neuromuscular scoliosis. In types A and B (double curves of the thoracic and lumbar spine), the spine remains well balanced with little or no pelvic obliquity. In types C and D (large thoracolumbar or lumbar curves), the deformity extends into the sacrum and often causes significant pelvic obliquity. Figure 2. Radiographs of a patient with Friedrich’s ataxia showing pre-operative a) posteroanterior (PA) and b) lateral radiographs of the spine at age 14 years and 6 months. A primary thoracolumbar scoliosis measuring 50o with a compensatory thoracic curve measuring 35o and no pelvic deformity can be seen. Post-operative c) PA and d) lateral radiographs at age 17 years and 2 months following posterior spinal fusion demonstrate excellent correction of the thoracolumbar and thoracic curves to 8o and 5o, respectively, with restoration of global spinal balance. Figure 3. Radiographs of a patient with quadriplegic cerebral palsy showing preoperative a) posteroanterior (PA) and b) lateral radiographs of the spine at age 14 years and 8 months. A collapsing thoracolumbar scoliosis measuring 88o with associated thoracic hyperkyphosis measuring 98o and severe pelvic obliquity can be seen. The pain had severe back and left costo-pelvic impingement pain (bony pain produced due to the lower ribs sitting against the elevated left side of the pelvis) which did not allow him to sit on his wheelchair. Post-operative c) PA and d) lateral radiographs at age 17 years and 1 month following posterior spinal fusion demonstrate correction of the thoracolumbar curve to 25o, levelling of the pelvis and normalisation of thoracic kyphosis to 40o. An intrathecal Baclofen pump may also be seen in the radiographs and this was preserved in place during scoliosis surgery. 31 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis Figure 4. Additional education resources for patients and healthcare professionals. 32 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis Figure 1 33 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis Figure 2a 34 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis Figure 2b 35 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis Figure 2c 36 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis Figure 2d 37 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis Figure 3a 38 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis Figure 3b 39 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis Figure 3c 40 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis Figure 3d 41 Factors Influencing the Evaluation and Management of Neuromuscular Scoliosis Figure 4 Scoliosis Association (UK): charity supporting patients with scoliosis; www.sauk.org.uk Scottish National Spine Deformity Service: information regarding the service, spinal deformities, and their treatment; http://www.nhslothian.scot.nhs.uk/Services/AZ/ScottishNationalSpineDeformityService/Pages/default.aspx British Scoliosis Society: society supporting surgeons, healthcare workers and researchers regarding scoliosis; http://www.britscoliosissoc.org.uk British Scoliosis Research Foundation: charity promoting research into scoliosis and allied health conditions in the UK; http://www.bsrf.co.uk Scoliosis Research Society: society supporting education for healthcare workers and research in spinal deformities; http://www.srs.org 42