Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
History of invasive and interventional cardiology wikipedia , lookup
Cardiac surgery wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
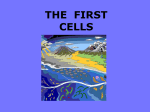
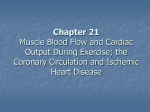
Total and Regional Coronary Blood Flow Measured by Radioactive Microspheres in Conscious and Anesthetized Dogs By Raul J. Domenech, M.D., Julien I. E. Hoffman, M.D., Mark I. M. Noble, M.B., Ph.D., Kenneth B. Sounders, M.D., James R. Henson, B.A., and Sujanto Subijanto, M.D. Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 ABSTRACT Total and regional coronary blood flow were measured in dogs by left atrial injection of carbonized microspheres labeled with different radioactive isotopes (mean diameter 14 to 6lfi). Simultaneously blood was collected at 20 ml/min from a catheter tied into a peripheral artery. The ratios of flow to radioactivity in myocardium and arterial blood should be equal if microspheres are well mixed in the aortic root and are distributed regionally in proportion to flow. This was proved in seven right heart by-pass experiments where coronary venous drainage was measured directly. Also, less than 0.1% of total myocardial radioactivity appeared in coronary venous blood, even with hypoxemia and small microspheres. Total coronary flow in seven conscious dogs averaged 95 to 150 ml/min/100 g heart; and flow to the left ventricle was 111 to 169 ml/100 g. Although not validated independently, there was evidence that values for flow to each ventricle, the atria and the septum were correct. The radioactivity per gram of left ventricular subendocardial muscle was 2.5 times that of subepicardial muscle using microspheres 51 to 61yx in diameter, but the ratios were 1.4 and 1.3 using microspheres of mean diameters 20 to 23/i, and 14/i, respectively. It is unlikely that any of these microspheres measure blood flow to small portions of the ventricle. ADDITIONAL KEY WORDS left ventricular muscle flow coronary venous drainage right heart by-pass arteriovenous shunts right ventricular muscle flow arterioluminal shunts particle streaming • Coronary blood flow to the whole heart or to specific portions of it is difficult to measure From the Cardiovascular Research Institute and the Department of Pediatrics, University of California San Francisco Medical Center, San Francisco, California 94122. This work was supported in part by U. S. Public Health Service Program Project Grant HE-06285 from the National Heart Institute. Dr. Domenech was a U. S. Public Health Service International Postdoctoral Research Fellow (F05 TW 1181). Dr. Hoffman was formerly an Established Investigator of the American Heart Association. Dr. Noble was a senior Fellow and Dr. Saunders a Junior Fellow of the San Francisco Bay Area Heart Research Committee. Mr. Henson was supported by U. S. Public Health Service Ceneral Research Support Crant (University of Cincinnati College of Medicine). Dr. Subijanto was supported by the Agency for International Development. Received June 30, 1969. Accepted for publication September 15, 1969. Circulation Research, Vol. XXV, November 1969 in conscious dogs. Only electromagnetic or ultrasonic flowmeters or indicator dilution techniques might be applicable for total flow; however, flowmeter transducers can seldom be implanted successfully on both right and left main coronary arteries, and indicator dilution curves are difficult to perform and evaluate because of the small size of the right coronary artery and early branching of the left coronary artery. None of these techniques can measure flow to a ventricle or any specific portion of it. All other methods—nitrous oxide washout (1, 2), washout of indicators injected into the myocardium (3, 4) or coronary arteries (5, 6), rubidium clearance techniques (7, 8) — either measure flow per unit weight of myocardium without referring it to a welldefined region of the heart, refer it only to the 581 582 DOMENECH, HOFFMAN, NOBLE, SAUNDERS, HENSON, SUBIJANTO Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 left ventricle or else require sacrifice of the animal within a few minutes of the injection of the indicator. These methods are often difficult to apply in either conscious or unconscious intact dogs. Rudolph and Heymann (9) developed a method for measuring the distribution of the total cardiac output to different organs by the injection of carbonized microspheres labeled with gamma-emitter nuclides. The principle of the method is that if the microspheres are well mixed at the root of the aorta, are distributed in proportion to blood flow, and do not escape from the organs, their fractional distribution in the organs will be in proportion to the fraction of cardiac output going to the organs. Then, if the flow to any organ (reference flow) is known, the flow to any other organ can be determined. This principle has been validated for many organs (9, 10), but because the coronary arteries arise close to the site of injection of microspheres in the left atrium or ventricle, we could not assume that the microspheres would be mixed well enough in the root of the aorta to permit the correct measurement of coronary blood flow. Therefore we checked the accuracy of this method in right heart by-pass preparations in which almost all the coronary venous drainage could be measured, and then applied it to measure total coronary flow in conscious dogs. In these studies we also estimated the distribution of flow to atria, ventricular septum, and ventricular free walls as well as to portions of the ventricular walls, for example, subendocardial and subepicardial regions. These measurements could not be checked directly, so we obtained indirect evidence in support of our conclusions by using microspheres of different sizes and altering the mechanical and metabolic functions of the heart by preparations with nonworking left ventricles. Methods The microspheres1 were labeled with six iFrom Nuclear Products Division of Minnesota Mining & Manufacturing Company. These spheres have a specific gravity of 1.3 to 1.6; they contain Ql% different radioactive nuclides; the mean diameters and standard deviations in microns of the large microspheres were: 125 I, 56.0 ± 3.8; 141Ce, 60.0 ± 6.8; 51Cr, 60.9 ± 6.4; 85Sr, 55.8 ± 6.3; 91 Nb, 50.9 ± 3.6; «Sc, 55.0 ± 4.8. The smaller microspheres used in some experiments had diameters: 125 I, 22.4 ± 3.08 or 83Sr, 14.1 ± 2.52 and 20.5 ± 2.53. The total number of microspheres given with each injection usually varied from 7,000 to 160,000, depending on the activity of each radioisotope, but twice about 800,000 microspheres with low activity were injected; with each injection about 1 to 2 yu,c of isotope was given. Microspheres were suspended in a solution of 20% dextran of medium molecular weight (with a small amount of polyoxyethylene-80-sorbitan mono-oleate [Tween 80] to prevent aggregation [9]), placed in a small stirring chamber of about 3-ml capacity and stirred with a Teflon-covered magnet until no clumps were seen. Then they were flushed into the left atrium through a thin polyvinyl catheter with about 15 to 20 ml saline in 12 to 50 sceonds. The reference flow was collected from a catheter tied into an artery, usually the brachial but occasionally the femoral or internal mammary. To avoid trapping microspheres between the arterial wall and the catheter, the ligature was tied as close to the tip of the catheter as possible. The reference flow was adjusted to about 20 ml/min and its actual volume obtained by weighing a timed sample and measuring its density. The reference flow was started a few seconds before the injection of microspheres and was collected for 15 to 30 seconds after finishing the injection; it was collected in fractions for 1 to 5 minutes after the end of the injection in ten injections in five dogs to determine the time taken for all the microspheres to emerge. Each dog was killed by intravenous injection of sodium pentobarbital, the heart was excised, cleaned of blood on its surface and the cavities flushed with water and swabbed with gauze. The visible epicardial fat and large vessels were removed and counted together with the valves and chordae tendineae. The atria were split into the left and right atrial free walls and septum. Both ventricular free walls were cut as close as possible to the ventricular septum. This was relatively easy for the right ventricle; however, although the posterior limit of the free wall for the left ventricle was defined by the right border of the posterior papillary muscle, the anterior limit had to be chosen arbitrarily. The left ventricular free wall was divided into anterior and carbon and 33% oxygen, but their exact composition has not been disclosed. Circulation Research, Vol. XXV, November 1969 TOTAL AND REGIONAL CORONARY BLOOD FLOW Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 posterior papillary muscles (pooled) and four layers across the wall, each extending from apex to base; the inner (or subendocardial) layer made up of the trabeculated muscle, and the outer (or subepicardial) layer were each 1 to 2 mm thick, and thinner than the other two layers, which consisted of the intermediate muscle split in halves. The right ventricular free wall was divided into the major papillary muscles (pooled), the inner layer of trabeculated muscle, a thin subepicardial layer, and a thicker intermediate layer. The septum was divided into three layers of equal thickness—left, middle, and right layers. The heart and blood samples were placed in glass vials (9) and counted in a well scintillation detector connected to a 400-channel pulse-height analyzer.2 The total activity for each radioisotope was obtained by modifying the method of Rudolph and Heymann (9) for use with six radioisotopes. Because of the overlap of spectral energies for 40Sc and 91Nb, the former was not often used. All blood samples were centrifuged and the supernatant fluid was counted to determine the amount of radioactivity not bound to microspheres. Right Heart By-pass.—Nine mongrel dogs weighing 22 to 33 kg were anesthetized with sodium pentobarbital, 35 mg/kg iv, with subsequent smaller doses as needed. The blood from both venae cavae was drained into the reservoir of a system previously filled with dog blood or 6% dextran solution in saline and returned by a roller pump into the pulmonary artery. A no. 14 Bardic catheter with side holes was introduced into the right ventricular cavity through the azygos vein to drain the coronary venous return from the right chambers of the heart into the reservoir. Both the output of the pump and the coronary venous return were measured continuously by cannulating electromagnetic flowmeter transducers (Statham M-4001) to verify constancy of flow during the studies. By changing the output of the pump, different coronary blood flows were obtained. In two dogs, the aorta was constricted by a clamp, and two other dogs were made hypoxemic (oxygen tensions of 14 and 26 mm Hg) and hypercapnic (carbon dioxide tensions 84 and 62 mm Hg) by breathing in a closed circuit; both maneuvers produced high coronary flows. A catheter was tied into a brachial artery in seven dogs, in a femoral artery in one dog, and in both arteries in another. While the reference flow from these arteries was being collected, the coronary venous return was drained directly into a graduated cylinder, then measured. In some experiments, including those in which coronary 2 Technical Measurements Corporation, 404C Multiple Pulse Height Analyzer, North Haven, Conn. Circulation Research, Vol. XXV, November 1969 583 venous return was increased two- to threefold by hypoxemia, the total coronary venous return was counted to detect any radioisotope which might pass through the myocardial vascular bed. In eight of the nine dogs, between two and five sets of microspheres, each with a different isotope, were injected successively; the remaining dog had two injections, each with two different sets of microspheres mixed in the stirring chamber. In some dogs, both large and small microspheres were injected. Conscious Dogs.—In seven other dogs a thin polyvinyl catheter was implanted into the left atrium; in two of them we placed an electromagnetic flowmeter transducer around the root of the aorta and a Microsystems 1017 pressure gauge through the left ventricular wall with its surface flush with the endocardium. One to ten days after surgery, a polyvinyl catheter was inserted under local anesthesia into the brachial artery. In one dog the catheter for the reference flow was placed in the internal mammary artery at the time of surgery. With the dogs lying quietly on their right sides, between two and six sets of microspheres, each labeled with a different radioisotope, were injected into the left atrium, and the reference flow was collected. Each experiment lasted about 1 to 2 hours and the interval between each injection varied from 15 to 30 minutes. After the last injection, the dogs were killed by large intravenous doses of pentobarbital and the hearts removed and divided. To get more information about the distribution of microspheres within the heart, similar studies were made on four additional conscious dogs, except that the reference flow was not measured. In three of them, smaller microspheres of mean diameter 14.1/x or 22 Afj, were alternated with the larger microspheres. Dogs with Nonfunctioning Left Ventricles.— To study the regional distribution of microspheres, several different preparations were devised in which the left ventricle did not work. In one dog, large catheters were placed in the left atrium and ventricle to drain blood into the reservoir, from which it could be pumped into both femoral arteries. Prior to by-pass, two control injections of microspheres were given; then the pump was started, adjusted to return aortic pressure to control levels, and one set of microspheres was injected into the output of the pump. In eight dogs not used in other studies, a cannula connected to a reservoir was placed in the root of the aorta. After a control injection of microspheres through this aortic cannula, the heart was stopped by inducing ventricular fibrillation with electrical shock in two dogs; injection into the left atrium or aorta of 30% KC1 DOMENECH, HOFFMAN, NOBLE, SAUNDERS, HENSON, SUBIJANTO 584 STROKE VOLUME LEFT VENTRICULAR PRESSURE (mm Mg) LEFT VENTRICULAR DIASTOLIC 20 PRESSURE (mmHg) Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 FIGURE 1 Left ventricular pressures and ascending aortic flow recordings in a conscious dog immediately after six successive injections of large microspheres into the left atrium. The flowmeter was not calibrated. The lowest tracing was recorded at high gain to show left ventricular diastolic pressure more clearly. The intervals between injections varied from 3 to 5 minutes. in two dogs; or continuous infusion of 0.1% acetylcholine into the left atrium or aorta in four dogs. At the same time, in five of these dogs the descending aorta and the arteries arising from the arch were occluded, and microspheres were injected into the root of the aorta while the coronary vascular bed was perfused at approximately the preexisting aortic pressure from the reservoir; in the other three dogs, perfusion took place with aortic pressures of 10 to 20 mm Hg. In the two dogs injected with potassium chloride and one with acetylcholine, the venae cavae and azygos vein were occluded, and the right chambers of the heart drained to estimate coronary blood flow during the injection of microspheres into the arrested heart. In two of these dogs, the inner and outer layers of the left ventricular free wall were digested with 70% nitric acid. The microspheres so obtained were measured with a calibrated eyepiece to study the relative distribution of different sizes in these regions. atrium in one conscious dog with a flowmeter transducer around the aortic root and a Microsystems model 1017 strain gauge in the left ventricular wall flush with the endocardium. A similar result was obtained in another dog. In these dogs there were no consistent changes of pressures or flows after successive injections of microspheres. In the remaining conscious dogs in which only arterial pressure and heart rate were recorded, no changes in heart rate or arterial pressure were observed during the injection of the microspheres. None of the dogs showed any sign of discomfort. After injection, no radioactivity was detected on the Teflon-coated stirring bar or in the effluent obtained by subsequently flushing out the stirring chamber. Furthermore, in seven injections in five dogs, successive separate fractions of the reference flow revealed no significant numbers of large microspheres circulating more than 30 seconds beyond the end of the injection; over 99% of the total microspheres were recovered in the reference flow within 1 minute of the begin- 320 280 240 200 I 60 120 80 40 4-0 80 120 160 200 240 280 320 CORONARY VENOUS RETURN (ml/min) 360 FIGURE 2 Results Figure 1 records the left ventricular stroke volume, left ventricular pressure, and first derivative of ventricular pressure with respect to time (dP/dt) after each injection of six successive sets of microspheres into the left Linear correlation between the directly measured coronary venous return to the right chambers of the heart and the values for total coronary blood flow calculated from the large microspheres in the right heart by-pass preparations. Solid circles = brachial artery; Open circles = femoral artery; Dashed lines represent 95% confidence limits for points. Circulation Research, Vol. XXV. November 1969 585 TOTAL AND REGIONAL CORONARY BLOOD FLOW ning of the injection. However, in three injections of small microspheres in three dogs, only S5% to 92% of the total amount of microspheres collected in the reference sample appeared within 1 minute after the beginning of the injection; the remainder appeared slowly over the next 4 minutes. TOTAL FLOW Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 Right Heart By-pass.—Figure 2 shows the correlation between the directly measured coronary venous return to the right chambers of the heart and the values for total coronary blood flow calculated from the large microspheres in the right heart by-pass preparation. In 27 measurements in seven dogs, the calculated flow was within 5% of the measured flow in 12, within 10% in 19 and within 20% in 24 measurements. Two of the 3 with the largest errors (24%, 20%, and 33%) were in one dog with abnormally low coronary blood flow. When small microspheres were used, coronary blood flow was overestimated by 6% to 70% (average 29%) in all studies in which the reference flow was collected for no more than 30 seconds from the end of the injection. Too few measurements were made with small microspheres and longer collection of reference flow to assess their accuracy in measuring total coronary flow. The total number of microspheres in the heart varied from 230 to 8,000 for large and from 9,000 to 25,000 for small microspheres. In the three dogs in which a total of ten injections of large microspheres were made and the coronary venous return was examined to detect any microspheres going through the coronary vascular bed, the radioactivity in the coronary venous return (after discounting the small amount in the supernatant fluid obtained by centrifuging the sample) was always under 0.5%, and usually less than 0.1% of the total radioactivity in the heart for every radioisotope. The coronary venous return measured in these dogs varied from 130 to 340 ml/min, the highest flow occurring in dogs with hypoxemia. Similar results were obtained in three dogs which had four injections of small microspheres (the smallest, 14.1 ± 2.52/x in diameter); the coronary venous return in Circulation Research. Vol. XXV. November 1969 these ranged from 120 to 180 ml/min. Conscious Dogs.—Table 1 shows the values for total coronary blood flow in the seven conscious dogs; coronary flow is also expressed per kilogram total body weight as well as per 100 g wet heart weight. The arterial pressures for these dogs varied from 160 to 180 mm Hg systolic and 70 to 90 mm Hg diastolic. The heart rates were 114 to 156 beats per minute; blood oxygen tensions 88 to 99 mm Hg and carbon dioxide tensions 22 to 35 mm Hg; blood pH varied from 7.30 to 7.42. In any one dog, none of these variables seemed to be related to the amount of coronary blood flow. The numbers of microspheres in the heart varied from 360 to 8,800 (large) and 6,400 to 65,100 (small). DISTRIBUTION TO LARGE REGIONS Figure 3 shows the percent distribution of the microspheres in the atria, right ventricular free wall, septum, left ventricular free wall, and septum plus left ventricular free wall in the 11 conscious dogs. The results obtained with small microspheres are included with those for the large microspheres in the three dogs in which large and small microspheres were injected, since no differences in the distribution of microspheres of different sizes were noted (Table 2). The proportions of total coronary flow going to left ventricular free wall plus septum, the right ventricular free wall or the atrium were almost constant, but the relative amounts to the septum and left ventricular free wall varied from dog to dog. From the values of total coronary blood flow obtained in seven dogs and the corresponding percent distribution, the coronary blood flow per gram of tissue for these regions of the heart was calculated (Table 3). An analysis of variance showed a significant difference between left and right ventricular free wall (P < 0.05) and between atria and right ventricular free wall (P<0.05), except in two dogs (P<0.10, 0.20). No significant difference was found between left ventricular free wall and septum except in one dog (P<0.025); however, taking 21 pairs of differences in the six dogs with two or more DOMENECH, HOFFMAN, NOBLE, SAUNDERS, HENSON, SUBIJANTO 586 TABLE 1 Total Coronary Blood Flow (CBF) in Conscious Dogs Body No. wt observations Dog (kg) 1 2 3 4 5 6 7 27.5 23.8 1 2 4 5 20 18 20 28 4 2 4 22.7 CBF/kg body wt (mlmin-'kg-') Mean Range Total CBF (ml-min"1) Mean Eange 239 177 159 136 132 234 153 8.69 7.44 7.96 7.54 6.61 8.37 6.75 175-179 137-201 123-155 99-154 220-249 144-164 7.35- 7.53 6.85-10.05 6.83- 8.61 4.95- 7.70 7.86- 8.89 6.34- 7.22 CBF/100 g heart wt (mlmln-'lOO g"1) Range Mean 150 95 132 114 108 99 114 94- 96 114-167 103-131 81-126 93-106 107-122 The same number is used for the same dog in all the tables. Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 radioisotopes injected, the flow to the left ventricular free wall averaged 0.15 ml/g higher than that to the septum. The magnitude of this difference in each dog was unrelated to the relative distribution of flow to the septum and left ventricular free wall. In comparing the distribution of micro- spheres to these large regions in the conscious dogs and those on right heart by-pass, there were significant differences (unpaired f-test) in the percent distribution to the right ventricular free wall and the left ventricular free wall plus septum. For the right ventricular free wall, the mean percent of total & 80 1 70 § o 60 Q: 5 0 § 40 30 ° 20 i k 10 ATRIA RIGHT VENTRICULAR LEFT LEFT VENTRICULAR SEPTUM VENTRICULAR VENTRICULAR FREE WALL FREE WALL FREE WALL + SEPTUM FIGURE 3 Distribution of coronary blood flow to different regions of the heart in conscious dogs. In each group one bar represents one dog, and the sequence of bars is the same for the different groups. Vertical lines at the tops of the bars represent the ranges of measurements in the dogs with over two measurements. Solid circles indicate that large and small microspheres were used. Circulation Research. Vol. XXV, November 1969 587 TOTAL AND REGIONAL CORONARY BLOOD FLOW TABLE 2 Percent Distribution of Large and Small Microspheres to Ventricles :RV free wall Type of study Dog Conscious dog If 2t 3 Anesthetized, closed chest st 9 Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 Open chest 10J Right heart by-pass lit 12t 51-61/1* 51-61,1* 14-23,1* 14.1 19.2 1S.9 17.6 16.7 17.S 17.4 17.S 73.2 70.9 70.9 70.9 66.2 6S.9 70.6 68.9 19.5 16.6 15.7 19.6 1S.1 14.6 17.6 16.2 15.9 19.1 17.8 13.4 10.7 74.S 77.6 76.9 76.9 76.6 77.7 85.3 84.9 S3.6 76.6 77.8 71.3 73.7 75.4 78.9 83.6 84.3 S5.3 9.0 9.0 11.3 13 LV including septum 14-23,.* 9.3 10.0 0.57 0.5 > P > 0.4 t P 1.76 0.2 > P > 0.1 RV = right ventricle; LV = left ventricle. *Microsphere diameter. tSimultaneous injection of small and large microspheres. In the others, small and large microspheres were injected with a short interval between them and with relatively stable heart rates and aortic blood pressures; the order of injection varied. tDuplicate studies in the same dog. coronary blood flow was 13.4 ± 3.2 SD (n = 22) in the right heart by-pass and 17.2 ±2.1 SD (n = 40) in the conscious dog (P < 0.001). For left ventricular free wall plus septum the mean percent was 79.4 ± 4.0 SD (n = 21) in the right heart by-pass and 75.3±3.2 SD (n = 40) in the conscious dog (P < 0.001). No significant difference was found for atrial flow distribution. In conscious dogs or anesthetized dogs (some with right heart by-pass), the proportional distribution of microspheres to the right ventricular free wall and the left ventricle plus septum was independent of microsphere size (Table 2). DISTRIBUTION TO SMALL REGIONS In the two dogs in which the inner and outer layers of the left ventricle were digested so that the microsphere diameters could be measured, the same distribution of diameters was found in both layers for large (mean diameter 51/n and 55/i.) and medium-sized (mean diameter 22AJX) microspheres. Circulation Research, Vol. XXV, November 1969 Table 4 shows the proportional distribution of radioactivity to different regions of the heart in a conscious dog after successive injections of large microspheres labeled with different isotopes. The proportions were similar for the different injections in this dog as well as in the other ten conscious dogs. In addition, the flow per gram was calculated for each region (Table 4), assuming that flow and radioactivity were proportional (see below). There was almost always a gradient in the distribution of radioactivity across the free walls of both ventricles, the inner layers having the greatest amount per gram and the outer layers the least. The only exceptions to the gradients shown in Table 4 occurred in three dogs in which the outer layer had a greater amount of radioactivity per gram than the layer next to it, but the inner layer still had more radioactivity per gram than the outer. In 38 measurements with large microspheres in 11 conscious dogs, the radioactivity per gram of the inner layer divided by DOMENECH, HOFFMAN, NOBLE, SAUNDERS, HENSON, SUBIJANTO 588 -H CJ -H -H — ~ O TO c i CO O - * — TO —< CO o TO + Ci —< co o — cc TO tO —' IC TO ?> -^ -* ^ N M C to O to C: -N5 W is c7 J! 3 co 5 3 _^ -* O i co OI ^ C> IN T)H ~ rf c: co TO TO ^1 TJ< 1^ i~ <N -^ C; b - O5 CO •# C-) —I iff £ s jj 3 5 jl t^ i^> c; oo o o ^) -—' CO O TtH C-l O T^ CO < I- c; o_) oco TO — co co i^ c; i^ o co o CO 576853- to 597570- Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 TO 1^ TO *3 •I s d 55 02 to co 3 E-1 the radioactivity per gram of the outer layer gave mean ratios for the right ventricular free wall of 1.8 ±0.5 SD (n = 14), and for the left ventricular free wall 2.7 ± 0.8 SD (n = 14). A gradient of radioactivity per gram was also noted across the interventricular septum, with a mean ratio (left:right) of 2.4 ± 0.7 SD (n = 14). When small (mean diameter 14.1/x) or medium-sized microspheres (mean diameter 20.5/LA or 22.4/A) were injected simultaneously with, or within a short time of, large, microspheres (mean diameter 50.9 to 60.9^i) there were significant differences in the ratios of radioactivity per gram of inner to outer ventricular layers or left- to right-sided ventricular septal layers (Table 5). These differences from the ratios with large microspheres were significantly larger (unpaired ttest) with the small microspheres than those of medium size for the free wall of the left ventricle (P<0.05) and the ventricular septum (P < 0.05) but not for the right ventricular free wall (P = 0.2). In the right heart by-pass studies with large microspheres, the ratio of radioactivity per gram (inner:outer) was 2.0 ± 0.8 SD (n=16) for the right ventricular free wall—not significantly different from that for the conscious dogs (0.5<P<0.6). However, the ratio of radioactivity per gram of inner to outer layers of 1.9 ± 0.7 SD for the left ventricular free wall was significantly less than for conscious dogs (P < 0.01). The ratio for the left to right sides of the septum was 1.9 ±0.6 SD (n=16) and was not significantly lower than that in conscious dogs (0.10 > P > 0.05). In each nonvvorking left ventricle with normal aortic pressures there was usually no change in the ratio of radioactivity per gram (inner to outer layers) of the ventricular free walls or of the left to right sides of the ventricular septum compared to control values (Table 6). In three of these dogs whose hearts were arrested and whose coronary venous return was measured, the flows were 140,200 and 300 ml/min. In three other dogs with very low perfusing pressures after acetylcholine arrest, the ratios were below 1. Circulation Research. Vol. XXV. November 1969 589 TOTAL AND REGIONAL CORONARY BLOOD FLOW TABLE 4 Percent of Total Cardiac Radioactivity and Blood Flow per Gram in Different Regions (Large Microspheres) Percent of total cardiac radioactivity wt Region Flow per gram (K) mi i«Ce »Sr '•Nb mi •'"Ce »Sr "Nb 6.05 2.53 6.39 1.4 0.7 2.7 2.5 0.9 3.9 2.4 0.7 5.0 1.9 0.7 4.0 0.4 0.3 0.7 0.6 0.6 1.0 0.6 0.4 1.2 0.5 0.4 0.9 Right ventricle Papillary muscle Subendocardial layer Middle layer Subepicardial layer 0.S2 5.74 17.57 4.29 0.3 5.S 8.2 3.4 1.2 6.1 8.3 2.3 0.8 5.2 8.5 3.3 0.5 3.7 7.5 3.4 0.6 1.7 O.S 1.3 2.3 1.7 0.7 O.S 1.4 1.3 0.7 1.1 0.9 0.9 0.6 1.1 Ventricular septum Right side Middle Left side 5.55 23.86 4.24 5.2 4.S 2.S 17.5 16.3 15.4 9.5 S.I 8.3 3.1 1S.4 S.2 1.5 1.2 3.7 1.4 1.1 3.0 0.7 1.0 2.9 O.S 1.1 2.S Left ventricle Papillary muscle Subendocardial layer Inner middle layer Outer middle layer Subepicardial layer 3.22 4.95 16.88 15.39 6.S7 6.2 9.0 7.0 S.2 6.2 S.9 16.2 17.8 18.5 5.4 9.6 19.7 9.2 3.6 S.4 3.6 9.2 3.9 9.5 3.6 3.2 3.0 1.6 1.0 0.9 3.4 2.6 1.7 0.9 0.8 2.S 2.7 1.6 0.9 0.8 2.4 2.8 1.7 0.9 0.8 Fat, valves, large vessels 10.19 1.0 0.7 1.0 0.8 0.2 0.1 0.1 0.1 Atrium Right Septum Left Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 Conscious dog (no. 7) with successive injections of large microspheres. Calculated total coronary blood flow in ml/min was, respectively, 164, 157, 148 and 144. Discussion This technique permits complete injection of microspheres and their collection in the reference sample without causing any discomfort to the dog or detectable changes in cardiac function. Furthermore, after successive injections of microspheres there were no large or consistent changes of aortic pressure or coronary blood flow; therefore, in the numbers given, the microspheres did not alter coronary vascular resistance. However, to measure coronary blood flow by this technique no significant numbers of microspheres can pass through the myocardial vascular bed, and they must be well mixed at the root of the aorta. The microspheres used in these experiments ranged in mean diameter from 14.1/x to 60.9/z and are far larger than the diameter of the capillaries of the dog heart (3/x to 8/LI) (11). Therefore, only those going through large Circulation Research, Vol. XXV, November 1969 arteriovenous and arterioluminal shunts could pass through the coronary circulation. After discounting the amount of free radioactivity in the solution for each set of microspheres, less than 0.5% (usually under 0.1%) of the total radioactivity in the heart was found in the coronary venous blood, even during marked coronary vasodilation from hypoxemia and with the smallest microspheres. Since the microsphere diameters have a gaussian distribution, at least 2% of those with a mean diameter of 14.Lu were below 9/i. in diameter; therefore there were clearly no significant arterioluminal and arteriovenous shunts above this diameter into the right chambers of the dog heart. Prinzmetal et al. (12), who injected glass spheres into the coronary arteries of the postmortem human heart, described shunts of about 70^. to 220/i, in diameter between the coronary arteries and both ventricular cavities DOMENECH, HOFFMAN, NOBLE, SAUNDERS, HENSON, SUBIJANTO 590 TABLE S Ratios of Radioactivity per Gram of Inner lo Outer Layers of Ventricular Free Walk and Left to Right Side of Ventricular Septum Inner : outer layer LV free wall Left:right side ventricular septum RV free wall Large Medium Large Medium Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 Dog Large Medium 1* 2 3 8* 9 10 11 12 13* 2.54 1.32 1.98 3.13 3.85 2.00 1.36 2.26 1.82 1.94 1.19 1.34 2.91 1.69 1.30 0.27 2.26 1.27 2.60 1.20 1.49 2.39 2.75 1.51 1.37 3.08 2.08 2.32 1.03 1.14 1.73 1.54 0.86 0.90 1.87 1.42 2.57 2.32 1.97 1.79 2.27 2.34 1.59 1.63 1.92 1.68 2.03 1.62 1.97 1.62 1.44 0.81 1.27 1.16 2.25 0.82 1.43 0.91 2.05 0.69 1.42 0.49 2.04 0.35 1.51 0.39 Large Small Large Small Large Small 2.59 4.18 1.78 3.06 0.96 1.75 1.02 1.41 1.72 2.39 1.32 3.19 1.00 1.07 0.76 2.05 3.43 2.26 2.22 2.50 1.19 1.35 1.41 1.37 2.90 1.00 1.28 0.37 2.15 0.82 1.22 0.57 2.60 0.57 1.33 0.10 MEAN SD <0.02 P 2 8* 10 12 M HAN SO P < 0.005 <0.02 < 0.02 <0.01 < 0.05 Large = microspheres ol-61/i in diameter; Medium = microspheres 20.5 or 22.4/x diameter; Small = microspheres 14.1M diameter. Dogs 1-3 were conscious; dogs 8-13 were anesthetized; dogs 8 and 9 had closed chests, dog 10 had an open chest, and dogs 11-13 had the right heart by-passed. LV and RV as in Table 2. *Simultaneous injection of large and smaller microspheres. and also arteriovenous shunts into the coronary sinus of 70/JL to 170/J. in diameter. However, even though the difference in species and experimental conditions makes comparison of their experiments with ours difficult, there is in fact no conflict. They injected 5 to 12 million spheres into the coronary arteries. If arterioluminal or arteriovenous shunts into the right chambers of the heart carry less than 0.1% of the coronary blood flow (the usual upper limit from our data), then this would have permitted 5,000 to 12,000 of their glass spheres to pass the capillary bed. These would easily have been detected, although they did not mention the total number of spheres recovered from the cardiac chambers. MacLean et al. (13), who injected radioactive glass microspheres 20/JL in diameter into the root of the aorta in the beating but nonworking dog heart, found no radioactivity in the left chambers of the heart; 4% of the radioactivity entering the coronary arteries drained into the right chambers of the heart. It is possible that the difference between their results and ours are due to their use of a nonworking heart. Recently, Fortuin et al. (14) found no significant passage of microspheres 15/tt in diameter and labeled with 40 Sc into the coronary sinus. There is less information about arterioluminal shunts into the left atrium and ventricle, and only MacLean et al. (13) studied this directly with microspheres. However, the direct coronary venous drainage into the left chambers of the dog heart is less than 5% of the total coronary flow in the isolated heart (15) and less than 2% in more physiological Circulation Research, Vol. XXV, November 1969 591 TOTAL AND REGIONAL CORONARY BLOOD FLOW TABLE 6 Ratios of Radioactivity per Gram of Inner lo Outer Layers of Left Ventricular Free Wall in Working and Nonworkr ing Ventricles Method Working heart Left heart by-pass 1.74, 2.61 Ventricular fibrillation 4.62 Ventricular fibrillation 2.65 Potassium chloride arrest 1.35 Potassium chloride arrest 2.57 1.20 Acetylcholine arrest Acetyleholine arrestf 2.55 Acetylcholine arrestf 1.59 Acetylcholine arrestf 2.S9 Non-working heart 1.92 3.28 2.74 1.26 2.59 2.17, 2.27* 0.36, 0.33* 0.91, 0.89* 1.05 Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 *Both sets of isotopes injected simultaneously. fAortic pressure not maintained during arrest. preparations (16). From all these studies it seems that no significant numbers of microspheres escape through the coronary vascular bed. The same studies permit us to state that the coronary venous drainage measured in the right heart by-pass experiments represented over 95% of the total coronary venous drainage. Therefore the high correlation between calculated and measured coronary flow (Fig. 2) can be interpreted as a proof of adequate mixing of the large microspheres at the root of the aorta and their subsequent distribution to the heart and reference sample in proportion to their flows after left atrial injections. There are two possible explanations for the overestimate of coronary blood flow in our earlier studies with small microspheres; namely, disproportionately few microspheres in the reference sample or disproportionately too many in the heart. Our results show that collecting the reference flow for 1 minute did not allow for the long transit time of small microspheres, so that they were underrepresented in the reference sample. We do not know the reason for this difference in transit time, but it may be due to a more peripheral position of small microspheres in the arterial lumen so that some travel in slower streams (17). It is probably not due to recirculation of small microspheres, since these on their second and subsequent circulations should be Circulation Research, Vol. XXV, November 1969 distributed in proportion to flow, thus retaining the proportionality of radioactivity to flow in the heart and reference blood. A disproportionately high distribution of microspheres to the heart could occur only if at the root of the aorta there were more small microspheres in the periphery than near the axis of the stream and the coronary flow came mainly from this region. Segre and Silberberg (17) have shown that with a steady flow in a tube, particles are evenly distributed across the radius of the inlet; in this respect the aortic root resembles their model. Furthermore, Bellhouse et al. (18) have shown in models that vortices produced in the aortic root could provide a homogeneous distribution of particles. Both of these studies suggest that the heart should not receive a disproportionately high number of microspheres. Flow to Large Regions.—The flow per 100 g total heart weight was less than that per 100 g left ventricular free wall plus septum in the TABLE 7 Coronary Blood Flow (ml • min~l) per 100 Grams of Left Ventricle by Different Authors No. Ref. measurements Method Mean Range SD 79-220 111-169 35 24 Conscious Dogs 19 * * 20 21 22 23 24 1 25 7 27 22 N2O microspheres 133 135 Anesthetized Dogs (Closed Chest) 138-226 microspheres 173 3 101 N,0 8 81 9 N2O 104 10 N,0 100-220 147 12 N2O 121 10 N2O 71 17 N2O 14 21 133 86 Xe Rb 89 112 44 33 14 24 39 23 11 29 Since most dogs in these studies had several estimations of coronary blood flow, standard deviation (SD) is not based on independent observations. However, analysis of variance showed no significant differences between the means for each of our dogs, so that the observations have been regarded as independent for comparison with those of other workers. •Combined left ventricular free wall and septum, present study. 592 DOMENECH, HOFFMAN, NOBLE, SAUNDERS, HENSON, SUBIJANTO Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 seven conscious dogs; (ratio 77% to 90%, mean 83%). This follows from the lower flows observed per 100 g of atrial or right ventricular muscle and must be kept in mind when interpreting coronary blood flows derived by methods which relate flow to the mass of left ventricular muscle. When we compared our values with those reported for coronary blood flow per 100 g left ventricular muscle (Table 7) with studies on conscious and anesthetized dogs by different methods (1, 7, 19-25), the agreement was reasonably good; the values during anesthesia were generally lower than in the conscious state. The fact that our method and the nitrous oxide method agree well is in keeping with observations that coronary sinus blood probably represents most of the venous drainage from the left ventricle (2). We have not validated regional flow to the atria, ventricular free walls, and septum but believe that these regional flow measurements may be correct. (1) The method can measure small flows like those going to right or left ventricles, as shown by the right heart bypass studies with low total coronary blood flows (Fig. 2). (2) The regional distribution of blood flow and its variation in different physiological states was consistent with determinants of coronary flow. In general, coronary blood flow varies with metabolic needs (24, 26-28) but may also depend on vascular impedance within the myocardium for regulation of local flow (29). Thus, the greater proportion of flow going to the left ventricle (including septum) is expected because of its greater muscle mass and expenditure of energy; the latter would also explain the greater flow per gram of left ventricular muscle. Furthermore, the fact that in the right heart by-pass studies the distribution of flow to the nonworking right ventricular free wall was less than in the conscious dog is also consistent with the importance of metabolic factors in regulating coronary blood flow. On the other hand, in one experiment there was no change in relative flows to right and left ventricles after left heart by-pass was started, perhaps because of proportional lowering of the effects of left ventricular metabolism and impedance. (3) Our results for flow per 100 g of left ventricle in conscious dogs agree with those obtained by others using the nitrous oxide method. (4) The percent distribution to large regions of the heart is similar with large and small microspheres and with a diffusible indicator (7). In the conscious dogs, the ratio of flow per gram of left ventricular free wall plus septum to right ventricular free wall varied from 1.24 to 1.59 (mean 1.43). These results differ from those of MacLean et al. (13), who found a greater flow per gram of tissue in the right ventricular free wall than in the left. Nevertheless, although they used a technique similar to ours, their experiments were done in a nonworking heart and are not comparable. On the other hand, our results agree with those of Love and Burch (30) and Levy and deOliveira (31), who measured distribution of coronary blood flow with the 8<iRb clearance technique in the anesthetized dog with an intact circulation; their ratios of flow per gram of left ventricular wall plus septum to right ventricular free wall averaged 1.48 and 1.49 respectively. Radioactivity of Small Region.?.—To inter- pret the ratio of radioactivity per gram of tissue in the inner to outer ventricular layers (or the two sides of the septum) as a ratio of flows, we must first know that the amount of radioactivity in a layer is proportional to the numbers of microspheres in it. This cannot be assumed, because the microspheres vary in volume. For example, microspheres with mean diameter 50/u. ± 5fi (standard deviation) have upper and lower 95% confidence limits for diameter of about 60/u, and 40/u. Microspheres with these diameters have volume ratios of 27:8 (3.4:1) and if the radioisotope is evenly mixed with the material composing the microsphere, then the average radioactivity of these larger microspheres in a batch will be 3.4 times that of the smaller microspheres. With microspheres 20/u, in diameter the volume ratios of the larger to the smaller microspheres in a batch is about 4.6:1. Because of the variability of microsphere Circulation Research, Vol. XXV, November 1969 TOTAL AND REGIONAL CORONARY BLOOD FLOW Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 volume in a batch, there might be a tendency for larger microspheres to be separated from the smaller microspheres by variations in arterial size, branching or position of differentsized microspheres in the stream. If this occurred, then the radioactivity in a region might not be proportional to number of microspheres or to flow. Our studies of the distribution of the diameters of large and medium-sized microspheres in inner and outer ventricular layers showed no significant differences, so this source of error was not present. However, when small or medium-sized microspheres were used, the ratios of radioactivity per gram in the inner to outer ventricular layers differed from those obtained with the large microspheres and from each other (Table 5). These differences can be explained by the known distribution of particles in flowing streams. Large microspheres similar to those used here have been shown to be concentrated near the axis of the stream (32) and so might be underrepresented in the proximal intramural coronary arteries which, if they resemble other vascular beds, are supplied by microspheres from the peripheral part of the stream. Smaller particles take longer to reach a similar distribution (17), so the smaller microspheres are probably more evenly dispersed across the lumen of the larger coronary arteries and thus more evenly distributed to subepicardial and subendocardial arteries. Even these small microspheres, however, are likely to show some tendency to axial concentration once they are beyond the orifices of the main coronary arteries and are thus likely to be slightly underrepresented in subepicardial vessels. (The equal distribution of microsphere diameters in inner and outer layers with any one batch of microspheres injected was probably due to the relatively narrow range of variations of diameters found within each batch. Thus the larger and smaller microspheres in a batch with a mean diameter of 50/u, had volume ratios of 3.4:1, but microspheres of 50fi and 20/u, in diameter have volume ratios of 15.6:1). After they have reached the terminal Circulation Research, Vol. XXV, November 196i> 593 vessels, movement of microspheres is unlikely because of the similarity of distribution before and after cardiac arrest. Furthermore, the similarity of distribution in the working and nonworking left ventricle favors an anatomically determined distribution of large microspheres more than a real variation in flow because of metabolic needs. It is possible, however, that the arrested or fibrillating left ventricle has a much lower than normal impedance to flow in the inner layers because of decrease of intramyocardial tension, rather like a prolonged diastole, so that even when the heart is not working, the flow in the inner layer of the ventricle would be greater than that in the outer layer. The only condition which permitted lower radioactivity per gram with the large microspheres in the inner as compared to the outer layers were very low aortic pressure and, probably, a very low coronary blood flow, as in three of the four studies with cardiac arrest after acetylcholine. Possibly preferential streaming of microspheres to the inner layer because of their momentum and inability to make sharp turns was abolished at low flows. Another possibility is that all the ratios are correct but that microspheres of different sizes measured different flows. Estes et al. (33) reported that in the postmortem human heart there was a subendocardial plexus of vessels which formed large looping arcades. If the flow in these vessels passes from deep to superficial layers and if the diameter of arteries in the deep layer is smaller than that of the large microspheres used here, then the large microspheres might measure total flow going as far as the inner layer, while the small microspheres would measure the actual or effective flow to each layer. However, the number, size, direction of flow in, and function of, these arteries is not known, nor have they been described in the dog. Numerous studies with diffusible indicators give a ratio of flow per gram in inner to outer layers of the left ventricle close to 1 (4, 3438). Even though the interpretation of results of methods using diffusible indicators has been criticized (3, 5), it is difficult to accept 594 DOMENECH, HOFFMAN, NOBLE, SAUNDERS, HENSON, SUBIJANTO Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 the ratio of 2.3 to 2.7:1 obtained with large, or 1.4 with medium-sized, microspheres as being correct. The ratio of 1.3:1 obtained with the smallest microspheres (Table 5) is closer to that found with diffusible indicators, but the weight of evidence is against microspheres of any size measuring flow to different layers of the ventricular wall. Critique of the Method.— This method has many advantages. The microspheres used for each injection cost only 7 to 30 cents. It is relatively easy to apply to the conscious dog, does not disturb the dog and apparently does not alter cardiac function or coronary circulation. It permits measurement of total coronary blood flow and its distribution to large regions of the heart. No theoretical assumptions have to be made about any blood-tissue interchange, for none occurs. It is not necessary to take heart samples immediately after the injection to avoid diffusion of the isotope from the tissue into the blood. With the microspheres available in our laboratory, five measurements of total coronary blood flow and its distribution can be made in each animal; other radioactive nuclide-labeled microspheres are available. Finally, a steady state is needed only for a relatively short time (about 1 minute with the large microspheres). There are, however, some disadvantages to the method. Counting the tissues involves much technical effort and the use of expensive equipment. The method measures mean and not phasic flow and requires a relatively steady state; if small microspheres are used this must last for about 5 minutes. The microspheres must not be clumped and have to be injected into the left side of the circulation, probably the left atrium, so that a catheter must be placed in the left atrium by prior operation, or by transseptal or retrograde left atrial catheterization. If the reference sample technique is used, a catheter must be tied into a peripheral artery. On the other hand, if the method of measuring cardiac output and determining the fraction of it going to the heart is used, then radioactivity must be measured on the whole animal after it is killed or special techniques used to count the total amount of radioactivity injected. There is a limit to the number of measurements that can be made, because of the demands on the instruments which separate the spectral energies of the different isotopes or because of the cumulative effect of the numbers of microspheres on the physiology of the animal. Finally, the animal has to be killed to make the counts. Acknowledgments We wish to thank Dr. Abraham M. Rudolph for use of counting equipment and advice; Drs. John M. Neutze and Felix Wyler, who first demonstrated the feasibility of the reference sample technique; Dr. Frederick Firestone for assistance with the right heart by-pass preparations; and Mr. Lesley Williams for technical assistance. References 1. ECKENHOFF, J. E., HAFKENSCHIELD, J. H., HABMEL, M. H., COODALE, W. T., LUBIN, M., BING, R. J., AND KETY, S. S.: Measurement of coronary blood flow by the nitrous oxide method. Am. J. Physiol. 152: 356, 1948. 2. BING, R. J.: Determination of coronary blood flow. Methods Med. Res. 8: 269, 1960. 3. SALISBURY, P. F., CROSS, C. E., OBLATH, R. W., AND RIEBEN, P. A.: Local circulation in heart muscle studied with Na 24 clearance method. J. Appl. Physiol. 17: 475, 1962. 4. KIBK, E. S., AND HONIG, C. R.: Nonuniform distribution of blood flow and gradients of oxygen tension within the heart. Am. J. Physiol. 207: 661, 1964. 5. BASSINGTHWAICHTE, J. B., STRANDEIX, T., AND DONALD, D. E.: Estimation of coronary blood flow by washout of diffusible indicators. Circulation Res. 23: 259, 1968. 6. HERD, J. A., HOLLENBERC, M., THORBURN, G. D., KOPALD, H. H., AND BARGER, A. C : Myocardi- al blood flow determined with krypton 85 in unanesthetized dogs. Am. J. Physiol. 203: 122, 1962. 7. LOVE, W. D., MUNFOHD, R. S., AND ABRAHAM, R. E.: Comparison of the effects of Z-norepinephrine, angiotensin, dipyridamole, digitoxin, and reserpine on the regional distribution of coronary blood flow. J. Lab. Clin. Med. 66: 423, 1965. 8. LOVE, W. D.: Isotope clearance and myocardial blood flow. Am. Heart J. 67: 579, 1964. 9. RUDOLPH, A. M., AND HEYMANN, M. A.: Circulation of the fetus in utero: Methods for studying distribution of blood flow, cardiac output and organ blood flow. Circulation Res. 21: 163, 1967. Circulation Research, Vol. XXV, November 1969 595 TOTAL AND REGIONAL CORONARY BLOOD FLOW 10. Use of radioactive microspheres to assess distribution of cardiac output in rabbits. Am. J. Physiol. 215: 486, 1968. 11. from rate of myocardial nitrous oxide desaturation. Circulation Res. 1: 502, 1953. NEUTZE, J. M., WYLJER, F., AND RUDOLPH, A. M.: 24. FOLTZ, E. L., PACE, R. G., SHELDON, W. F., WONG, S. K., TUDDENNAM, W. J., AND WEISS, A. J.: Factors in variation and regulation of coronary blood flow in intact anesthetized dogs. Am. J. Physiol. 162: 521, 1950. REYNOLDS, S. R. M., KIBSCH, M., AND BING, R. J.: Functional capillary beds in the beating, KCl-arrested and KCl-arrested-perfused myocardium of the dog. Circulation Res. 6: 600, 1958. 25. O'ROURKE, R. A., FISCHER, D. P., ESCOBAR, E. E., BISHOP, V. S., AND RAPAPORT, E.: Effect of acute pericardial tamponade on coronary blood flow. Am. J. Physiol. 212: 549, 1967. 12. PRINZMETAL, N., SIMKIN, B., BERGMAN, H. C , AND KRUGER, H. E.: Studies on the coronary circulation: II. Collateral circulation of the normal human heart by coronary perfusion with radioactive erythrocytes and glass spheres. Am. Heart J. 33: 420, 1947. 26. KATZ, L. N., AND FEINBERG, H.: Relation of cardiac effort to myocardial oxygen consumption and coronary flow. Circulation Res. 6: 656, 1958. Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 13. MACLEAN, L. D., HEDENSTROM, P. H., AND KIM, 27. BERGLUND, E., BORST, H. G., DUFF, F., AND S. Y.: Distribution of blood flow to the canine heart. Proc. Soc. Exptl. Biol. Med. 107: 786, 1961. SCHREINER, G. L.: Effect of heart rate on cardiac work, myocardial oxygen consumption and coronary blood flow in the dog. Acta Physiol. Scand. 42: 185, 1958. 14. FORTUIN, N. J., PITT, B., AND KAIHARA, S.: Distribution of regional myocardial blood flow in the dog (abstr.). Circulation 38: 77, 1968. 28. BRAUNWALD, E., SARNOFF, S. J., CASE, R. B., STAINSBY, W. N., AND WELCH, G. H., JR.: Hemodynamic determinants of coronary flow: Effect of changes in aortic pressure and cardiac output on the relationship between myocardial oxygen consumption and coronary flow. Am. J. Physiol. 192: 157, 1958. 15. HAMMOND, G. L., AND AUSTEN, W. G.: Drainage patterns of coronary arterial flow as determined from the isolated heart. Am. J. Physiol. 212: 1435, 1967. 16. Morn, T. W., DRISCOL, T. E., AND ECKSTEIN, R. 29. KATZ, L. N., JOCHTM, K., AND BOHRNING, A.: W.: Thebesian drainage in the left heart of the dog. Circulation Res. 14: 245, 1964. Effect of the extravascular support of the ventricles on the flow in the coronary vessels. Am. J. Physiol. 122: 236, 1938. 17. SEGRE, C , AND SILBERBERG, A.: Radial particle displacements in poiseuille flow of suspensions. Nature 189: 209, 1961. 30. LOVE, W. D., AND BURCH, G. E.: Differences in the rate of Rb 86 uptake by several regions of the myocardium of control dogs and dogs receiving Z-norepinephrine or pitressin. J. Clin. Invest. 38: 479, 1957. 18. BELLHOUSE, B. J., BELLHOUSE, F. H., AND REID, K. A.: Fluid mechanics of the aortic root with application to coronary flow. Nature 219: 1059, 1968. 19. SPENCER, F. C , MERRILL, D. L., POWERS, S. R., AND BING, R. J.: Coronary blood flow and cardiac oxygen consumption in unanesthetized dogs. Am. J. Physiol. 160: 149, 1950. 20. MAXWELL, G. M., CASTILLO, C. A., CRUMPTON, C. W., AND ROWE, G. G.: Hyperthermia: Sys- temic and coronary circulatory changes in the intact dog. Am. Heart J. 58: 854, 1959. 21. 22. MAXWELL, G. M., CASTILLO, C. A., WHITE, D. H., JR., CRUMPTON, C. W., AND ROWE, G. G.: 31. LEVY, M. N., AND DEOLIVEIRA, J. M.: Regional distribution of myocardial blood flow in the dog as determined by Rb 80 . Circulation Res. 9: 96, 1961. 32. PHIBBS, R. H., WYLER, F., AND NEUTZE, J.: Rheology of microspheres injected into circulation of rabbits. Nature 216: 1339, 1967. 33. ESTES, E. H., ENTMAN, M. L., DIXON, H. B., AND HACKEL, D. B.: Vascular supply to the left ventricular wall. Am. Heart J. 71: 58, 1966. 34. MOIR, T. W., AND DEBRA, D. W.: Effect of left Induced tachycardia: Its effect upon the coronary hemodynamics, myocardial metabolism, and cardiac efficiency of the intact dog. J. Clin. Invest. 37: 1413, 1958. ventricular hypertension, ischemia and vasoactive drugs on the myocardial distribution of coronary flow. Circulation Res. 21: 65, 1967. ROWE, G. G., CASTILLO, C. A., MAXWELL, G. M., WHITE, D. H., JR., FREEMAN, D. J., AND 35. CUTARELLI, R., AND LEVY, M. N.: Intraventricu- CRUMPTON, C. W.: Effect of mecamylamine on coronary flow, cardiac work, and cardiac efficiency in normotensive dogs. J. Lab. Clin. Med. 52: 883, 1958. 23. GOODALE, W. T., AND HACKEL, D. B.: Measure- ment of coronary blood flow in dogs and man Circulation Research, Vol. XXV, November 1969 lar pressure and the distribution of coronary blood flow. Circulation Res. 12: 322, 1963. 36. PALMER, W. H., FAM, W. M., AND MCGREGOR, M.: Effect of coronary vasodilation (dipyridamole-induced) on the myocardial distribution of tritiated water. Can. J. Physiol. Pharm. 44: 777, 1966. 595 TOTAL AND REGIONAL CORONARY BLOOD FLOW from rate of myocardial nitrous oxide desaturation. Circulation Res. 1: 502, 1953. 10. NEUTZE, J. M., WYLER, F., AND RUDOLPH, A. M.: Use of radioactive inicrospheres to assess distribution of cardiac output in rabbits. Am. J. Physiol. 215: 486, 1968. 11. 24. FOLTZ, E. L., PAGE, R. G., SHELDON, W. F., WONG, S. K., TUDDENNAM, W. J., AND WEISS, A. J.: Factors in variation and regulation of coronary blood flow in intact anesthetized dogs. Am. J. Physiol. 162: 521, 1950. REYNOLDS, S. R. M., KIRSCH, M., ANTS BING, R. J.: Functional capillary beds in the beating, KCl-arrested and KCl-arrested-perfused myocardium of the dog. Circulation Res. 6: 600, 1958. 25. O'ROURKE, R. A., FISCHER, D. P., ESCOBAR, E. E., BISHOP, V. S., AND RAPAPORT, E.: Effect of acute pericardial tamponade on coronary blood flow. Am. J. Physiol. 212: 549, 1967. 12. PRINZMETAL, N., SIMKIN, B., BERGMAN, H. C , AND KRUGER, H. E.: Studies on the coronary circulation: II. Collateral circulation of the normal human heart by coronary perfusion with radioactive erythrocytes and glass spheres. Am. Heart J. 33: 420, 1947. 13. MACLEAN, L. D., HEDENSTROM, P. H., AM) KIM, 26. KATZ, L. N., AND FEINBERG, H.: Relation of cardiac effort to myocardial oxygen consumption and coronary flow. Circulation Res. 6: 656, 1958. 27. Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 S. Y.: Distribution of blood flow to the canine heart. Proc. Soc. Exptl. Biol. Med. 107: 786, 1961. SCHREINER, G. L.: Effect of heart rate on cardiac work, myocardial oxygen consumption and coronary blood flow in the dog. Acta Physiol. Scand. 42: 185, 1958. 14. FORTUIN, N. J., PITT, B., AND KALHARA, S.: Distribution of regional myocardial blood flow in the dog (abstr.). Circulation 38: 77, 1968. 28. BRAUNWALD, E., SARNOFF, S. J., CASE, R. B., STAINSBY, W. N., AND WELCH, G. H., JR.: Hemodynamic determinants of coronary flow: Effect of changes in aortic pressure and cardiac output on the relationship between myocardial oxygen consumption and coronary flow. Am. J. Physiol. 192: 157, 1958. 15. HAMMOND, G. L., AND AUSTEN, W. G.: Drainage patterns of coronary arterial flow as determined from the isolated heart. Am. J. Physiol. 212: 1435, 1967. 16. MOIR, T. W., DRISCOL, T. E., AND ECKSTEIN, R. 29. KATZ, L. N., JOCHIM, K., AND BOHRNINC, A.: W.: Thebesian drainage in the left heart of the dog. Circulation Res. 14: 245, 1964. Effect of the extravascular support of the ventricles on the flow in the coronary vessels. Am. J. Physiol. 122: 236, 1938. 17. SEGRE, G., AND SILBERBERG, A.: Radial particle displacements in poiseuille flow of suspensions. Nature 189: 209, 1961. 30. LOVE, W. D., AND BUBCH, G. E.: Differences in the rate of Rb 86 uptake by several regions of the myocardium of control dogs and dogs receiving Z-norepinephrine or pitressin. J. Clin. Invest. 38: 479, 1957. 18. BELLHOUSE, B. J., BELLHOUSE, F. H., AND REID, K. A.: Fluid mechanics of the aortic root with application to coronary flow. Nature 219: 1059, 1968. 19. SPENCER, F. C , MERRILL, D. L., POWERS, S. R., AND BING, R. J.: Coronary blood flow and cardiac oxygen consumption in unanesthetized dogs. Am. J. Physiol. 160: 149, 1950. 20. MAXWELL, G. M., CASTILLO, C. A., CRUMPTON, C. W., AND ROWE, G. C.: Hyperthermia: Sys- temic and coronary circulatory changes in the intact dog. Am. Heart J. 58: 854, 1959. 21. 22. MAXWELL, C. M., CASTILLO, C. A., WHITE, D. H., JR., CRUMPTON, C. W., AND ROWE, G. G.: BERGLUND, E., BORST, H. G., DUFF, F., AND 31. LEVY, M. N., AND DEOLIVEIRA, J. M.: Regional distribution of myocardial blood flow in the dog as determined by Rbsfl. Circulation Res. 9: 96, 1961. 32. PHIBBS, R. H., WYLER, F., AND NEUTZE, J.: Rheology of microspheres injected into circulation of rabbits. Nature 216: 1339, 1967. 33. ESTES, E. H., ENTMAN, M. L., DIXON, H. B., AND HACKEL, D. B.: Vascular supply to the left ventricular wall. Am. Heart J. 71: 58, 1966. 34. MOIR, T. W., AND DEBRA, D. W.: Effect of left Induced tachycardia: Its effect upon the coronary hemodynamics, myocardial metabolism, and cardiac efficiency of the intact dog. J. Clin. Invest. 37: 1413, 1958. ventricular hypertension, ischemia and vasoactive drugs on the myocardial distribution of coronary flow. Circulation Res. 21: 65, 1967. ROWE, G. G., CASTILLO, C. A., MAXWELL, G. M., WHITE, D. H., JR., FREEMAN, D. J., AXD 35. CUTARELLI, R., AND LEVY, M. N.: Intraventricu- CRUMPTON, C. W.: Effect of mecamylamine on coronary flow, cardiac work, and cardiac efficiency in normotensive dogs. J. Lab. Clin. Med. 52: 883, 1958. 23. COODALE, W. T., AND HACKEL, D. B.: Measure- ment of coronary blood flow in dogs and man Circulation Reiearcb, Vol. XXV, November 1969 lar pressure and the distribution of coronary blood flow. Circulation Res. 12: 322, 1963. 36. PALMER, W. H., FAM, W. M., AND MCGREGOR, M.: Effect of coronary vasodilation (dipyridamole-induced) on the myocardial distribution of tritiated water. Can. J. Physiol. Pharm. 44: 777, 1966. 596 37. DOMENECH, HOFFMAN, NOBLE, SAUNDERS, HENSON, SUBIJANTO GHIGCS, D. M., JR., AND NAKAMUBA, Y.: Effect of coronary constriction on myocardial distribution of iodoantipyrine-I131. Am. J. Physiol. 215: 1082, 1968. 38. BRANDI, C , FAM, VV. M., AND MCGREGOR, M.: Measurement of coronary flow in local areas of myocardium using xenon133. J. Appl. Physiol. 24: 446, 1968. Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 Circulation Research, Vol. XXV, November 1969 Total and Regional Coronary Blood Flow Measured by Radioactive Microspheres in Conscious and Anesthetized Dogs RAUL J. DOMENECH, JULIEN I. HOFFMAN, MARK I. NOBLE, KENNETH B. SAUNDERS, JAMES R. HENSON and SUJANTO SUBIJANTO Downloaded from http://circres.ahajournals.org/ by guest on April 29, 2017 Circ Res. 1969;25:581-596 doi: 10.1161/01.RES.25.5.581 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1969 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/25/5/581 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/