Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Biochemistry wikipedia , lookup
Germ theory of disease wikipedia , lookup
Functional specialization (brain) wikipedia , lookup
Holonomic brain theory wikipedia , lookup
Central nervous system wikipedia , lookup
Acquired characteristic wikipedia , lookup
Neurodegeneration wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
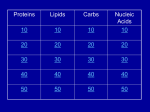
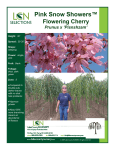
PINK DISEASE SUPPORT GROUP PO Box 5120, Eagleby, Qld., Australia, 4207. [email protected] http://www.pinkdisease.org PINK NEWS - MARCH, 2009 Dear Everyone, With all the drama that’s been going on here in Australia and overseas, all I can say is that I hope you are all healthy, happy, financially secure and safe. This year the group will be doing things a bit differently. As you will see from Heather’s Newsletter, it is probably her last newsletter because she has time consuming work and personal commitments. She is still the Treasurer of the group and will always be a “Pink Disease Hero” for her continuing work in raising awareness of Pink Disease. I suspect a lot of the interest in Pink Disease that has occurred in the last couple of decades is due to Heather’s hard work. I’ll still be doing newsletters this year but there won’t be a regular quarterly schedule because I have got so far behind with my Pink Disease and other commitments due to medically unsuitable housing and ill health. Now that I’ve moved to a more suitable abode, I’m hoping my health will pick up and I’ll gradually manage to get all the things on my lengthy “to do” list done. One of the things that has been a permanent fixture on the list for some years is the writing of a Pink Disease book containing all the information that has come my way over the years. Because newsletters won’t be regular, no membership fee will be charged this year. People who were paid members in 2008 will get any newsletters that I do. You are, as always, welcome to make a donation to the Group either by cheque, money order or PayPal – http://www.pinkdisease.org/donation.htm. Because of Heather’s busy schedule, any donations should be sent to the Group at PO Box 5120, Eagleby, Qld., 4207 because I’ll be doing the banking this year. Donations of 55 cent Australian stamps are also acceptable. This newsletter set includes this newsletter, Heather’s newsletter, survey documents (see below), a Pink Disease pamphlet, and a Pink Disease handout. Everything can be found on the website at http://www.pinkdisease.org/newsletters2009.htm. HAVE YOU HAD MERCURY CHELATION? Dr. Andrew Cutler, the author of “Amalgam Illness – Diagnosis and Treatment” would like to hear from anyone who has had mercury chelation. His email address is [email protected]. The book is well worth a read because it has lots of information on mercury toxicity and detoxification. More details of the book can be found at http://www.noamalgam.com. 1 th HAPPY 20 BIRTHDAY! The Pink Disease Support Group started from humble beginnings 20 years ago this month – all praise to Heather, for a job cleverly and well done. Since the Group’s beginning, it has received over 1200 completed Pink Disease Surveys and numerous other bits of information from those who survived Pink Disease. It is now well accepted that Pink Disease was caused by exposure to mercury, usually in the form of mercurous chloride (calomel) found in many teething, soothing and calming powders up until the mid 1950s. It is also a fact that only 1 in 500 babies who were given these powders got Pink Disease. This means that either mercury was accumulating in the body faster than it was being removed or mercury is more toxic to Pinkies for some reason. It is almost certain that there is a factor that predisposes babies to Pink Disease. That factor could be one or more or all of the following: Genetic – the gene that makes the transport protein that removes mercury from the body may be absent or defective. Epigenetic – the mercury removal gene isn’t faulty but for some reason it is switched off. Some other factor, such as an illness or medication, is disrupting the mercury removal process. The exposure to mercury is disrupting an essential bodily process resulting in the symptoms of Pink Disease Developmental – babies go through a massive amount of development in the first two years of life – the younger and less developed a baby is, the more toxic mercury is to it. It could be that there was a delay in some aspect of the development of babies that got Pink Disease. The conclusions of Professor Donald Cheek, who did extensive research on the physiology of Pink Disease, can be found in the Pink Disease handout. Survey data and other information received also shows that while some people have no ill effects from having had Pink Disease, most people have some problems that can be related to the Disease. Unfortunately, some people have very severe and disabling problems. Another very important part of the information received relates to the descendants of Pink Disease survivors – quite a number have ‘pink disease’ type symptoms, and an assortment of odd health and/or developmental problems. To date, the Group hasn’t done a formal survey about the health of the children, grandchildren or great-grandchildren of those who had Pink Disease. I’m pleased to say that Swinburne University of Technology is currently carrying out a research project to investigate certain aspects of the health of Pink Disease survivors and their descendants. The project consists of a two part survey – one part asks about Pink Disease Survivors and the other part wants to know about their descendants (if any). The Survey can be filled in either by the Pink Disease Survivor, or if they are unable to complete the survey, then another person can complete it on their behalf. This combined Pink Disease Survivor/Descendants survey is extremely important partly because it will give us some indication about what type of genetic or other shortcoming caused just 1 in 500 babies exposed to mercury to get the disease; how heritable it is; and how many descendants have problems that might relate to mercury sensitivity. I want to urge you to complete and return this survey. It can be anonymous if you wish but if you would like to enter the prize draws, you will need to fill in your personal details on the final page of the survey. Swinburne has 10 x $75.00 vouchers as prizes. The Pink Disease Support Group is offering an additional prize of $250.00. The Group is offering the additional prize in the hope that it will inspire you to complete the survey because we need the information that this Survey, which covers the descendants of people who had Pink Disease, will provide. It is a gap in our existing knowledge. As the years pass, the number of Pink Disease survivors is falling. We therefore need to get this research done while we still can. This Survey is being carried out by Swinburne researchers, Ms. Kerrie Shandley and Associate Professor David Austin. Although there are a lot of the specific questions on the descendants’ survey, a very 2 important column called “other conditions” is included. In that column, you can include anything (even if it minor) that your descendants suffer from. Another very important box is marked “Additional Comments”. You can put anything that you think might be of interest in this box. For Pinkies who don’t have biological descendants, but have other relatives such as siblings, nieces or nephews who have any of the problems mentioned in the survey or which are unusual or might relate to Pink Disease or mercury sensitivity, please put the details in this box as well. Kerrie Shandley and David Austin, state they “…are passionate about not letting the disastrous effects of mercury on living beings be forgotten” and this is a sentiment that both Heather and I share. Keeping the story of Pink Disease alive will help stop a preventable epidemic like Pink Disease happening again. The Pink Disease epidemic began in the 1880's. Why did the Pink Disease epidemic begin then: In the 1850’s, the use of mercury in medicines became unfashionable. During the 1880’s, the use of mercury in the form of calomel in teething powders became commonplace. Although knowledge of the dangers of mercury and the symptoms of mercury toxicity had been almost universal among the doctors of the 1850’s, by the 1880’s, doctors were no longer familiar with these dangers and symptoms so they did not recognize Pink Disease for what it was – a type of mercury toxicity. Remember – you don’t have to put your name and address on the survey if you would like your and/or your descendant’s difficulties to remain private. Although Swinburne will be giving me a copy of the survey results, I will not be getting anything that identifies a specific individual. CLOVER’S DYSTONIA One of our members who had been struggling to get an accurate diagnosis of her speech/swallowing problem for over two years has at last been diagnosed by a neurologist as having a form of dystonia. She has been prescribed medication and advises that she really notices the difference in her speech and especially her swallowing. She would like to hear from anyone who has had problems with their speech and swallowing. Please contact me and I will put you in touch with her. Below is some information about dystonia from the article “Cramps, Spasms & Dystonia” in Pink News January, 2007 – http://www.pinkdisease.org/news0107.htm. Dystonia is a neurological movement disorder that causes muscles in the body to contract or spasm involuntarily. The involuntary muscle contractions cause twisting, repetitive and patterned movements as well as abnormal postures. Dystonic spasms can last for a few seconds or for weeks. There are many different types of dystonia and there are a number of different causes of dystonia but the causes are not fully understood. It is thought that dystonia may be caused by a chemical imbalance in a particular area of the brain called the basal ganglia where the messages to initiate muscle contractions are believed to originate. Dopamine is the neurotransmitter that regulates communication between the nerves within the basal ganglia and a malfunctioning dopamine system may be involved in some forms of dystonia. Focal dystonia affects one part of the body such as the eyes, neck, a limb or the voice. If a larger part of the body, such as the neck and arms is affected, it is called segmental dystonia. Hemi-dystonia affects the arm and leg on the same side of the body. If 2 or more unrelated parts of the body are involved, it is called multifocal dystonia. Generalised dystonia is wide-spread dystonia. Primary dystonia is of the genetic inherited type. Secondary dystonia is caused by small areas of brain damage. The brain damage can be caused by reduced oxygen at birth, small strokes, toxins, infections, tumours or brain injuries. The spasms and cramps caused by dystonia can be a minor annoyance such as writers’ cramp, or disabling, disfiguring and very, very painful. Treatment for dystonia includes surgery, sedatives, botox (to paralyse the contracting muscle), physical therapy, dopamine and counselling. 3 MANAGING BREATHLESSNESS One of the most common symptoms of lung disease is breathlessness. This can range from being more breathless than usual when walking up a slope, to being breathless when showering or even talking. There are a number of reasons that people feel breathless or short of breath: 1. Air Trapping: For people with Chronic Obstructive Pulmonary Disease (COPD), there is an increase in the size of the lungs due to air trapping. The air sacs (alveoli) are floppy and less elastic and this makes it difficult to get air out, so it becomes trapped in the lungs. The air tubes or airways may be narrowed due to swelling and mucus and this also makes it difficult to get air out. Air trapping makes it harder work to breathe and breathing can feel uncomfortable. 2. Stiff Lungs: For people with pulmonary fibrosis, the lungs are stiff and this makes it difficult to get air in and out. The breathing muscles have to work extra hard to move air in and out of the lungs. Breathing is shallower and faster, particularly when exercising. Stiff lungs increase the effort involved with breathing and it can be uncomfortable. 3. Weak and out of condition arm and leg muscles: When the arm and leg muscles are out of condition and weak they produce more waste product (lactic acid). This causes aching in the muscles. The body converts this waste product to carbon dioxide and gets rid of it by breathing harder. Weak and out of condition arm and leg muscles cause harder breathing and more breathlessness on activity. 4. Weak breathing muscles: In patients with COPD, the diaphragm is weaker and flatter (it should be dome shaped). The diaphragm doesn’t have much room to move, so the muscles of the neck and shoulders have to help with breathing, making it uncomfortable. A flattened, weak diaphragm makes breathing difficult. All of the above factors contribute to breathlessness. Anxiety or panic and feeling low (depressed) can make the feeling of breathlessness worse. When you become anxious, your breathing becomes faster and shallower. This allows less time for the air to get out and thus, contributes to air trapping and further breathlessness. A number of factors can help you manage your breathlessness: 1. Medication: Regular and correct use of your medication helps to keep airways open and allows air out. 2. Exercise: Regular exercise, such as walking, helps to improve muscle conditioning and fitness. Fitter, more efficient muscles produce less waste product and thus, activity causes less breathlessness. Pulmonary rehabilitation programs run by physiotherapists include exercises specifically designed for people with lung disease. These programs have been shown to reduce breathlessness and make people feel better. 3. Breathing techniques: Simple, relaxed breathing slower and deeper – during stressful situations may help alleviate the feeling of breathlessness. Pursed-lip breathing (pursing the lips together on the breath out) helps to keep “floppy” airways open and may help to relieve breathlessness. 4. Positioning: Leaning forward and bracing your shoulder girdle can help your breathing as the breathing muscles are in a better position to pull up the ribs. These positions may be helpful for you to recover your breathing after doing some physical activity. Some people find that leaning forward and supporting their arms (like when pushing a shopping trolley) causes less breathlessness and they can walk further. A four wheeled seated walker may help people who experience this. 5. Breathing muscle training: There is a special device that can train the muscles that help us to breathe in. However, to be beneficial, this needs to be supervised by a health professional. 6. Other strategies: Relaxation can help stop the cycle of anxiety and breathlessness. Some people report that air movement on their face, for example, from a fan, helps to reduce breathlessness. Sometimes thinking of something else – something pleasant and safe – takes the focus off breathlessness and can relieve the sensation. Whatever you do, don’t give up and stop doing things as this will contribute to the cycle of inactivity and further breathlessness. 4 SOURCE: “Managing Breathlessness” by Nola Cecins and Sue Jenkins, courtesy of Lungnet, February, 2009. Also from Lungnet, February, 2009: In November, The Australian Lung Foundation launched a new Access Economics report detailing the growing problem of Chronic Obstructive Pulmonary Disease (COPD), including its economic impact upon Australians and cost effective solutions to reduce the burden of this disease. The Report estimated that COPD, a disease which is more common in any year than most types of cancer, heart disease and diabetes, would cost Australia nearly $100 billion in 2008. The Report also stated that 2 million Australians (10% of the population) currently have COPD with around 45% of those having the disease in its early stages. Many, if not most of those with early stage COPD were not aware they had the disease. If COPD isn’t treated in its early stages, it is much more likely to progress to a moderate to severe form of COPD. The report also stated that early diagnosis, combined with disease management programs at the early stage could reduce COPD’s burden, improving quality of life, slowing disease deterioration, reducing mortality and importantly keeping people out of hospital. NOTE: Lungnet has updated its Bronchiectasis Brochure. The brochure can be downloaded from http://www.lungfoundation.com.au//index2.php?option=com_content&task=view&id=75&pop=1&page=0&Itemid=80 INNER SPACE – ABOUT THE BRAIN (PART 1) Our inner space, the brain, was a substantially undiscovered part of human biology until 20 years ago. Improved imaging tools and the use of functional MRI, have resulted in an explosion of knowledge about how the brain functions. Research is ongoing. Purpose: The brain is the most complex organ in the body and it has to be because it regulates almost all human activity. It’s tasks include: Control of the central nervous system using the cranial nerves and the spinal cord, and the peripheral nervous system. Control over involuntary actions such as respiraton, digestion, and heart rate via the autonomic nervous system Control over our voluntary or conscious actions including thought, reason, perception, imagination, interpretation, abstraction and language. Control of our emotions (most of the time) Receiving and processing masses of information from the world around us via the eyes, ears, nose, and the senses of taste and touch Handling our physical motion. Structure: The living brain is a soft, red, jelly-like mass of tissue about the size of a small cauliflower weighing about 1.4 kilograms and having a volume of about 1.6 litres. Grey and white matter are commonly used when describing the brain but they refer to the colour of a preserved brain, not a living one. The brain is suspended in cerebrosinal fluid and this fluid also fills the spaces within the brain. The fluid protects the brain and spinal cord from shock – basically, cerebrosinal fluid is the brain’s ‘shock absorber’. Major parts of the brain are: The Brain Stem controls reflexes and autonomic functions such as heart rate and blood pressure, movement of the limbs and functions carried out by bodily organs (viscera) such as digestion and urination. 5 The Cerebellum is at the back of the brain and it processes information from the vestibular system indicating position and movement and uses this information to co-ordinate limb movement. The vestibular system controls balance, posture, and spatial orientation. It also stores patterns of activity, such as movements, habits and frequently repeated actions, so that we can do them without thinking about them. The Hypothalamus and Pituitary Gland also control visceral functions, including maintenance of body temperature and behavioural responses such as hunger, thirst, aggression and pleasure. The Cerebral cortex (cerebrum) has two hemispheres connected via a large fibre tract called the ‘corpus callosum’, the cortex, and structures such as the basal ganglia, amygdala and hippocampus. The cerebral cortex is the largest part of the human brain and contains all the bits that receive and interpret information received via the senses, initiate movement, analyse information, and that allow us to reason, remember and to experience and control emotions. The cortex is the surface area of the brain and is about 2, 000 centimetres squared. It can’t fit into the skull unless it is folded up - the folds are called gyri and the grooves are called sulci. Several large grooves divide the cortex into a number of lobes with different functions. The Frontal and Prefrontal Lobes control conscious thoughts, decisions, planning, conceptualization, attention, working memory and social emotions such as empathy, regret and morality and motor skills including speech. The Parietal Lobe receives and processes sensory input from the body such as touch and pain and is involved with movement, position, orientation and calculation. The Occipital Lobe receives and processes visual information directly from the eyes The Temporal Lobe processes auditory information from the ears enabling us to comprehend speech and other sounds. The amygdala, which controls social and other emotions, and the hippocampus, which stores short term memory, are both located in the temporal lobe. From an anatomical point of view, the brain has 3 parts: The forebrain (higher brain)which includes the cerebral cortex and controls higher functions. The midbrain is involved in relaying information. It has pathways to the parts of the brain involved in movement, and also selects and catalogs information. If the substantia nigra in the midbrain is damaged, movements will be tremored, as with Parkinsons Disease. The hindbrain (lower brain) is made up of the spinal cord and brain stem and along with the midbrain, is involved with unconscious, autonomic functions. Consciousness: There appears to be no localized centre of conscious control. Our consciousness is an ‘emergent’ property that is derived from interaction between the numerous systems within the brain. Structure – Nerve Cells: The brain has 100 billion nerve cells (neurons) and each of these nerve cells makes connections with an average of 10,000 other nerve cells via synaptic pathways. This means that our brains have around a million billion connections. The brain contains both grey matter, white matter and glial cells. The grey matter is the bodies of our nerve cells while the white matter is the axons and dendrites that spread out from the cell body. Our brains contain a thousand billion glial cells which amplify the signal from nerve cells. Glial cells are as important as nerve cells in mental calculations. Memory, Personality and the Brain: Our brains create one million new connections between nerve cells every second of our lives. The pattern and strength of these connections constantly changes and as a result, no two brains are alike. Our memories are stored within these changing patterns of interconnection. Our habits and personalities are shaped by reinforcing certain patterns of brain activity and the weakening of other patterns that aren’t being used regularly. With habits and other patterns of activity, it is basically use it or lose it. The saying ‘practice makes perfect’ makes perfect sense because practice is a way of strengthening the pattern of brain activity that enables you to do something, for example, play the piano, drive, knit or do calculus. Because connecting pathways weaken when we don’t use them, if we stop indulging in a bad habit such as playing the pokies obsessively and stop thinking about the bad habit, the pathways won’t get used and hopefully the bad habit will be broken (in theory, anyway). One of the 6 reasons habits of the addictive variety – gambling, smoking, taking drugs (both legal and illegal) – are so hard to break relates to the chemical receptors in our brains – more about them in the next newsletter. Note: Rehearsing or imagining something in our mind also uses and strengthens pathways. Memories are stored as impressions and emotions rather than facts and what is stored is often reinterpreted or changed over time. This is why 100 witnesses or spectators have 100 different versions of an event. Because the human brain has so many nerve cells and connections between nerve cells, it can make an infinite number of unique pathways in our brain in which to store our memories, habits and personalities. A synaptic pathway is simply a nerve cell which ‘sends’ information to other nerve cells which in turn send information to more nerve cells. Brain structure is partly shaped by genes, but with one million new connections between nerve cells being made very second, brain structure is shaped largely by experience. To create the synaptic pathways within which our memories, personality and habits are stored, the nerve cells of our brain must be able communicate with each other. One method is by the release and capture of chemicals. The picture to the left is a basic sensory nerve cell. The process of transmission is as follows: 1. An electrical signal called an ‘action potential’ is initialized in the axon hillock and it travels down the axon to the axon terminal, that is, the nerve cell ‘fires’. 2. The axon terminal releases neurotransmitter chemicals to the synapse. 3. The chemicals drift across the synaptic cleft which is the gap between the synapse and the chemical receptors of the dendrites of the adjacent nerve cell. 4. The binding of the chemical to the chemical receptor causes the nerve cell to do something, stop doing something, or to adjust what it is doing. It is the chemical receptor rather than the neurotransmitter chemical that is responsible for the action of the neurotransmitter chemical. Nerve cells perform a wide variety of functions and as a result, there are many different nerve cells with different shapes, sizes and electrochemical properties. For example, although many nerve cells do just have one axon as shown in the diagram, the axon usually splits into numerous branches and this allows one individual nerve cell to communicate with numerous other nerve cells at the same time. 7 There are a multitude of neurotransmitter and neuromodulator chemicals including glutamate, dopamine, acetylcholine, noradrenalin, serotonin and endorphins. Some of these neurochemicals work at the synapse by passing chemical ‘messages’ from release sites to the receptors as mentioned above. Basically, this is nerve cell to nerve cell/s communication. Other neurochemicals spread their ‘message’ out more widely – like a radio signal – and make whole parts of the brain more or less sensitive. There are also, electrically conductive junctions between some cells called electrical synapses. These don’t use neurotransmitters. There will be more about neurotransmitters in the next newsletter. Brain Titbits: 75% of the glucose (blood sugar) created by the liver is used by the brain. 20% of the oxygen we inhale is also consumed by the brain. The brain creates more nerve cells (as distinct from connections) at certain times during our lives namely in the first 2 or 3 years, at puberty and in early adulthood. Much of the brain is made of fat, including cholesterol. Unfortunately, some cholesterol reducing medicines, especially the statins, reduce the cholesterol in the brain as well as the body so the brain doesn’t function as effectively as it should. Dendrites can’t secrete neurotransmitter chemicals and the axon has no chemical receptors. Therefore, electrical transmission is almost exclusively in one direction. If all the nerve cells in the brain fired at once, the electrical overload would cause a seizure. As a result, only 10% of the brain’s nerve cells are firing at any given time. Main Sources: 1. 2. 3. 4. “Human Brain” – http://en.wikipedia.org/wiki/Human_brain “How Your Brain Works” – http://health.howstuffworks.com/brain.htm “Neuron” – http://en.wikipedia.org/wiki/Neuron “Instant Expert: The Human Brain” = http://www.newscientist.com/article.ns?id=dn9969 FABULOUS FATS & OILS In previous newsletters protein and its essential roles in the body were discussed and in the last newsletter, carbon and those much maligned carbohydrates were praised for their crucial role as a supply of energy for the body. In this newsletter, the bodily requirement for another much maligned and essential food group will be discussed, lipids, better known as fats and oils. Lipids come in 3 varieties: 1. Triglycerides are made of 3 fatty acids attached to a backbone made of glycerol. Fatty acids are made up of a tail, which is a chain of between 4 and 24 carbon and hydrogen atoms, and a head made of carbon and oxygen atoms. There are a lot of different fatty acids and each type has a different arrangement and number of carbon and hydrogen atoms. 1. Phospholipids have 2 fatty acids and 1 phosphate group attached to the glycerol backbone. 2. Sterols are made from interconnecting rings of carbon. Triglycerides are the common dietary fats and oils that we eat and the properties of a particular fat or oil, such as flavour and whether it is a solid or liquid at room temperature, or is saturated, monounsaturated, or unsaturated, depends on the types of fatty acids it is made of: Saturated fatty acids are mostly solid at room temperature and have no gaps in the hydrogen/carbon tails of their component fatty acids. Sources include birds and animals and their products such as eggs and dairy as well as coconuts and palm oil. Research suggests that saturated fat is more likely to cause weight gain and that some types of saturated fatty acids also elevate blood cholesterol Monounsaturated fatty acids are usually liquid at room temperature and have one hydrogen missing from their tail. 8 Polyunsaturated fatty acids are also normally liquids and have two or more missing hydrogen atoms from their tails. Most plants and fish oils are unsaturated because the missing hydrogen atom/s gives the fatty acids they are made of a kink so the fatty acids cannot pack as closely together as saturated fatty acids do. As a result, they remain liquid at room temperature. The human body can make all the fatty acids it needs from carbohydrates except for linoleic acid (LA) which the body converts into omega-6 fatty acids and alpha-linoleic acid (ALA) which the body converts into omega-3 fatty acids and arachidonic acid which the body can make from LA. Because the body cannot make LA or ALA, they are called “essential fatty acids”. Vegetable oils such as corn, safflower and soybean oils, nuts and seeds are good sources of LA. Sources of ALA include flax seed oils. Fish contain the omega-3 derivatives, EPA and DHA, and these more beneficial that omega-3 fatty acids in some instances. Canola Oil is the best source of both LA and ALA combined. There has been quite a bit of research and conjecture about the problems caused by an imbalance between the intake of omega-3 fatty acids and omega-6 fatty acids. It has been suggested that the current Western diet includes too much omega-6 fatty acids and not enough omega-3 fatty acids – at a ratio of 7:1. In hunter-gatherer times, the human diet included roughly even amounts of the omega-3 and omega-6 fatty acids but the ratio started to tip in favour of a higher omega-6 intake when agriculture became common 10,000 years ago. About 50 years ago, cattle began to be fed more grains than grass and margarine replaced butter as the commonly used spread. The gap between the intake of omega-3 and omega-6 fatty acids widened further and is currently estimated at 7 to 1 in favour of omega-6 fatty acids. This unbalanced intake of essential fatty acids is believed to be the cause of increased rates of cancer, heart disease, diabetes, allergies, depression and other ailments. Our cells need the correct balance and types of fatty acids to function properly. The explosion of fish oil products on the market at the moment no doubt relates to publicity about the benefits of omega-3 fatty acids. A detailed discussion about what essential fatty acids do and the importance of getting the balance right can be found in the article “Fats You Need – Essential Fatty Acids” by Ben Best http://www.benbest.com/health/essfat.html. The body breaks down lipids into their component parts, glycerol and free fatty acids, for use by the body. Lipids are also stored in the body as triglycerides in the liver and muscles in a form called glycogen; as padding and insulation under the skin, and as a protective cushion around the organs. When the body needs energy, the liver converts glycogen to glucose which is absorbed by the body and converted into energy via glycolysis in the same manner that glucose from carbohydrates is converted (see the November, 2008 newsletter – http://www.pinkdisease.org/news1108.htm). Carbohydrates are easier to convert to glucose and digest than fat is so if there is a lot of carbohydrate in the diet, much of the dietary fat is stored. Phospholipids have an interesting property – the phosphate head is water loving but the fatty acid tail hates water. As a result, phospholipids in water line up in a bilayer with the water loving heads facing outwards and the water hating tails facing inwards protected from the water. The membranes surrounding our cells and many cellular structures are made of phospholipid bilayers with cholesterol between the layers to keep them fluid. Phospholipid bilayer – cell membrane 9 Lecithen is the most well known phospholipid. It’s phosphate group is choline. Lecithen can be made by the liver so it is not classed as an essential nutrient so it does not need to be added to the diet. Sterols include cholesterol which is a component of sex hormones, adrenal hormones and Vitamin D. As mentioned above, cholesterol is a normal component of body tissues and it is also an important part of the brain, the nervous system and blood. Ninety percent of the cholesterol in the body is part of the cellular structure or involved in cellular metabolism. Cholesterol is also needed for the digestion and absorption of dietary fats (in the form of bile); cellular maintenance; and is packed into transport molecules called lipoproteins, namely, HDL cholesterol, LDL cholesterol and VLDL cholesterol. LDL and VLDL cholesterol are the bad cholesterols that clog the arteries leading to heart disease and vascular problems. Most of the cholesterol used by the body is made by the liver from carbohydrates and fats – each day about 2 grams of cholesterol are made. Dietary cholesterol comes from offal, shellfish, egg yolks, fatty meat and full fat dairy products. At one stage, egg yolks were thought to be one of the villains that caused high cholesterol. Research by Purdue University found that while eating egg yolks made no significant difference to blood cholesterol, failure to exercise did make a difference – that is, lack of exercise is one of the villains that raises blood cholesterol. Note – people who have inherited disorders that cause high cholesterol should remain cautious about egg yolks and other cholesterol containing foods. Omega-3 and omega-6 fatty acids are both needed for the breakdown of cholesterol. Benefits of Lipids : They are an important dietary energy source and provide 9 calories of energy per gram They supply essential nutrients Vitamins A, D. E & K are fat-soluble vitamins and need to be transported with lipids so that they can be digested and absorbed. Lipids help calcium absorption by making Vitamin D available. Slow down digestion which satisfies hunger longer They help keep the skin, scalp and hair healthy. The body can store them and convert them to energy when other sources of energy are unavailable. Fats are also used to store undesirable substances including chemicals, viruses & bacteria that have reached unsafe levels in the blood stream. This includes mercury. This helps protects the body until the undesirable substance can be metabolized or removed from the body. I probably don’t need to talk about the dangers of lipids because the ailments associated with excess fat are in the media all the time. The body can store an unlimited supply of fat under the skin and around the organs. This causes obesity and increases the risk of getting numerous ailments including cardiovascular disease, diabetes, high blood pressure, high cholesterol and high triglycerides, and worsens the symptoms of arthritis and asthma. I’ve mentioned the problems associated withan imbalance between the intake of omega 3 and omega 6 fatty acids above and there is a discussion about trans fatty acids below. Fat Trivia: 1. This years World Congress of Fats and Oils is meeting in Sydney. 2. Nearly half of the dry weight of the brain is fat and a quarter of that fat is cholesterol. 3. The most commonly used vegetable oils in the world are palm and soy oil, followed by canola and sunflower oil. 10 4. In the absence of water, or if the kidneys are faulty, fats won’t be absorbed if there is no carbohydrate. This is the basis of the Atkins Diet which is extremely (possibly dangerously) low in carbohydrates. Industrial uses of vegetable oils include soap, perfumes, personal care products, candles, paints, insulation in the electrical industry, biodegradable hydraulic fluids and lubricants and biodiesel. Biodiesel is becoming increasingly popular as a way of reducing the carbon dioxide pollution of regular diesel and petrol. Unfortunately the use of food crops in the production of biodiesel has increased the worldwide food shortage somewhat. About trans fats - naturally occuring lipids are almost universally in the ‘cys’ configuration. Processing vegetable oils to convert them to margarines is called hydrogenation because in involves adding the hydrogen atoms that are missing from unsaturated fatty acids. Hydrogenation causes the normal fatty acids to convert to ‘trans’ fatty acids – that is fatty acids with bonds occuring on the opposite side of the chain. Using oil for frying also converts some of the natural cys bonds into trans bond, and re-using oil, converts even more of them to trans fatty acids. The problem with trans fatty acids is that there is mounting evidence that the human body does not react to them favourably. In particular, trans fatty acids are carcinogenic, they significantly increase the risk of heart disease and have been suggested as a causative factor in macular degeneration. MAJOR SOURCES: 1. 2. 3. 4. 5. 6. “Fat”, “Trans Fat”, “Fatty Acid” and “Vegetable Fats and Oils” all from Wikipedia – http://en.wikipedia.org/wiki/ “Fats You Need – Essential Fatty Acids” by Ben Best – http://www.benbest.com/health/essfat.html “Fats” – http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/F/Fats.html “Lipids: Fats, Oils, Waxes, etc.” – http://biology.clc.uc.edu/Courses/bio104/lipids.htm “Organic Chemistry and Biochemistry” http://faculty.clintoncc.suny.edu/faculty/michael.gregory/files/bio%20101/bio%20101%20lectures/biochemistry/biochemi.htm “The Nutrition Almanac”, 4th Edition, G. J. & J. D. Kirschmann. DRY MOUTH SYNDROME About 25% of people suffer from dry mouth syndrome, or xerostomia, which is caused by insufficient saliva in the mouth. The salivary glands make saliva which is pumped into the mouth along salivary ducts. There are a number of different salivary glands. The parotid glands are near the ears, the submandibular glands are under the tongue on both sides of jaw, the sublingual gland is on the floor of the mouth and there a number of other small salivary glands in the mouth, cheeks and throat. Saliva has a number of important attributes. It : helps destroy viruses; has anti-fungal properties; makes swallowing easier by moistening food; assists in the making of certain sounds for speech; increases the sensation in the mouth allowing the experience of pain, food texture and taste; contains phosphorus and calcium which is required for the ongoing rebuilding of tooth enamel; and its reduces the number of tooth decaying bacteria. There are many symptoms that can be caused by a dry mouth. These include a rough, dry tongue; trouble chewing or swallowing; mouth ulcers; dry, cracked lips; split skin at the corners of the mouth; burning sensation in the mouth or on the tongue; the tongue sticking to the top of the mouth; bad breath; excess tooth decay; oral thrush; and thick saliva. Other symptoms, such as dry, itchy eyes, nose or throat; coughing; joint pains or stiffness; hoarseness; constipation; and a reduced sense of smell, can also accompany dry mouth syndrome. Dry mouth can be caused by a lot of things. Six hundred drugs are known to cause the problem – examples include antihistamines, blood pressure medicine, sedatives, decongestants, antidepressants, painkillers and illegal drugs such as cocaine. Another cause is dehydration caused by not drinking enough fluid or by medical problems such as chronic diarrhoea or kidney failure. It can be caused by salivary duct obstructions; problems with the facial nerves (which control the salivary glands); cancer treatments; breathing through the mouth; diseases such as diabetes, Parkinson’s disease and AIDS; and 11 infections. A number of foods and drinks can cause a dry mouth. These include spicy foods, tea, some herbal teas, some citrus drinks, caffeine, and mints. If you have dry mouth symptoms, then your doctor, chemist or dentist might be able to help. Treatments include changing existing medication that can cause dry mouth for medication that doesn’t cause this (if possible); saliva substitute; surgery for salivary gland or duct blockages; antibiotics and anti-fungals; products that contain salivary enzymes; and the use of preventative measures. Eating chewy foods stimulates saliva, eating watery foods; sipping water regularly and chewing sugarless gum between meals are all helpful. Avoiding crunchy or acidic foods and drinks; cigarettes, alcohol, mint mouth washes; or any food, drink or product that increases the mouth dryness is also a good idea. For those with full or partial dentures, remove them when you sleep. Trivia: If saliva cannot dissolve something, you cannot taste it. Main Sources: 1. “Dry Mouth Syndrome” from the Better Health Channel http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/5bf5f6cf2121c66aca2571ea001ac993/7479683d3cb10028ca25728 70002253a?OpenDocument 2. “Dry Mouth” from MedicineNet – http://www.medicinenet.com/script/main/art.asp?artickekey+43095&pf=3&page=1 Regards, Di Farnsworth, PINK DISEASE SUPPORT GROUP. DISCLAIMER: Everything in this newsletter is for informational & educational purposes only and is generally brief and/or summarised versions of assorted information sources. Although all information is given in good faith, none of it is meant in any way to be medical advice, nor is it meant to replace the services of your own health professional/s. It is important that you make your own informed choices about medical treatment, diets, and amalgam removal and so forth. Please consult your own health professional/s regarding these matters. The Pink Disease Support Group, Heather Thiele and I are not responsible for any adverse effects or consequences from the use of any information, suggestions or materials provided by the Pink Disease Support Group or us. 12