Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Political abuse of psychiatry wikipedia , lookup
Antipsychotic wikipedia , lookup
Separation anxiety disorder wikipedia , lookup
Schizoaffective disorder wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
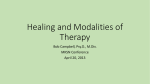
Classification of mental disorders wikipedia , lookup
Schizophrenia wikipedia , lookup
Sluggish schizophrenia wikipedia , lookup
Major depressive disorder wikipedia , lookup
Pyotr Gannushkin wikipedia , lookup
Conversion disorder wikipedia , lookup
Child psychopathology wikipedia , lookup
Glossary of psychiatry wikipedia , lookup
History of psychiatric institutions wikipedia , lookup
Moral treatment wikipedia , lookup
Generalized anxiety disorder wikipedia , lookup
Mental status examination wikipedia , lookup
Emergency psychiatry wikipedia , lookup
History of mental disorders wikipedia , lookup
History of psychiatry wikipedia , lookup
Abnormal psychology wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
Posttraumatic stress disorder wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
Cognitive Behavioral Therapy for Posttraumatic Stress Disorder in Persons With Psychotic Disorders Clinical Case Studies 8(6) 438–453 © The Author(s) 2009 Reprints and permission: http://www. sagepub.com/journalsPermissions.nav DOI: 10.1177/1534650109355188 http://ccs.sagepub.com Stephanie C. Marcello,1 Katie Hilton-Lerro,1 and Kim T. Mueser2 Abstract The prevalence of trauma in people with a serious mental illness (SMI) is high and poses a significant health problem. In addition, trauma exposure often leads to the development of posttraumatic stress disorder (PTSD). People with comorbid PTSD and a SMI have significantly poorer treatment outcomes. Despite the high occurrence of these two disorders, people with a SMI are often excluded from research on PTSD. To address this gap, Mueser, Rosenberg, and Rosenberg developed a cognitive restructuring (CR) program.This article describes a case study utilizing the CR program. The program is specifically tailored for people with psychotic and mood disorders with a focus on modifying dysfunctional beliefs and behaviors. Results suggest that addressing PTSD in people with a SMI is necessary and that the CR program can promote recovery in this population. Keywords trauma, posttraumatic stress disorder, serious mental illness, psychosis, schizophrenia, cognitive restructuring, cognitive behavioral therapy Cognitive behavioral therapy (CBT) has been shown to be effective for the treatment of posttraumatic stress disorder (PTSD) in the general population, with the preponderance of evidence supporting the efficacy of exposure therapy and cognitive restructuring (CR; Foa, Keane, Friedman, & Cohen, 2009). However, research on the treatment of PTSD in the general population has typically ruled out a large number of prospective study participants for a variety of reasons, including the presence of psychotic symptoms, cognitive impairment, substance abuse, and comorbid medical conditions (Spinazzola, Blaustein, & van der Kolk, 2005). The treatment of PTSD in persons with psychotic disorders and other severe mental illnesses poses special challenges. 1 University of Medicine and Dentistry of New Jersey Department Medical School, Hanover, NH 2 Corresponding Author: Stephanie C. Marcello, PhD, University of Medicine and Dentistry of New Jersey, University Behavioral HealthCare, Division of Schizophrenia Research, 151 Centennial Avenue, Piscataway, NJ 08854 Email: [email protected] Marcello et al. 439 To address this issue, Mueser, Rosenberg, Jankowski, Hamblen, and Descamps (2004) developed a time-limited program based on breathing retraining, psychoeducation, and CR for people with a serious mental illness (SMI) and PTSD (Mueser, Rosenberg, & Rosenberg, 2009). The program was developed as an “add on” to other services that the client may be receiving, such as case management, pharmacological treatment, and psychiatric rehabilitation. The program is designed to focus on the teaching of two cognitive-behavioral skills, breathing retraining (BRT) for the management of anxiety, and CR to target and modify trauma-related beliefs that underlie PTSD symptoms. These skills are taught in a flexible but structured manner appropriate to the individual client’s cognitive and emotional capacity, with homework assignments collaboratively developed with the client to ensure practice of the skills outside of sessions. One randomized controlled trial of 108 clients with SMI and PTSD found that this program was more effective than usual services at improving PTSD, depression, and other psychiatric symptoms, with treatment gains maintained at 6 months post-treatment (Mueser et al., 2008). In this article we provide an illustration of the treatment model in a client with co-occurring severe PTSD and schizoaffective disorder. Emphasis was placed on the use of functional assessments in case conceptualization, which suggested the client’s PTSD symptoms were severe and the traumatic experiences appeared to have contributed to his delusional thinking. We describe the client’s progress through the different parts of the program, and summarize improvements in PTSD and related symptoms. We also discuss the role of homework in teaching skills in the program. 1 Theoretical and Research Basis Psychological trauma refers to the experience of an uncontrollable event which is perceived to threaten a person’s sense of integrity or survival (Horowitz, 1986). In defining a traumatic event, the Diagnostic and Statistical Manual of Mental Disorders (4th ed.) (DSM-IV; American Psychiatric Association, 1994) adopts a narrower definition to include events involving direct threat of death, severe bodily harm, or psychological injury, which the person at the time finds intensely distressing or fearful. PTSD is defined in the DSM-IV by three types of symptoms, including re-experiencing of the trauma, overarousal, and avoidance of trauma-related stimuli, which persist or appear at least one month after exposure to the event (American Psychiatric Association, 1994). The prevalence of traumatic events in the lives of people with SMI is high and poses a significant public health problem. Read, Perry, Moskowitz, and Connolly (2001) reported that 69% of female and 60% of male psychiatric inpatients had histories of physical and sexual abuse. Estimates of lifetime exposure to traumatic events in people with schizophrenia range from 34% to 98% (Greenfield, Strakowski, Tohen, Batson, & Kolbrener, 1994; Mueser et al., 1998; Ross, Anderson, & Clark, 1994). In addition, reported rates of PTSD in people with schizophrenia range from 29% to 43% (Cascardi, Mueser, DeGiralomo, & Murrin, 1996; Mueser et al., 2001). Furthermore, it has been suggested that the frequency of trauma among people with schizophrenia may be underestimated, due to patients’ underreporting traumatic experiences and insufficient assessments of traumatic events at mental health facilities (Eilenberg, Fullilove, Goldman, & Mellman, 1996; Read & Fraser, 1998; Resnick, Bond, & Mueser, 2003). A substantial amount of research has documented the negative effects of trauma on people with schizophrenia. Trauma exposure has been linked to more severe symptoms (Mueser et al., 1998), increased rates of substance abuse (Read & Fraser, 1998), depression and more severe cognitive impairment (Schenkel, Spaulding, DiLillo, & Silverstein, 2005), and suicidality (Strauss et al., 2006). In addition, trauma exposure in people with schizophrenia is associated with increased use of mental health services, including an earlier age at first hospitalization, higher 440 Clinical Case Studies 8(6) rate of hospital readmissions, and greater use of seclusion and restraints during inpatient treatment (Goodman, Rosenberg, Mueser, & Drake, 1997; Mueser, Salyers et al., 2004; Resnick et al., 2003). Overview of the CR Program Research on the treatment of PTSD in the general population has demonstrated the effectiveness of exposure therapy and cognitive restructuring, with neither intervention consistently found to be more effective than the other, nor the combination more effective than either one alone (Benish, Imel, & Wampold, 2008; Bradley, Green, Russ, Dutra, & Westen, 2005). CR was chosen as the main active ingredient in the program for people with SMI developed by Mueser et al. (2009) for two main reasons. First, it was expected that CR would be less stressful and more acceptable to clients with SMI than prolonged exposure. Second, there is abundant experience using CR to treat other symptoms (e.g., psychotic symptoms, depression) in people with a SMI (e.g., Beck, Rector, Stolar, & Grant, 2008; Kingdon & Turkington, 2004). CR is based on the premise that depression, anxiety, and other negative feelings are mediated by individuals’ thoughts and beliefs about events, themselves, and the world (Beck, Rush, Shaw, & Emery, 1979; Ellis, 1962). Specific thoughts and beliefs related to traumatic experiences may or may not be accurate. To the extent that negative, self-defeating thoughts or beliefs are inaccurate, correcting them can reduce or eliminate the associated upsetting feelings. Individual differences in the personal meaning or appraisal of a traumatic event are a major factor in determining which individuals develop PTSD (Ehlers & Clark, 2000). Life experiences that introduce conflict into fundamental beliefs that an individual previously had about the world are more likely to be perceived as traumatic (Brewin & Holmes, 2003; Horowitz, 1979, 1986). PTSD is more likely to develop in people who have exaggerated, negative cognitive appraisals of traumatic events that emphasize the inherent danger in the world, mistrust of other people and the individual’s own response to trauma, such as being mentally defeated by an event (Dunmore, Clark, & Ehlers, 1999; Ehlers, Maercker, & Boos, 2000; Halligan, Michael, Clark, & Ehlers, 2003). When a person encounters stimuli that resemble events related to the trauma, these cues evoke trauma-related schemas that trigger distress due to perceptions of threat, loss, or personal inadequacy. CR involves teaching people how to identify, examine, challenge, and change inaccurate thoughts associated with negative feelings. Treatment programs using CR for posttraumatic disorders involve helping clients examine and modify these inaccurate trauma-related beliefs (Ehlers, Clark, Hackmann, McManus, & Fennell, 2005; Mueser et al., 2009; Resick & Schnicke, 1993). The CR program developed by Mueser et al. (2009) was designed to treat the broad population of persons with PTSD, while accommodating to the special needs of vulnerable populations such as persons with SMI, addiction, adolescents, or individuals exposed to natural disaster or mass violence. The program includes teaching BRT for the management of anxiety, education about PTSD and other trauma-related problems, and a primary focus on CR for addressing posttraumatic symptoms. CR is taught to clients as a skill for managing negative feelings and modifying posttraumatic appraisals that underlie PTSD symptoms, based on cognitive theories of PTSD described above. Since posttraumatic symptoms are defined partly in terms of their intrusive and upsetting effects on individuals’ daily lives, teaching CR as a way of coping with negative feelings naturally leads to addressing trauma-related thoughts and beliefs. Teaching CR as general self-management skill for dealing with any negative feelings, rather than using it solely to target cognitions believed to be related to traumatic experiences, simplifies the process of teaching the skill for therapists and clients alike, as it requires no distinction to be made between which thoughts or feelings are or are not related to the traumatic events. Marcello et al. 441 The CR Program The program is provided in 12-16 1-hour individual, weekly therapy sessions. To facilitate the teaching of skills in a systematic yet flexible manner, each session adheres to the following structure: (a) present a brief agenda for the current session; (b) briefly review the previous session; (c) review homework; (d) cover session’s material (most of the session time is spent on this item); (e) assign homework; (f) review session. During the first few sessions, establishing the therapeutic alliance is essential. The overall goal is to create an empathic and supportive environment where trauma work can be conducted in a safe, contained, yet task-focused manner. Session 1 begins with administering the PTSD Checklist Stressors Specific Version (PCL-S; Blanchard, Jones-Alexander, Buckley, & Forneris, 1996), with the client’s index trauma written at the top in order to assess severity of PTSD symptoms, and the Beck Depression Inventory-II (BDI; Beck, Steer, & Brown, 1996) to evaluate depression severity. Next, a brief orientation to the program and its components is provided, along with a discussion of homework and logistical aspects of treatment (e.g., cancellations). Then, a written crisis plan is developed to address any changes in the client’s psychiatric disorder or functioning that could signal a relapse or threaten the person’s continued participation in the program (e.g., increase or resumption of substance use, increased depression, suicidal thoughts, increased hallucinations, social isolation). In the last 15 minutes of the session, BRT is taught and practiced in session. A homework assignment is developed collaboratively with the client to regularly practice the BRT on his or her own, at first practicing it in safe and comfortable situations until the person has developed sufficient competence with the skill. In session 2, common reactions to trauma are discussed. The primary goal of psychoeducation is to help the client understand the nature of PTSD and establish it as a treatable disorder. The three main symptoms of PTSD that are discussed are: (a) re-experiencing the trauma; (b) active avoidance; (c) overarousal. In session 3, other common reactions to trauma are discussed, including: (a) four types of negative feelings: fear and anxiety, sadness and depression, guilt and shame, and anger; (b) relationship difficulties; (c) drug and alcohol abuse. Both psychoeducation sessions are taught using handouts that are read and discussed in an interactive manner in order to make the information as useful and pertinent to the client’s own experiences. Review questions are periodically asked to evaluate comprehension of the material, with additional reviews conducted as needed. Finally, at the end of session 3, treatment goals are set, based on the client’s discussion with the therapist of how PTSD has affected their lives, and the changes they would most like to see as a result of participating in the program. Session 4 starts with completing the PCL and BDI-II to assess the individual’s symptoms. It is not expected that most clients will experience an improvement in symptoms at this point, because CR has not been taught yet. However, some clients do report symptomatic improvement just from learning BRT and the psychoeducational sessions. If symptoms do improve, it is helpful to talk with the client about what they attribute these changes to. Occasionally, symptoms are slightly worse at the fourth session, and it is helpful for the therapist to normalize this experience, and to reframe it as part of the process of recovery from trauma. Following the review of symptoms, the remainder of session 4 is spent introducing cognitive restructuring, which is continued in session 5. The primary goal of these sessions is to first explain to the client the relationship between thoughts and feelings, and second to introduce a strategy for identifying and correcting common biases in thinking (frequently referred to as “cognitive distortions” in the CR literature, or Common Styles of Thinking (CST), in the program developed by Mueser et al., 2009). Clients are taught that CST are thinking patterns that people often have in reaction to everyday events, but which are inaccurate and unhelpful, and contribute to upsetting feelings. Some examples are: catastrophizing, all-or-nothing thinking, emotional 442 Clinical Case Studies 8(6) reasoning, “must” “should” or “never” statements, emotional reasoning, and inaccurate or excessive self-blame. In order to normalize this type of thinking, the therapist emphasizes to the client that everyone engages in these thinking patterns sometimes, but some people may be more prone to them than others because of their personal life experiences, including traumatic ones. Understanding which CST the client engages in can help them identify and correct thoughts and beliefs that lead to their upsetting feelings. After the client has gained some familiarity with recognizing and correcting CST, usually by session 5 or 6, the therapist introduces a more powerful approach to cognitive restructuring: the 5 Steps of CR. These steps include (a) describe the situation; (b) identify different feeling states (in particular, the “big four” feelings: fear and anxiety, sadness and depression, guilt and shame, and anger); (c) identify “automatic thoughts” associated with each feeling and focus on the most upsetting thought; (d) evaluate the thought and weigh the evidence for and against them; and (e) take action by either changing the thought or making a plan to remedy the problem situation. Homework assignments are developed with the client to practice using the 5 Steps of CR. Most of the remainder of the program is spent working through examples of CR that the client brings in from his/her life. After the initial introduction to the 5 Steps of CR, the following sessions are devoted to helping the client learn how to use the skill for dealing with negative feelings, and addressing trauma-related beliefs and schemas that underlie their PTSD symptoms. The sessions start with a homework review to evaluate the client’s efforts at using the 5 Steps of CR, focusing on helping clients learn steps for which they experienced difficulties. Then, the rest of the session is spent teaching the client how to use the 5 Steps of CR to address other negative feelings experienced during the week, specifically PTSD symptoms or depressive symptoms, or other trauma-related thoughts or beliefs that can be identified. After the client has been introduced to the 5 Steps of CR, the clinician shifts the focus of teaching to help the client learn and use the steps him/herself, rather than continuing to lead the client through the steps. This involves giving responsibility for completing the worksheet to the client in the session, asking questions to prompt the client to identify each step and its purpose (e.g., “OK, so what’s the first step of CR? Why is it important to describe the situation?” “Now that you’ve identified your upset feeling, what’s next?”), and providing hints or strategies to help the client use the skill more effectively. It is also important to reinforce the client for using the steps correctly, both by providing positive feedback and drawing attention to reductions in distress that usually occur when the 5 Steps of CR are completed. When working through the 5 Steps of CR, if the client concludes in the fifth step that the evidence supports his/her distressing thought, an Action Plan needs to be created to help the client deal with that upsetting situation. Learning how to face problems and how to develop effective Action Plans can counter the natural tendency of many trauma survivors to attempt to avoid such problems, and this new skill will ultimately give them greater control over their lives. Action Plans include the following four components: (1) a clear goal; (2) a list of possible strategies for achieving the goal; (3) a step-by-step plan for implementing the selected strategies; and (4) a date to follow up on the plan. From the outset of the CBT for PTSD program, the therapist aims at helping clients generalize the skills taught in session to their daily lives, and to maintain those skills after the program has ended. The more competence clients develop at CR over the course of treatment, the more likely it is that they will continue to be able to use the skill after the program ends. Central to teaching clients how to use CR is the therapist’s systematic use of shaping, or the successive reinforcement of approximations to a desired goal or skill. In order to shape the client’s competence at using cognitive restructuring, the therapist needs to actively engage him or her in repeatedly practicing the skill during treatment sessions, and provide feedback and guidance to hone the skill over multiple efforts. Homework practice between therapy sessions gives clients the opportunity Marcello et al. 443 to see whether they can use the CR skill taught in session on their own. Throughout treatment the therapist clearly communicates to the client that the CBT program is time-limited. Such clear communication is necessary to shape expectations, motivate participants to make use of the therapy sessions, and prepare them for termination. In the second to last session, there is a joint meeting between the PTSD therapist, client, and case manager/primary clinician. In this session, the client teaches their primary case manager the 5-steps of CR and they discuss how they will utilize this skill in their sessions. 2 Case Presentation “Mr. X” was in his 50’s when he was referred for treatment after scoring within the severe range for PTSD on the PCL. He was currently attending a partial hospital program 4 days per week for treatment of his schizoaffective disorder symptoms. Upon admission, he struggled with limited social skills, paranoid ideation, disorganization, and depressed mood. He lived in supported housing and was unemployed. He presented with depressed mood, anxiety, disorganization, episodes of irritability and agitation, difficulty in making decisions, ruminating thoughts, and paranoid ideation. Mr. X also had a long history of polysubstance abuse dating back into his 20’s, although he had been abstinent for many years. As part of his partial hospitalization treatment, Mr. X was assessed for PTSD and scored within the high range. He reported that his PTSD symptoms were negatively affecting his ability to function on a daily basis; he spent most of his time alone, did not have many close relationships, and had difficulty in taking care of himself. Mr. X presented with multiple PTSD symptoms. He expressed difficulties in trusting people and forming close relationships. He had severe anxiety and feared that something bad would happen to him, despite a lack of evidence. Mr. X presented with severe hyperarousal symptoms including, hypervigilance, and difficulties in falling asleep and concentrating. He engaged in many of the Common Styles of Thinking (CST) patterns, such as, all or nothing thinking, overgeneralization, emotional reasoning, and catastrophizing. Some of the themes in his distorted thinking included, “I’m no good at all,” “no one likes me,” and “I will always get hurt in a relationship.” 3 Presenting Complaints Mr. X’s primary presenting problems were anxiety and mood lability with a history of psychotic features. His secondary problems included inability to live independently, lack of social skills and social supports, and failure to obtain and hold employment. Mr. X experienced occasional panic attacks. He noted that his anxiety tended to be general in nature, but more recently centered on his interactions with other people. Mr. X stated that his paranoid thoughts made him more anxious during his social interactions. He reported that he often felt like what he had to say was “not important,” and would ruminate about his daily interactions, feeling like his contributions to groups and peers were “stupid.” This prevented him from being able to fall asleep, speaking up, trying to meet new people, or expressing his feelings to his family or friends. With Mr. X’s symptom report at onset of PTSD treatment, it appeared as though he was also suffering from social anxiety disorder. Mr. X also reported that his depression had increased to the point that he often couldn’t get out of bed in the morning. He stated, however, that since being in the partial hospital program and improving his coping skills his severe depressive episodes had occurred less frequently. He also attributed the improvements to adhering to his prescribed medication. Mr. X stated that feeling rejected or abandoned had often triggered depressive episodes. When in the midst of feeling 444 Clinical Case Studies 8(6) depressed he struggled with feelings of guilt, being self-critical, loss of confidence, feeling like he should be punished, loss of interest and energy, and indecisiveness. Mr. X had a history of suicidal ideation, but had not experienced these symptoms in 8 years. He reported increased instances of suicidal ideation when under the influence of mood altering substances. He stated that, when under the influence, the thoughts would start off as “it would be better for everyone if I wasn’t here” and then escalate to thinking of a plan. Mr. X had been receiving partial hospitalization services since 2001. He stated that he was frustrated with his current symptoms because he wanted to be able to find employment and possibly find a significant other to share his life with, but felt his current level of functioning prevented him from moving forward on either of these goals. 4 History Mr. X was born and raised in New Jersey to a middle-income family; he was the youngest of 3 children. He met developmental milestones and performed at a satisfactory level in school, although he reported difficulty in keeping up with his peers academically. Mr. X had a limited circle of friends when in school and was described as a shy child. When Mr. X was a child, he was sexually abused by a neighbor from ages 6 through 13. Mr. X said that he was afraid that no one would believe him if he told and his abuser reinforced those fears. He did not report this to his parents until he was much older and the neighbor had moved away. Mr. X reported experiencing problems with anxiety since his childhood and depressive episodes since his teens. He had a history of psychiatric symptoms since his early 20’s, which were aggravated by his heavy polysubstance dependence. He reported that the anxiety and depression had varied in their severity throughout his treatment and that he had experienced periods where it was difficult for him to have healthy activities of daily living or to leave the house. Mr. X abused multiple mood altering substances. This started in high school and escalated throughout his 20’s and 30’s. Abused substances included alcohol, marijuana, cocaine, and heroin. During periods of active addiction, Mr. X would prostitute himself with men in order to obtain drugs. These encounters would bring up memories of his childhood sexual abuse and as a result, he would use increased amounts of drugs to medicate the pain. For weeks after prostituting behaviors, when he was not using mood altering substances, he would have flashbacks and experience symptoms of hyper-arousal: increased heart rate, sweating, trembling, and agitation. Since his 20’s, Mr. X had been involved in various levels of care and had 4 psychiatric hospitalizations. Each time Mr. X was hospitalized, it was for an increase in his depression and psychotic symptoms. Mr. X had found the partial hospitalization treatment to be the most effective program for him. As a client in the partial hospitalization program, he had been receiving group therapy and pharmacological treatment and had been able to maintain stability in the community without the need for inpatient treatment. Although Mr. X had received individual therapy before, he stated that it did not focus on his traumatic experiences. When he was approached by his individual therapist about trauma he had difficulty “putting his feelings about the events into words.” As a result, he would wind up discussing other matters instead. Mr. X brought several strengths to his PTSD treatment. He was motivated and willing to attend 16 weeks of treatment, and was open to learning about PTSD. Although he was initially unaware of how his thoughts, emotions, and feelings were connected to one another, he was motivated to learn about this, and was able to improve his insight in this regard despite his cognitive limitations. Mr. X had difficulty in understanding his thoughts and his metacognitive deficit was worked on throughout treatment (Lysaker, Buck & Ringer, 2007). Marcello et al. 445 5 Assessment To better assist in diagnosis, conceptualization, treatment planning, and monitoring outcome, Mr. X completed several assessments at intake, during the course of treatment, and at the end of treatment. As part of an ongoing assessment, two measures were administered every third session over the course of the 16-week CR program: Beck’s Depression Inventory-II (BDI-II) and PTSD Checklist Stressor Specific Version (PCL-S). Careful assessment of the client’s understanding and response to treatment is important throughout the program. This monitoring is done both formally and informally with the client and his/her treatment team (e.g., case manager). Integration of the PTSD program with current treatment is also important. During treatment, there was regular consultation with the case manager/primary therapist to review client progress, particularly outside of therapy (e.g., have there been times when the skills learned in the program have helped and have there been crises that might be related to the PTSD treatment?). Mr. X also had cognitive deficits, including difficulties following through on tasks due to impaired memory and attention, poor problem solving skills. Due to his cognitive impairments, several strategies were implemented to more effectively teach the critical information and skills. For example, material was presented at a slower pace and the therapist periodically checked in with him throughout each session to verify and correct his understanding of the material. Paper-and-Pencil Measures PTSD checklist stressor specific version (PCL-S; Weather et al., 1993). The PCL-S has been found to be both a reliable and valid instrument as a brief self-report inventory of PTSD (Blanchard, et al., 1996), including in clients with SMI (Mueser et al., 2001). The PCL-S is a 17-item selfreport measure based on the criteria for a DSMI-IV diagnosis of PTSD. Items are rated on a 5-point Likert-type scale ranging from 1 (not at all) to 5 (extremely). There are several versions of the PCL. The PCL-S (which was used with Mr. X) asks about specific problems in relation to an identified “stressful experience.” Scores range from 0 to 85 and interpretation is based on total score. Scores above 45 are indicative of severe PTSD, what is needed to participate in this treatment. Prior to administering the PCL-S, an “index trauma” or the trauma that is currently causing the most distress in the person’s life is identified in session. Because people with co-occurring schizophrenia and PTSD to have numerous traumas in their lives, by identifying the event causing the most distress, we can monitor the symptoms more accurately. Beck Depression Inventory-II (BDI-II; Becket al., 1996).The BDI-II is the most widely used instrument to assess severity of depressive symptoms (Lambert & Stephenson, 2000). The BDI-II is a 21-item Likert-type scale with individual scores ranging from 0 to 3, with higher scores representing increased symptomatology. Each item represents a symptom that is a DSM-IV characteristic of depression, such as loss of pleasure, suicidal thoughts, sadness and feelings of worthlessness. Scores range from 0 to 63 and interpretation is based on total score. Scores from 0 to 13 indicate minimal depressive symptomatology, from 14 to 19 indicate mild depressive symptoms, and from 29 to 63 indicate severe depressive symptomatology. 6 Case Conceptualization Through a review of biopsychosocial factors, it was hypothesized that Mr. X’s PTSD and psychotic symptoms may have been caused, maintained and/or exacerbated by the traumatic events in his childhood. One explanation for this is that earlier life experiences that introduce conflict into one’s belief system can make a person more vulnerable to developing PTSD and other 446 Clinical Case Studies 8(6) mental illnesses. In addition, his maladaptive thinking patterns appeared to play a role in both types of symptoms. The psychotic symptoms Mr. X struggled with in the past included paranoid ideation about family and supports in his life, inappropriate affect, disorganized and tangential thoughts, and a history of auditory hallucinations, the content of which was negatively centered around his selfworth, safety around others, and commands to harm himself. Upon initiation of PTSD treatment, Mr. X’s psychotic symptoms included paranoid ideation toward family and peers, mild auditory hallucinations, and tangential thinking. He verbalized multiple core beliefs that reflected distorted thinking such as, “I’m stupid, I’m worthless, no one will every love me.” Several treatment goals were developed that included increasing daily social interaction because of his tendency to isolate when he experienced symptoms, developing better coping skills for symptoms, identifying continued triggers for substance abuse, working on his relapse and recovery thoughts, and expanding his social connections outside of the partial hospital program. 7 Course of Treatment and Assessment of Progress Session 1 In session 1, Mr. X established a good rapport with his PTSD therapist. The client completed a crisis plan to assist him throughout treatment. He understood that he could refer to the crisis plan at any time, in or out of session. Mr. X defined crises that would be difficult to handle as increased anxiety, depression or psychosis, and the urge to use drugs or alcohol. Maintaining Mr. X’s sobriety was very important to him, so the urge to use was quite distressing. He was aware of his early warning symptoms of a possible crises, which included becoming argumentative with supportive others, withdrawing from others, increased anxiety or depression, and strong urges to use substances. He was able to clearly identify individuals he could go to for help if these signs occurred, including people both at the program and in the community. Mr. X’s crisis plan consisted of reaching out to his support system, taking his medications, and alerting members of his treatment team as soon as he noticed an early warning sign. After completing his crisis plan, Mr. X was taught the BRT skill. Mr. X learned this skill fairly quickly, as he had had exposure to breathing exercises in other forms of treatment. Mr. X reported that the BRT made him feel calmer and more relaxed. He expressed a willingness to practice and use the skill throughout treatment program. Sessions 2 and 3 As planned, Mr. X did very well in following through on his homework to practice BRT on his own, and soon he was able to begin using the skill when he started to feel stressed at home. During psychoeducation about PTSD, Mr. X completed the in-session handouts and discussed his symptoms. He reported that he had nightmares about the trauma several times a month that disrupted his sleep. Mr. X reported that, after he had a nightmare, he would be afraid to fall asleep for several days. He also reported avoidance symptoms. Mr. X stated that he often would avoid crowded places or situations where he would be around groups of men, because being in the presence of men triggered memories of his sexual abuse. He also experienced many of the overarousal symptoms. Mr. X stated that these symptoms were one of the most disruptive to his daily functioning. Over-arousal symptoms included heart pounding and chest pain, sweating, shaking, trouble falling asleep, restlessness, nausea, jumpiness, irritability, and being always on guard. Mr. X also discussed difficulty with feelings of fear and anxiety, sadness and depression, Marcello et al. 447 guilt and shame, and anger. Another problem that Mr. X found to be particularly troublesome was relationship difficulties. Mr. X stated it was often difficult for him to feel close to another person or trust other people. He stated that in his existing relationships, he was often afraid that the people he loved would leave him. Mr. X identified that he struggled with conflict with family members and establishing and maintaining relationships. In addition to the previous goals Mr. X established when he first entered the partial program (discussed above), he also set goals in the CR Program. The goals Mr. X identified where to build healthier, close relationships, to find a significant other to share his life with, and to be able to return to work. Mr. X felt that if he could learn to mange his PTSD symptoms these goals would be possible for him. Sessions 4 to 5 The teaching of CST proceeded slowly due to Mr. X’s cognitive deficits and the therapist’s need to teach slowly, allow Mr. X to ask questions, and to review the concept of the common styles of thinking several times. With practice, Mr. X began to learn how to recognize common styles in inaccurate thinking, and how to challenge and correct those thoughts. Sessions 6 to 12 Mr. X responded well to the 5-steps of CR. The therapist often stopped to check for comprehension before moving forward as sometimes Mr. X would say he understood, but it would become clear he needed further clarification. Mr. X struggled most with Step 4—evaluating the evidence for and against the thought. Every session would require a review of the type of evidence that he needed to look for to accurately complete the five steps. The therapist encouraged him to look for evidence like a police detective investigating a case. This strategy was helpful to him in sessions, and he learned to prompt himself to pretend that he was a detective when using the skill on his own. The therapist needed to utilize much repetition to reinforce these learning points session after session. Socratic questioning was also used to guide the client in using Step 4. When Mr. X veered way from relying on factual information as evidence in Step 4, he responded well to his therapist asking him whether he was focusing only on the facts. He also struggled with what it meant if a thought could be identified as a Common Style of Thinking. He was often able to identify that his thoughts were Common Styles of Thinking, but would need to be reminded that CST were inaccurate, and not supported by the evidence. Sessions 6 through 12 were spent practicing and honing the 5 Steps of CR. Despite Mr. X’s initial difficulty with the different steps, he only needed to develop an Action Plan twice to deal with problematic situations throughout treatment. Even when practicing the 5 Steps of CR on his own, Mr. X was frequently able to correct inaccurate thoughts and beliefs, and get relief from his distressing feelings. When initially teaching the 5 Steps of CR, the therapist encouraged Mr. X to focus on upsetting everyday events, rather than ones clearly related to his sexual abuse. Around session eight, as Mr. X became more skilled at using the 5 Steps of CR, the therapist began to utilize the worksheets about PTSD that Mr. X had completed, and distressing symptoms endorsed on the BDI-II and PCL, to guide him toward more trauma-related thoughts. Mr. X identified trauma-related thoughts such as “I’m a bad person” or “No one could ever love me.” Mr. X believed that he was a weak, stupid person because he had allowed himself to be abused. He was able to challenge this belief by working through the 5 steps in session, and after completing CR, Mr. X was able to change the thought to “even though I felt stupid at the time, 448 Clinical Case Studies 8(6) I was a child when I was abused and it was not my fault.” Mr. X was able to look at the evidence in Step 4 of CR and realize that as a child, the abuse was beyond his control and not his fault. Another core belief that Mr. X reported was “no one will ever love me because I was abused.” This belief was also challenged through the use of the 5 steps of CR. In step 4, Mr. X was able to generate evidence against the thought (my family tells me they love me every time I speak to them on the phone, my best friend wants to spend time with me and be around me; we hang out 2 times a week) and was able to come up with a new thought (“I have people in my life who love me despite the fact that I was abused as a child”). After each session, Mr. X was assigned homework to use the 5 steps of CR daily. Sessions 12 to 16 In sessions 10 to 12, the process of termination was discussed with Mr. X. The therapist explained to him the importance of his case manager joining them in a session toward the end of the program to learn about his participation, and about the 5 Steps of CR. Mr. X understood that the purpose of this exercise was so he would continue to use the new skills even after the PTSD treatment program had ended. Mr. X’s case manager joined the client and therapist in the final session 16. In the final session, the PCL and BDI-II were completed and discussed as Mr. X had shown decreases in both measures from the time of the initial session. Mr. X commented that he did feel a difference since the beginning of treatment and noticed that he was having fewer PTSD-related symptoms. His case manager joined the session for about 20 minutes, and Mr. X did a nice job of demonstrating the 5 Steps of CR for his case manager, with some assistance from the therapist. The case manager asked several questions related to how well the treatment works and Mr. X responded positively about how it had helped him change his thought patterns and reactivity. His treatment team, including the PTSD therapist, noted positive changes in the client in regards to his self-esteem and group participation. Mr. X’s clinician reported that their therapeutic relationship continued to positively develop and treatment was smooth throughout the entire 16 sessions. The remainder of the session was spent reviewing what areas of his life Mr. X felt were improved by the treatment and what skills he found to be the most helpful. He found that over the last few weeks of treatment, his thinking was more positive overall and he found he needed to use the skill less and less. Mr. X also found that he had more patience with himself as well as others. His overall anxiety level decreased as well. Mr. X agreed that these were skills that he fully intended on using in the future as part of his treatment and in the community when he noticed himself starting to get upset. Overall, Mr. X reported feeling very positively about his PTSD therapy and responded well to the termination process. Assessment of Progress Mr. X learned that some of his symptoms, and much of his distress, was due to PTSD. Before participating in the program, Mr. X had believed that all of his symptoms were related to his schizoaffective disorder. When Mr. X first learned the 5 Steps of CR, and throughout sessions six through eleven, it would take the entire session to review his homework and work through a single worksheet. From session 12 and on, Mr. X was able to complete multiple sheets in session as he was able to move through the five steps quicker and get the same amount of relief, if not more. Mr. X reported that, after learning the 5 Steps of CR, he was able to look at his thoughts with different perspective. He stated that instead of getting angry or upset immediately, he had improved control over his reactions and was able to come up with more realistic and helpful thoughts. Mr. X experienced a decrease in depression and anxiety, irritability, and paranoid 449 Marcello et al. 30 27 BDI-II score 25 22 21 20 15 BDI-II 14 10 12 10 5 0 1 4 7 10 Session # 13 16 Figure 1. BDI-II 60 57 51 PCL-S score 50 43 50 40 36 30 30 PCL-S 20 10 0 1 4 7 10 Session # 13 16 Figure 2. PCL-S ideation. He found that by the end of treatment he was even using the 5 Steps of CR less often and his negative thoughts were occurring less frequently. Mr. X reported feeling an increase in positive thoughts and emotions and his treatment team noticed his improved mood and functioning level. Upon termination, Mr. X said he felt be able to work on getting a job and believed that he was capable of developing and maintaining healthy, trusting relationships. See Figures 1 and 2 for Mr. X’s BDI-II and PCL-S scores. 8 Complicating Factors One complicating factor was Mr. X’s cognitive difficulties. Several techniques worked well to help him understand the material: (1) explaining and demonstrating the five Steps of CR (with the therapist taking the lead); (2) prompting the client to use the steps of the skill (with the client taking the lead); (3) praising the client for steps that were performed well; (4) providing additional 450 Clinical Case Studies 8(6) prompts or instructions to teach other steps; (5) gradually fading the instructions and prompts as the client became more able to perform the skill independently. 9 Managed Care Considerations There were no managed care considerations necessary, as Mr. X had social security benefits. 10 Follow-Up No formal follow-up was scheduled with Mr. X; however, considerable emphasis was placed on continuing to use the breathing exercises and CR once the sessions ended. In the last session, Mr. X’s case manager was present and they created a plan to continue to work on the 5 Steps of CR. Mr. X continued to attend the partial hospital program and is working toward discharge. Some of the goals Mr. X had set in the early stages of PTSD treatment were to be able to increase his peer support group, move to more independent living, and to return to work. At posttreatment, Mr. X was applying for more independent living, he had attended more recreation events through his day program with peers he did not socialize with before, and was applying to a supportive employment program. Mr. X is currently attending a vocational readiness group at his day program. 11 Treatment Implications of the Case This case provides an example of an effective implementation of a recently developed and empirically supported program for treating PTSD in persons with SMI (Mueser et al., 2008, 2009). It also demonstrates the utility of offering a cognitive-behavioral treatment for severe PTSD in people with a SMI. 12 Recommendations to Clinicians and Students This case underscores the importance of assessing trauma and PTSD in people with SMI, who tend to have experienced multiple traumas throughout their lives but are rarely evaluated for the presence of PTSD, and of treating PTSD in this population that has been excluded from most treatment research. In addition, the effect of homework and the clinician’s attitude and use of shaping techniques to reinforce completing these assignments appeared to have contributed to the effectiveness of the treatment. It is imperative that clinicians provide rationale for homework at the onset of treatment, develop homework assignments in a collaborative fashion with input from the client, regularly follow-up on homework completion, and troubleshoot difficulties as needed. Author’s Note This paper is for the “Special Issue on Psychotherapies for Schizophrenia (S. Silverstein and P. Lysaker, Guest Editors).” Declaration of Conflicting Interests The authors declared that they had no conflicts of interests with respect to their authorship or the publication of this article. Funding This research was supported by NIH grant #: R01 MH064662-04A1. Marcello et al. 451 References American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author. Beck, A. T., Rector, N. A., Stolar, N., & Grant, P. (2008). Schizophrenia: Cognitive theory, research, and therapy. New York: Guilford. Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1979). Cognitive therapy of depression. New York: Guilford. Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Manual for the Beck Depression Inventory-II. San Antonio, TX: Psychological Corporation. Benish, S. G., Imel, Z. E., & Wampold, B. E. (2008). The relative efficacy of bona fide psychotherapies for treating post-traumatic stress disorder: A meta-analysis of direct comparisons. Clinical Psychology Review, 28, 1281-1289. Blanchard, E. B., Jones-Alexander, J., Buckley, T. C., & Forneris, C. A. (1996). Psychometric properties of the PTSD Checklist (PCL). Behavior Research Therapy, 34, 669-673. Bradley, R., Green, J., Russ, E., Dutra, L., & Westen, D. (2005). Multidimensional meta-analysis of psychotherapy for PTSD. American Journal of Psychiatry, 162, 214-227. Brewin, C. R., & Holmes, E. A. (2003). Psychological theories of posttraumatic stress disorder. Clinical Psychology Review, 23, 339-376. Cascardi, M., Mueser, K. T., DeGiralomo, J., & Murrin, M. (1996). Physical aggression against psychiatric inpatients by family member and partners. Psychiatric Services, 47, 531-533. Dunmore, E., Clark, D. M., & Ehlers, A. (1999). Cognitive factors involved in the onset and maintenance of posttraumatic stress disorder (PTSD) after physical and sexual assault. Behaviour Research and Therapy, 37, 809-829. Ehlers, A., & Clark, D. M. (2000). A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy, 38, 319-345. Ehlers, A., Clark, D. M., Hackmann, A., McManus, F., & Fennell, M. (2005). Cognitive therapy for posttraumatic stress disorder: Development and evaluation. Behaviour Research and Therapy, 43, 413-431. Ehlers, A., Maercker, A., & Boos, A. (2000). Posttraumatic stress disorder following political imprisonment: The role of mental defeat, alienation, and perceived permanent change. Journal of Abnormal Psychology, 109, 45-55. Eilenberg, J., Fullilove, M. T., Goldman, R. G., & Mellman, L. (1996). Quality and use of trauma histories obtained from psychiatric outpatients through mandated inquiry. Psychiatric Services, 47, 165-169. Ellis, A. (1962). Reason and emotion in psychotherapy. New York: Lyle Stuart. Foa, E. B., Keane, T. M., Friedman, M. J., & Cohen, J. A. (Eds.). (2009). Effective treatments for PTSD: Practice guidelines from the international society for traumatic stress studies (2nd ed.). New York: Guilford. Goodman, L. A., Rosenberg, S. D., Mueser, K. T., & Drake, R. E. (1997). Physical and sexual assault history in women with serious mental illness: Prevalence, correlated, treatment, and future research directions. Schizophrenia Bulletin, 23, 685-696. Greenfield, S. F., Strakowski, S. M., Tohen, M., Batson, S. C., & Kolbrener, M. L. (1994). Childhood abuse in first-episode schizophrenia. British Journal of Psychiatry, 164, 831-840. Halligan, S. L., Michael, T., Clark, D. M., & Ehlers, A. (2003). Posttraumatic stress disorder following assault: The role of cognitive processing, traumatic memory, and appraisals. Journal of Consulting and Clinical Psychology, 71, 419-431. Horowitz, M. (1979). Psychological response to serious life events. In V. Hamilton & D. M. Warburton (Eds.), Human stress and cognition: An information processing approach (pp. 235-263). New York: John Wiley. 452 Clinical Case Studies 8(6) Horowitz, M. (1986). Stress response syndromes (2nd ed.). New York: Jason Aronson. Kingdon, D. G., & Turkington, D. (2004). Cognitive therapy of schizophrenia. New York: Guilford. Lambert, M. J., & Stephenson, A. (2000). Beck Depression Inventory. In A. E. Kazdin (Ed.), The use of psychological testing for treatment planning and outcome assessments (pp. 831-836). Mahwah, NJ: Lawrence Erlbaum. Lysaker, P. H., Buck, K. D., & Ringer, J. (2007). The recovery of metacognitive capacity in schizophrenia across thirty two months of individual psychotherapy: A case study. Psychotherapy Research, 17, 713-720. Mueser, K. T., Goodman, L. B., Trumbetta, S. L., Rosenberg, S. D., Osher, F. C., & Vudaver, R., et al. (1998). Trauma and posttraumatic stress disorder in severe mental illness. Journal of Consulting and Clinical Psychology, 66, 493-499. Mueser, K. T., Rosenberg, S. D., Fox, L., Salyers, M. P., Ford, J. D., & Carty, P. (2001). Psychometric evaluation of trauma and posttraumatic stress disorder assessments in person’s with severe mental illness. Psychological Assessment, 13, 110-117. Mueser, K. T., Rosenberg, S. D., Jankowski, K., Hamblen, J., & Descamps, M. (2004). A cognitive-behavioral treatment program for posttraumatic stress disorder in severe mental illness. American Journal of Psychiatric Rehabilitation, 7, 107-146. Mueser, K. T., Rosenberg, S. D., & Rosenberg, H. J. (2009). Treatment of posttraumatic stress disorder in special populations: A cognitive restructuring program. Washington, DC: American Psychological Association. Mueser, K. T., Rosenberg, S. D., Xie, H., Jankowski, M. K., Bolton, E. E., Lu, W., et al. (2008). A randomized controlled trial of cognitive-behavioral treatment for posttraumatic stress disorder in severe mental illness. Journal of Consultant and Clinical Psychology, 76, 259-271. Mueser, K. T., Salyers, M. P., Rosenberg, S. D., Goodman, L. A., Essock, S. M., Osher, F. C., et al. (2004). Interpersonal trauma and posttraumatic stress disorder in patients with severe mental illness: Demographic, clinical, and health correlates. Schizophrenia Bulletin, 30, 45-57. Read, J., & Fraser, A. (1998). Staff response to abuse histories of psychiatric inpatients. Australian and New Zealand Journal of Psychiatry, 32, 206-213. Read, J., Perry, B. D., Moskowitz, A., & Connolly, J. (2001). The contribution of early traumatic events to schizophrenia in some patients: A traumagenic neurodevelopmental model. Psychiatry, 64, 319-45. Resick, P. A., & Schnicke, M. K. (1993). Cognitive processing therapy for rape victims: A treatment manual. Newbury Park, CA: Sage. Resnick, S. G., Bond, G. R., & Mueser, K. T. (2003). Trauma and posttraumatic stress disorder in people with schizophrenia. Journal of Abnormal Psychology, 112, 415-423. Ross, C. A., Anderson, G., & Clark, P. (1994). Childhood abuse and the positive symptoms of schizophrenia. Hospital and Community Psychiatry, 45, 489-491. Schenkel, L. S., Spaulding, W. D., DiLillo, D., & Silverstein, S. M., (2005). Histories of maltreatment in schizophrenia: Relationships with premorbid functioning, symptomatology, and cognitive deficits. Schizophrenia Research, 76, 273-286. Spinazzola, J., Blaustein, M., & van der Kolk, B. A. (2005). Posttraumatic stress disorder treatment outcome research: The study of unrepresentative samples. Journal of Trauma and Stress, 18, 425-436. Strauss, J. L., Calhoun, P. S., Marx, C. E., Stechuchak, K. M., Oddone, E. Z., Swartz, M., et al. (2006). Comorbid posttraumatic stress disorder is associated with suicidality in male veterans with schizophrenia or schizoaffective disorder. Schizophrenia Research, 84, 165-169. Bios Stephanie C. Marcello, PhD earned her doctorate in Counseling Psychology from Temple University. She is a Research Associate at UMDNJ-UBHC in the Division of Schizophrenia Research. Dr. Marcello focuses on people with serious mental illness, especially involving substance abuse and trauma. Marcello et al. 453 Katie Hilton-Lerro is a licensed professional counselor. She is a clinician at UMDNJ-University Behavioral Health Care and works directly with people who have serious and persistent mental illness. Kim T. Mueser, PhD is a licensed clinical psychologist and a Professor in the Departments of Psychiatry and Community and Family Medicine at the Dartmouth Medical School in Hanover, New Hampshire. Dr. Mueser has extensive clinical and research experience in the psychosocial treatment of schizophrenia and other severe psychiatric disorders. He has co-authored ten books and several hundred journal articles.