Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
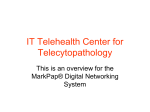
HOME TELEHEATH COMPLIANCE: LITERATURE REVIEW FINAL REPORT FOR ONE IN FOUR LIVES / AUSTRALIAN INFORMATION INDUSTRY ASSOCIATION TELEHEALTH RESEARCH AND INNOVATION LABORATORY SCHOOL OF COMPUTING, ENGINEERING AND MATHEMATICS UNIVERSITY OF WESTERN SYDNEY MAY 2015 ANTHONY MAEDER AND NATHAN POULTNEY Home Telehealth Compliance: Literature Review ABSTRACT systems suitable for delivery of Home Telehealth services. A major attraction of such solutions is that they enable new models of care to be implemented, shifting towards greater patient-centric and careteam-based emphasis in healthcare. This report describes a detailed review of published scientific literature on the topic of Home Telehealth compliance, encompassing aspects of patient adoption and adherence. A total of 72 peer review published papers were selected as the most relevant representatives of state-of-the-art contributions to the topic, and compliance findings presented in these papers are summarised here. Some common characteristics for studies selected were identified: they were mainly under 12 months in duration, with widely varying sample sizes, and typically 60-70% of participants were over 50 years of age and male. In general, there was good adherence/compliance at the start of a study that steadily dropped off over time, most rapidly in the period immediately after the start. Some overall observations of common themes across the range of papers are provided in conclusion. Numerous clinical trials have demonstrated the health, economic, and social benefits of Home Telehealth when used in specific clinical settings. However, developers and suppliers of both technology and services often face questions as to the effectiveness of these solutions, since their patient-centric nature also implies that the subjects-of-care have the option of “opting out” and abandoning use of the solution. They may also fail to make use of it in the intended way, resulting in poorer outcomes than were projected. The realisation of benefits can only occur in Home Telehealth settings when compliance levels are high, and so it is important to establish what evidence exists to inform this aspect of the overall Home Telehealth “business model”. This report describes a systematicallyconducted detailed review of published scientific literature on the topic of Home Telehealth compliance, encompassing aspects of patient adoption and adherence. A literature search strategy and filtering process was undertaken to establish the most relevant peer review published papers, which serve as representatives of state-of-the-art contributions to the topic. A total of 72 papers were selected for further in-depth analysis, and were classified as High, Moderate and Lower relevance in the level of their contributions. 1. INTRODUCTION Recently there has been rapid growth of the Home Telehealth market, providing patient monitoring and telecare services for individuals who are living independently in their own home accommodation. Much of this growth has been stimulated by the adoption of Home Telehealth solutions by large corporate healthcare organizations (as in the USA) or by government health agencies (as in the UK and some European countries). A further driver has been the development of new technology components and integrated 1 The findings presented in these papers concerning compliance to the use of Home Telehealth systems are summarised here. Some overall observations of common themes and critique of recurring issues revealed in the literature, across the range of papers, are provided in conclusion. It is hoped that this report will contribute to a broader understanding of the nature of Home Telehealth compliance, and inform future work to deploy the associated systems. year envelope to include the earliest home monitoring publications. The final overall search formula constructed was as follows: (adherence OR compliance OR retention OR attitudes) AND (self-care OR self-management OR selftreatment OR self-monitoring) AND (home-monitoring OR home-system OR telehealth OR tele-medicine OR tele-care) 2. METHODOLOGY The chosen terms included in this formula were those deemed to be most strongly indicative and most consistently used in connection with the concepts being sought. PubMed, Google Scholar and Scopus were selected as the most appropriate sources for searching the published literature, these having distinctive target collections which differ considerably from each other. PubMed is a specialised health publications collection, with a strict quality assurance process for inclusion. Google Scholar is a general automatically compiled listing with strong search capabilities. Scopus is an academically oriented collection with wide coverage of both health and non-health disciplines. It is acknowledged that compliance experiences may also be reported in grey literature, but that was beyond the scope of this review. Selection of papers was undertaken using the final overall search formula and results were as follows: - The results were ordered on the basis of best fit as determined by each source’s search function, generally requiring at least 1 term from each of the 3 groups of terms to be present. Figure 1 shows the overall process. Those papers with non-trivial citation counts (e.g. >10 cites for papers published up to 2010, and >1 cites for papers published since 2010) occurring in the first 10 pages (i.e. the highest rated best fits for the search results) of all three searches were extracted. Papers which duplicated project reporting were omitted. This process yielded a candidate list of 190 unique potential papers. These were scrutinised using their titles alone to indicate whether they were likely to be in scope for the review. This screening stage reduced the number retained to 121 probable papers. Search terms were selected to cover the topic area broadly, in three concept groups: - PubMed 1111 papers; Google Scholar 6480 papers; Scopus 9089 papers. Adherence to Usage; Self Care/Management; Telehealth Systems. A succession of trial search formulas were developed and applied, and refinement of the terms included in these was undertaken on the basis of iterative inspection of their results. Searches were limited to papers published from 1990 onwards, providing a 25 2 Of the 121 probable papers, 72 most relevant papers were identified on the basis of the combination of additional information in the keywords and abstract indicating good alignment with the target area of the review, and the remainder were rejected from further consideration. The 72 most relevant papers were then classified into High relevance (40 papers), Moderate relevance (18 papers) and Lower relevance (14 papers) categories, on the basis of reading their full text to establish their direct and comprehensive contributions. Table 1. Clinical areas covered by papers Clinical Area Blood Pressure Monitoring Heart Failure/Stroke Monitoring Diabetes Asthma Chronic Obstructive Pulmonary Disease (COPD) Activity Monitoring of Daily Living (AMDL) Lung Function /Respiratory Disease Well-being Cystic Fibrosis The 72 most relevant papers are listed in a table in the Appendix to this report, and full citations are provided in the References section. The year of publication of each paper is indicated. It may be noted that only 3 of these papers were published prior to 2000, and a further 12 prior to 2005, so there is a strong bias towards recent work published in the last 10 years. Papers concerning work undertaken in Australia have been identified. Prominence *** There was also a diverse range of study methodologies applied by the authors among the papers identified for inclusion, which are listed in Table 2. These are tabulated here (having been extracted from the Appendix table) to indicate the nature of the different scientific approaches taken, rather than to identify any methodologies as superior. 3. COMMENTARY The literature review conducted here considered High relevance papers reporting project findings, identifying factors which favour achievement of compliance and adherence, as well as reasons for noncompliance and non-adherence, in the area of home-monitoring and self-management health related devices. Table 2. Study methodologies used in papers Type of Study Methodology Randomised Controlled Trial (RCT) Systematic Review Feasibility Study Pilot Study Prospective Study Outcome Pilot Cross-sectional Survey Case Study Randomised Survey Literature Review Field Trial Qualitative Study/Evaluation Mixed Methods Study Longitudinal Study Studies and interventions in several different clinical areas were found, with information regarding patient adherence and compliance. These clinical areas are listed in Table 1 and assigned to three levels of prominence, based on number of papers and value of their content to informing this report. 3 The following sections consider each of the above clinical areas in turn and provide a brief discussion of the nature of the work reported and its contributions to knowledge on compliance performance matters. the GP practice monthly to have their blood pressure checked. The resulting satisfaction with the system after the 13 week programme was 4.81/5.00. It was also found that the system improved patient education about hypertension and they felt a greater degree of support and flexibility that "suited the patient rather than the practice".17 3.1 Blood Pressure Monitoring A study involving frequent home blood pressure monitoring of 17 articles revealed trends of compliance dropping during weekends compared to workdays. There was a greater degree of patient "enthusiasm" (ie; participation) in the first two months (89%) which then was followed by a phase lowering to 64%. At the conclusion of the study it was found that approximately half of the participants would willingly continue to monitor their blood pressure beyond the one year study.7 In a study on blood pressure monitoring among middle-aged Korean Americans a total of 377 patients participated in the study. Instructions were to take blood pressure readings 3 times upon waking and 3 times again before bed, at least 2 or more times a week over a 48 week period. Through the use of multivariate logistic regression it was found that older participants were more compliant than younger participants, also patients with depressive symptoms were also less compliant. It was found that participants that were compliant with the instructions were 4 times more likely to control their blood pressure by the end of the intervention in comparison to those who were noncompliant. The results suggest that participants who checked their blood pressure regularly had a much greater tendency to control their blood pressure.19 In a community-based senior centre pilot study of blood pressure monitoring, the use of a kiosk for taking readings steadily increased over the trial period and was as high as 80% in a study size of 112 participants. The usage then begun to decline to only 47% by 10 months. The vast majority of intervention patients reported being "very comfortable" with the technology by the end of the study and reported that it was "very easy" to use. 89% of study participants reported they would recommend it to a friend.16 A telephone survey was conducted with a random quota sample of a group of nonparticipants in a home blood pressure monitoring study. The questions were designed to assess the use of monitors, patients' perceived benefit, patient communication with providers and any barriers. 320 surveys were completed which was a response rate of 53%. Barriers to participation were primarily personal such as forgetfulness, not having time to take readings as well as self-described laziness. The A study involving blood pressure readings texted to a server by 124 participants was found to be well accepted by patients reporting high satisfaction due to the system being easy to use and receiving valuable feedback from their GP in regards to their readings. This was much preferred by the patients compared to having to physically visit 4 reasons for not communicating readings to providers were primarily clinical factors such as no doctor visit, the doctor didn't ask or the patient thinking the doctor wouldn't care. At the conclusion of the survey, the central reporting system for the blood pressure monitoring was over three times more likely to be used by the patients.20 monitoring as well as the delivery of motivational and educational materials via text messages to the intervention group participants. It was found that the intervention group had a significantly higher uptake (80%) in comparison to the traditional, centre-based programme (62%). Adherence in the intervention group was also significantly higher with 94% compared to 68%, the same was also true with the completion rate within the intervention group; 80% compared to 47%. 38 3.2 Heart Failure/Stroke Monitoring This study assesses the attitudes of heart failure patients towards mobile based telehealth monitoring using 20 heart failure patients and 16 clinicians. It was proven that patients preferred using the mobile technology even more than they would using computers. Patients and clinicians agreed that they would happily use the system as long as it was easy to use with clear tangible benefits, it maintained good patient-provider communication and did not increase the workload. 28 3.3 Diabetes A comparative study on the differences in patients complying with web applications compared to mobile applications was conducting on telehealth monitoring diabetes. Patients were given choice of which modality they preferred for the telehealth monitoring and of the 403 there were 291 that chose the app and 112 that chose the web. Demographics of the patients were similar but it was noted that 95% of women preferred the app and only 68% of men preferred the app. It was concluded that different types of data acquisition technologies have an important impact on the effects of a patient’s willingness to use telehealth monitoring. This conclusion was drawn from the Kaplan-Meier analysis which showed a steady decline in compliance using mobile apps over a long period of time and a rapid decline in using the web based application. 15 382 patients were involved in a study relating to home monitoring their knowledge, selfcare and adherence to a heart failure system. Patients were assigned randomly to either home monitoring or a usual care group and received 4 questionnaires via post for assessment purposes. There were baseline differences between the groups for self-care and self-efficacy. However, there was a significant difference in patient knowledge favouring the home monitoring group. After 6 months it was found that self-efficacy and adherence improved in the intervention group using home monitoring. 35 Another study evaluated the impacts of using mobile phones for telehealth monitoring of type 2 diabetes patients. This study involved 30 patients which were randomised into intervention and control groups. Results In a randomised controlled trial with 120 participants using a smartphone-based home care model for cardiac rehabilitation. The smartphone was used for health and exercise 5 favoured the intervention group showing that HbA1c levels improved as did self-efficacy scores. There was no improvement in the control group. One limitation to this study is while it is more feasible for patients to use the technological intervention was not userfriendly. 24 During this run-in period the average compliance was 83% with compliance varying between 6-106%. Following this period was a 4 week follow-up. During this timeframe on days without exacerbation compliance of inhaled medication increased by 12% and ranged between 21-200% per individual. On days when patients should have doubled the intake of inhaled medications compliance decreased by 28% and ranged between 4694%. Additionally out of 10 who should have doubled their inhaled medication only 3 did so. This shows that most people are willing to increase but not double their intake of inhaled medication. Thus, an emphasis on the safety of inhaled medications is needed to reassure patients.37 A study on the use of an internet based telehealth monitoring system for diabetes aimed to investigate if the program improved glycaemic control more effectively than usual care. 248 patients between 35 and 75 years of age were eligible for the internet based program and were treated with insulin. It was found that this innovative means of telehealth monitoring could result in a better performance of self-titration of insulin leading to the improvement of glycaemic control. The ideology is that the patient will discover their own ability to monitor their diabetes resulting in user empowerment. 25 3.5 Chronic Obstructive Pulmonary Disease A systematic review on home monitoring of Chronic Obstructive Pulmonary Disease Patients (COPD) was conducted to explore the patients’ adherence and satisfaction with the use of telemonitoring systems. In total, 17 articles were reviewed of which 12 were published from 2010 to the present. All studies reviewed had similar training and data collection processes but differed in terms of technology used, the duration of telemonitoring and the provision of prompts or feedback. 3.4 Asthma Participants involved in a mobile phone-based monitoring system for asthma found that the system can facilitate guided self-help management. However, it caused a significant dependence on professional/technology support. In the early phases of this trial patients were beginning to understand and control their asthma, however; this evolved into an unhelpful phase of being too dependent on self-managing asthma which raised concerns among health professionals.23 Overall, it was patients were satisfied and found the systems to assist with monitoring their diseases. A constraint however existed with the usability of the systems as it was found that they are lacking in this area and future research should take this into consideration.2 In a study of compliance with inhaled medication and self-treatment guidelines for asthma participants were given a 2 week runin period where compliance with inhaled medication was electronically registered. 6 3.6 Activity Monitoring of Daily Living study there was a non-adherence level of 59.4% based on patient behaviour investigated through electronic monitoring. In the study there were three main reasons reported for the rate of non-adherence which were forgetfulness (22%), lack of time (19%) and good self-perception of health status (19%). 40 Participants in a study involving wireless Triaxial Accelerometer (TA) had a high compliance rate for using the units. The TA unit was worn on 88% of the days throughout the study for an average of 11.2 hours per day. It was found that the system was easy to use and the TA unit was unobtrusive and comfortable to wear which gives reason for the high compliance rate.4 3.8 Well-being In a study on home monitoring systems compliance and technical feasibility of long term health monitoring was conducted on 17 working age participants and 19 elderly participants. Of this, the working age participants collected data for a total of 1406 days with an average participation period of 83 days. In comparison, the elderly participants collected data for a total of 1593 days with an average participation of 84 days. Overall, users gave positive feedback and the study showed that the data-collection rate is between 70 and 90% for monitoring health data. However, an unexpected issues which were raised in this study was thunder storm damage to equipment in homes and scheduling differences between staff and the participants.12 3.7 Lung Function/Respiratory Disease Twelve participants were involved in a feasibility study of an internet-based system for home-monitoring lung transplant recipients. The lung transplant recipients demonstrated that they were able to use the Adherence Enhancement Internet Program (AEIP) with little training, found it acceptable and were generally using it as a tool to maintain or promote adherence.8 In a study measuring the acceptance of an internet-based telemonitoring system providing direct transmission of home spirometry to the hospital overall patient compliance was 55% for 2 measurements a day and 84% for one measurement a day. This study was based on 22 bilateral-lung and heart-lung transplant recipients. It was concluded that the home monitoring of pulmonary function in lung transplant recipients via the internet is feasible and provides reproducible data. However, it only has a mild sensitivity for the detection of acute allograft dysfunction.10 3.9 Cystic Fibrosis Five adolescents were asked to use a home telecare system during a routine hospital visit over one week to monitor Cystic Fibrosis. Patients found that the system easily recorded lung function measurements with no supervision and indicated that it was easy to learn and use. Patients also indicated that feedback provided by the system and ongoing clinical support would determine long-term use and compliance with the monitoring protocol.18 A study measuring adherence to regular selfmonitoring of lung function in 269 lung transplant recipients found that across 22052 measurements performed throughout the 7 3.10 Medical Benefits from Compliance reasons, refusal to wear the device in cold weather, the device was believed to be "too difficult to carry around at work" and the frequency of the telemonitoring requirements was deemed to be too demanding such as 3 times a day on week days. While it was not the focus of this review, it was noted that varying evidence of medical benefits was reported in the papers. Only those papers providing well founded information with thorough quantitative analysis of medical benefits are described here. It is likely that a separate literature review on that topic would reveal many more papers, as different search terms would be chosen to suit that context. Five of the studies that provided information on patient dropouts within the intervention period had a dropout rate of 20% or more as well as low compliance rates of 80% or less. However, in one study it was found that the rate of compliance was high when the patient only had to transmit data once a day, with compliance rates of 98% for oxygen saturation and 83% for respiratory rate. The compliance rate dropped significantly when the patient was recommended to transmit data 3 times per day instead with compliance rates of 79% for oxygen saturation and 60% for respiratory rate. In a study involving intelligent home monitoring a total of 61 alerts were recorded with an average frequency of one alert per month per client. 15 of the 61 alerts were considered genuine but there were no real emergencies recorded for the duration of the study. Many clients in the field trial reported enhanced fields of safety and security which in the long run will assist with alleviating the pressures of living independently. In turn, the monitoring system ultimately increased the range of care choices available to the elderly and improved the role of the carer.22 The reasons for the dropouts were due to usability problems in 2 studies, technical problems in 3 studies and reasons unrelated to the intervention itself but rather the patient's condition in 3 studies. Relocation was a reason for dropouts in 2 studies and patients' death in 4 studies.2 As mentioned previously, a study on diabetes shows that HbA1c levels and self-efficacy of using home monitoring improved, adding an overall health benefit to the patients in the trial. 24 In another systematic review looking at the evidence base for home telemonitoring for chronic diseases it was found that regardless of the patient's nationality, socioeconomic status, or age, generally patients comply with the use of a telemonitoring device/system and programme. It was also found that there is a greater degree of consistency with the clinical effectiveness outcomes in regards to telemonitoring usage in pulmonary or cardiac studies in comparison to diabetes and hypertension. The economics side of telemonitoring usage was mentioned in very 3.11 Systematic Review Findings A systematic review of home telemonitoring in COPD 2 found that all studies had provided information regarding patient dropouts. 3 of the studies provided patient dropout information prior to the intervention and reasons for withdrawal were included in one of the studies, this included: worsening of patient's physical condition, financial-related 8 few studies and in the majority of studies there was no analysis of cost-minimisation.5 4. DISCUSSION 3.12 Multi-site Multi-state Clinical Trials A brief overview of the collective findings reveals the following characteristics: Unfortunately there are comparatively few large projects that specifically examine adherence and compliance across a variety of patient circumstances and delivery settings. The well-publicised Whole Systems Demonstrator project run in the UK was intended to synthesize a large body of evidence from several separate studies and was described by its investigators as a “multisite cluster randomised trial”. 27 Its considerations and findings in terms of compliance appear to have varied widely across the components of the trial, providing some strong anecdotal insights but not a strong systematic contribution in terms of evidence. The studies selected are mainly between 1 to 12 months in duration. The majority (typically 60-70%) of participants in the selected literature are over the age of 50 and male. Sample sizes across the selected literature vary greatly. In general, there is good adherence/compliance at the start of a study that steadily drops off over time, most rapidly in the period immediately after the start. Some broad observations can be made concerning recurring themes with respect to adherence/compliance, in the reviewed studies. The recent CSIRO trial of a home monitoring device for chronic disease at several locations along the east coast of Australia with NBN capability assessed various aspects related to effective use and implementation of a home monitoring service. The aspects of interest are those of the participants’ satisfaction, useability, acceptance, workload, anxiety and strain, all of which are factors associated with compliance or non-compliance. Entry and exit questionnaires were utilised to gather the aforementioned information as well as periodic questionnaires and patient vital signs. Data was expected to be obtained from 125 test patients and up to 250 control patients. Clinical benefits were the focus of the report’s findings however they indirectly imply a “high level of acceptance by patients and their carers”. 39 4.1 Participant Education The greatest level of compliance has been found within the studies involving an education programme for the participants. Across the publications involving an education programme, participants display high levels of compliance throughout most of the duration of a study. It has been noted that when a participant better understands their condition and their role in managing their condition effectively they are far more likely to comply with the instructions provided to them in regards to the home monitoring intervention. The converse is also true: studies without adequate participant education, or no education at all beyond the basic usage of a home monitoring system or device, tend to 9 result in lower compliance for the duration of a study. These effects all apply after the initial startup period of the study, when compliance is almost always at its highest. Non-compliance can also be an issue once technical issues are encountered with a home monitoring device or system. Some study participants are hesitant to report technical failures, feeling as if they have misused the technology rather than realising that the technology itself was at fault. These issues can lead to drops in compliance in random periods of a study and leave gaps in the data collection. 4.2 Age Group Effects Whilst many of the selected papers reported on studies involving elderly participants, of the studies involving a wider age range it was found that elderly participants were generally more compliant throughout a study, compared to middle-aged or young adults. This is most likely due to the fact that elderly participants better understand their condition and value the importance of managing it, compared to younger participants who may not prioritise the nature of their condition as highly as the more elderly participants. 4.4 Support and Independence Participants in some studies have reported they feel home monitoring devices or systems help support them in a way that allows them to have greater flexibility in their life and be more independent when managing their condition. This is one of the strengths of home monitoring compliance: once a participant feels it empowers them, they are far more likely to continue to comply. However, in some cases the opposite is true, participants may feel home monitoring hinders their day to day lives and is more of a burden and a tool that is tedious to deal with. Rather than feel supported or independent, they feel rather dependent and that the device is intrusive on their life. Consequently this leads to non-compliance behaviours. 4.3 Participant Misunderstanding The literature has reported the importance of conveying information correctly and appropriately to potential participants for a study regarding a home monitoring device or system. In a few studies, a handful of potential participants had no interest in taking part in the study, due to the participation instructions and lack of detailed description of what it involves giving them a feeling of it being too “difficult”. In particular, with eligible elderly participants it has been reported that they can confuse a simple home monitoring device which has only a few buttons to operate, with a computer. As they are often hesitant towards computers and lack computer competency, this tends to limit their intake into a study. This results in nonparticipation with otherwise eligible patients, which also further results in smaller sample sizes within studies. 4.5 Motivation Across studies there are clear differences in compliance trends between motivated and demotivated participants. Motivated participants tend to comply consistently for either part of or for the majority of a study, and when given surveys or questionnaires will report high satisfaction with the home monitoring device or system. Demotivated participants will frequently not comply and at the conclusion of a study when given a survey 10 participants, and to relieve fatigue elements experienced by clinicians due to changes in practice associated with Home Telehealth programmes, in conjunction with developing business models for cost containment or neutrality in the delivery pathways, are therefore high priority areas for further consideration. or questionnaire will report forgetfulness or laziness, as well as disinterest in the home monitoring device or system. This direct indication of the association between motivation and compliance appears to be a major but largely unaddressed factor. 5. CONCLUSION From analysis of the High relevance papers selected in this review, it is apparent that there are several areas of differing clinical focus which have attempted comparable patient monitoring tasks within the Home Telehealth domain, and met with generally comparable success rates in terms of compliance. Self-care using telehealth monitoring systems was the major focus of this review, rather than detailed analysis of its use in specific clinical areas. It is not possible to single out a particular clinical area or areas which offer breakthrough approaches for assuring or improving on compliance. It is possible that a clinical area with a more highly tuned model of care depending more closely on the nature of the Home Telehealth intervention, could achieve better compliance than reported levels. Compliance is an aspect of Home Telehealth which has been considered in numerous studies reported in the scientific literature, generally in conjunction with other aspects rather than in isolation. It is apparent from the literature that reliable evidence of compliance rates and factors (including aspects such as retention, adherence, satisfaction) is relatively thin by comparison with analyses of clinical and economic aspects. Existing evidence on compliance has been obtained by different methods, and so is not easily aggregated. It is also apparent that compliance effects have been less rigorously evaluated than is desirable, pointing the way to a need for future work and the desirability of planning for managing compliance in future Home Telehealth projects. The characteristic compliance profile appears to be rapid attrition of some substantial fraction of participants early in a project lifecycle, followed by a more sustained level of participation and much slower further attrition. Factors affecting these two components have not been well explored scientifically, but there is wide agreement that intuitively they include motivational and educational aspects (affecting both patients and careteam members) and the ability to continue providing appropriate support to programmes to enable sustainable long term delivery. Ways to enthuse and inform 11 Potential papers identified from the following sources: PubMed (n = 1111) Google Scholar (n = 6480) Scopus (n = 9089) Remaining papers excluded based on search engine based poorer fit to search Papers retained based on search engine based best fit to search (n = 190) (n = 190) Remaining papers excluded based on title as probable out of scope Papers retained based on title as probable in scope (n = 121) Remaining papers excluded based on keywords and abstract as out of scope Papers retained based on keywords and abstract as in scope (n = 72) High Relevance Papers (n = 40) Moderate Relevance Papers (n = 18) Lower Relevance Papers (n = 14) Figure 1: Summary of literature search methodology for selection and categorization of papers. 12 References 8. Karl, B., Finkelstein, S. and Robiner, W. (2006). The Design of an Internet-Based System to Maintain Home Monitoring Adherence by Lung Transplant Recipients. IEEE Transactions on Information Technology in Biomedicine, 10(1), pp.66-76. High Relevance 1. McCant, F., McKoy, G., Grubber, J., Olsen, M., Oddone, E., Powers, B. and Bosworth, H. (2009). Feasibility of blood pressure telemonitoring in patients with poor blood pressure control. Journal of Telemedicine and Telecare, 15(6), pp.281-285. 9. Scherr, D., Zweiker, R., Kollmann, A., Kastner, P., Schreier, G. and Fruhwald, F. (2006). Mobile phone-based surveillance of cardiac patients at home. Journal of Telemedicine and Telecare, 12(5), pp.255-261. 2. Cruz, J., Brooks, D. and Marques, A. (2014). Home telemonitoring in COPD: A systematic review of methodologies and patients’ adherence. International Journal of Medical Informatics, 83(4), pp.249-263. 10. Morlion, B., Knoop, C., Paiva, M. and Estenne, M. (2002). Internet-based Home Monitoring of Pulmonary Function after Lung Transplantation. American Journal of Respiratory and Critical Care Medicine, 165(5), pp.694-697. 3. Jasemian, Y. (2008). Elderly comfort and compliance to modern telemedicine system at home. 2008 Second International Conference on Pervasive Computing Technologies for Healthcare. 11. Myers, S. (2006). Impact of Home-Based Monitoring on the Care of Patients with Congestive Heart Failure. Home Health Care Management & Practice, 18(6), pp.444-451. 4. Mathie, M., Coster, A., Lovell, N., Celler, B., Lord, S. and Tiedemann, A. (2004). A pilot study of long-term monitoring of human movements in the home using accelerometry. Journal of Telemedicine and Telecare, 10(3), pp.144-151. 12. Merilahti, J., Parkka, J., Antila, K., Paavilainen, P., Mattila, E., Malm, E., Saarinen, A. and Korhonen, I. (2009). Compliance and technical feasibility of long-term health monitoring with wearable and ambient technologies. Journal of Telemedicine and Telecare, 15(6), pp.302-309. 5. Pare, G., Jaana, M. and Sicotte, C. (2007). Systematic Review of Home Telemonitoring for Chronic Diseases: The Evidence Base. Journal of the American Medical Informatics Association, 14(3), pp.269-277. 13. Alwan, M., Dalal, S., Mack, D., Kell, S., Turner, B., Leachtenauer, J. and Felder, R. (2006). Impact of Monitoring Technology in Assisted Living: Outcome Pilot. IEEE Transactions on Information Technology in Biomedicine, 10(1), pp.192-198. 6. Artinian, N., Harden, J., Kronenberg, M., Vander Wal, J., Daher, E., Stephens, Q. and Bazzi, R. (2003). Pilot study of a Web-based compliance monitoring device for patients with congestive heart failure. Heart & Lung: The Journal of Acute and Critical Care, 32(4), pp.226-233. 14. Wade, Wade, and Cartwright, (2012). Factors relating to home telehealth acceptance and usage compliance. Risk Management and Healthcare Policy, p.25. 7. Port, K., Palm, K. and Viigimaa, M. (2005). Daily usage and efficiency of remote home monitoring in hypertensive patients over a oneyear period. Journal of Telemedicine and Telecare, 11(5), pp.34-36. 15. Schreier, G., Eckmann, H., Hayn, D., Kreiner, K., Kastner, P. and Lovell, N. (2012). Web versus App - compliance of patients in a telehealth diabetes management programme using two 13 different technologies. Journal of Telemedicine and Telecare, 18(8), pp.476-480. impact of mobile telephone technology on type 2 diabetic patients’ self-management: the NICHE pilot study. Journal of Evaluation in Clinical Practice, 14(3), pp.465-469. 16. Resnick, H., Ilagan, P., Kaylor, M., Mehling, D. and Alwan, M. (2012). TEAhM— Technologies for Enhancing Access to Health Management: A Pilot Study of Community-Based Telehealth. Telemedicine and e-Health, 18(3), pp.166-174. 25. Roek, M., Welschen, L., Kostense, P., Dekker, J., Snoek, F. and Nijpels, G. (2009). Webbased guided insulin self-titration in patients with type 2 diabetes: the Di@log study. Design of a cluster randomised controlled trial [TC1316]. BMC Family Practice, 10(1), p.40. 17. Cottrell, E., McMillan, K. and Chambers, R. (2012). A cross-sectional survey and service evaluation of simple telehealth in primary care: what do patients think?. BMJ Open, 2(6), pp.e001392-e001392. 26. Botsis, T. and Hartvigsen, G. (2008). Current status and future perspectives in telecare for elderly people suffering from chronic diseases. Journal of Telemedicine and Telecare, 14(4), pp.195-203. 18. Magrabi, F., Lovell, N., Henry, R. and Celler, B. (2005). Designing Home Telecare: A Case Study in Monitoring Cystic Fibrosis. Telemedicine and e-Health, 11(6), pp.707-719. 27. Bower, P., Cartwright, M., Hirani, S., Barlow, J., Hendy, J., Knapp, M., Henderson, C., Rogers, A., Sanders, C., Bardsley, M., Steventon, A., Fitzpatrick, R., Doll, H. and Newman, S. (2011). A comprehensive evaluation of the impact of telemonitoring in patients with long-term conditions and social care needs: protocol for the whole systems demonstrator cluster randomised trial. BMC Health Services Research, 11(1), p.184. 19. Kim, J., Han, H., Song, H., Lee, J., Kim, K. and Kim, M. (2010). Compliance With Home Blood Pressure Monitoring Among Middle-Aged Korean Americans With Hypertension. The Journal of Clinical Hypertension, 12(4), pp.253-260. 20. Huff, L., Zittleman, L., DeAlleaume, L., Bernstein, J., Chavez, R., Sutter, C., LeBlanc, W. and Parnes, B. (2011). What Keeps Patients from Adhering to a Home Blood Pressure Program? The Journal of the American Board of Family Medicine, 24(4), pp.370-379. 28. Seto, E., Leonard, K., Masino, C., Cafazzo, J., Barnsley, J. and Ross, H. (2010). Attitudes of Heart Failure Patients and Health care Providers towards Mobile Phone-Based Remote Monitoring. Journal of Medical Internet Research, 12(4), p.e55. 21. Logan, A., Dunai, A., McIsaac, W., Irvine, M. and Tisler, A. (2008). Attitudes of primary care physicians and their patients about home blood pressure monitoring in Ontario. Journal of Hypertension, 26(3), pp.446-452. 29. Powell, J., Jennings, A., Armstrong, N., Sturt, J. and Dale, J. (2009). Pilot study of a virtual diabetes clinic: satisfaction and usability. Journal of Telemedicine and Telecare, 15(3), pp.150-152. 30. Pinsker, J., Nguyen, C., Young, S., Fredericks, G. and Chan, D. (2011). A pilot project for improving paediatric diabetes outcomes using a website: the Pediatric Diabetes Education Portal. Journal of Telemedicine and Telecare, 17(5), pp.226-230. 22. Sixsmith, A. (2000). An evaluation of an intelligent home monitoring system. Journal of Telemedicine and Telecare, 6(2), pp.63-72. 23. Pinnock, H., Slack, R., Pagliari, C., Price, D. and Sheikh, A. (2007). Understanding the potential role of mobile phone-based monitoring on asthma self-management: qualitative study. Clinical & Experimental Allergy, 37(5), pp.794-802. 31. Hazenberg, C., Bus, S., Kottink, A., Bouwmans, C., Schonbach-Spraul, A. and van Baal, S. (2011). Telemedical home-monitoring of diabetic foot disease using photographic foot 24. Faridi, Z., Liberti, L., Shuval, K., Northrup, V., Ali, A. and Katz, D. (2008). Evaluating the 14 imaging - a feasibility study. Journal Telemedicine and Telecare, 18(1), pp.32-36. of randomised controlled pp.1770-1779. 32. Kenealy, T., Parsons, M., Rouse, A., Doughty, R., Sheridan, N., Hindmarsh, J., Masson, S. and Rea, H. (2015). Telecare for Diabetes, CHF or COPD: Effect on Quality of Life, Hospital Use and Costs. A Randomised Controlled Trial and Qualitative Evaluation. PLoS ONE, 10(3), p.e0116188. trial. Heart, 100(22), 39. Celler, B., Sparks, R., Nepal, S., Alem, L., Varnfield, M., Li, J., Jang-Jaccard, J., McBride, S. and Jayasena, R. (2014). Design of a multi-site multi-state clinical trial of home monitoring of chronic disease in the community in Australia. BMC Public Health, 14(1270). 40. Kugler, C., Gottlieb, J., Dierich, M., Haverich, A., Strueber, M., Welte, T. and Simon, A. (2009). Significance of patient self-monitoring for long-term outcomes after lung transplantation. Clinical Transplantation, 24(5), pp.709-716. 33. Rho, M., Kim, S., Kim, H., Cho, J., Yoon, K., Mun, S. and Choi, I. (2014). Exploring the Relationship Among User Satisfaction, Compliance, and Clinical Outcomes of Telemedicine Services for Glucose Control. Telemedicine and e-Health, 20(8), pp.712-720. Moderate Relevance 34. Mc Namara, K., Versace, V., Marriott, J. and Dunbar, J. (2014). Patient engagement strategies used for hypertension and their influence on self-management attributes. Family Practice, 31(4), pp.437-444. 41. Cho, J., Lee, H., Lim, D., Kwon, H. and Yoon, K. (2009). Mobile communication using a mobile phone with a glucometer for glucose control in Type 2 patients with diabetes: as effective as an Internet-based glucose monitoring system. Journal of Telemedicine and Telecare, 15(2), pp.77-82. 35. Boyne, J., Vrijhoef, H., Spreeuwenberg, M., De Weerd, G., Kragten, J. and Gorgels, A. (2013). Effects of tailored telemonitoring on heart failure patients' knowledge, self-care, self-efficacy and adherence: A randomized controlled trial. European Journal of Cardiovascular Nursing, 13(3), pp.243-252. 42. Cassimatis, M. and Kavanagh, D. (2012). Effects of type 2 diabetes behavioural telehealth interventions on glycaemic control and adherence: a systematic review. Journal of Telemedicine and Telecare, 18(8), pp.447-450. 36. Jones, M., Greenfield, S., Bray, E., Hobbs, F., Holder, R., Little, P., Mant, J., Williams, B. and McManus, R. (2013). Patient self-monitoring of blood pressure and self-titration of medication in primary care: the TASMINH2 trial qualitative study of health professionals’ experiences. British Journal of General Practice, 63(611), pp.378-385. 43. Kugler, C., Fuehner, T., Dierich, M., DeWall, C., Haverich, A., Simon, A., Welte, T. and Gottlieb, J. (2009). Effect of Adherence to Home Spirometry on Bronchiolitis Obliterans and Graft Survival After Lung Transplantation. Transplantation, 88(1), pp.129-134. 37. van der Palen, J., Klein, J. and Rovers, M. (1997). Compliance with inhaled medication and self-treatment guidelines following a selfmanagement programme in adult asthmatics. European Respiratory Journal, 10(3), pp.652-657. 44. Ramaekers, B., Janssen-Boyne, J., Gorgels, A. and Vrijhoef, H. (2009). Adherence Among Telemonitored Patients with Heart Failure to Pharmacological and Nonpharmacological Recommendations. Telemedicine and e-Health, pp.517-524. 38. Varnfield, M., Karunanithi, M., Lee, C., Honeyman, E., Arnold, D., Ding, H., Smith, C. and Walters, D. (2014). Smartphone-based home care model improved use of cardiac rehabilitation in postmyocardial infarction patients: results from a 45. de Lusignan, S., Wells, S., Johnson, P., Meredith, K. and Leatham, E. (2001). Compliance 15 and effectiveness of 1 year's home telemonitoring. The report of a pilot study of patients with chronic heart failure. European Journal of Heart Failure, 3(6), pp.723-730. 54. Tarassenko, L., Velardo, C., Shah, A., Gibson, O., Clifford, G., Heneghan, C., Rutter, H. and Farmer, A. (2013). M-health for long-term management of COPD. International Journal of Integrated Care, 10(1). 46. Port, K., Palm, K. and Viigimaa, M. (2003). Self-reported compliance of patients receiving antihypertensive treatment: use of a telemonitoring home care system. Journal of Telemedicine and Telecare, 9(suppl 1), pp.65-66. 55. Taha, N., El-Azeaz, M. and El-Razik, B. (2011). Factors affecting compliance of diabetic patients toward therapeutic management. The Medical Journal of Cairo University, 79(2). 47. Bobrie, G., Postelvinay, N., Delonca, J. and Corvol, P. (2007). Self-Measurement and SelfTitration in HypertensionA Pilot Telemedicine Study. American Journal of Hypertension, 20(12), pp.1314-1320. 56. Glynn, L., Murphy, A., Smith, S., Schroeder, K. and Fahey, T. (2010). Self-monitoring and other non-pharmacological interventions to improve the management of hypertension in primary care: a systematic review. British Journal of General Practice, 60(581), pp.476-488. 48. Boise, L., Wild, K., Mattek, N., Ruhl, M., Dodge, H. and Kaye, J. (2013). Willingness of older adults to share data and privacy concerns after exposure to unobtrusive in-home monitoring. Gerontechnology, 11(3). 57. Hall, A., Dodd, V., Harris, A., McArthur, K., Dacso, C. and Colton, L. (2014). Heart Failure Patients' Perceptions and Use of Technology to Manage Disease Symptoms. Telemedicine and eHealth, 20(4), pp.324-331. 49. Finkelstein, S., Snyder, M., Edin-Stibbe, C., Chlan, L., Prasad, B., Dutta, P., Lindgren, B., Wielinski, C. and Hertz, M. (1996). Monitoring progress after lung transplantation from homepatient adherence. Journal of Medical Engineering & Technology, 20(6), pp.203-210. 58. Varnfield, M., Karunanithi, M., Särelä, A., Garcia, E., Fairfull, A., Oldenburg, B. and Walters, D. (2011). Uptake of a technology-assisted homecare cardiac rehabilitation program. The Medical Journal of Australia, 194(4). 50. Bailey, W. (1990). A randomized trial to improve self-management practices of adults with asthma. Archives of Internal Medicine, 150(8), pp.1664-1668. Lower Relevance 51. Hoban, M., Fedor, M., Reeder, S. and Chernick, M. (2013). The Effect of Telemonitoring at Home on Quality of Life and Self-Care Behaviors of Patients with Heart Failure. Home Healthcare Nurse, 31(7), pp.368-377. 59. Marshall, A., Medvedev, O. and Antonov, A. (2008). Use of a Smartphone for Improved SelfManagement of Pulmonary Rehabilitation. International Journal of Telemedicine and Applications, 2008, pp.1-5. 52. Wagner, S., Toftegaard, T. and Bertelsen, O. (2013). Introducing the Adherence Strategy Engineering Framework (ASEF). Methods of Information in Medicine, 52(3), pp.220-230. 60. Kang, H., Mahoney, D., Hoenig, H., Hirth, V., Bonato, P., Hajjar, I. and Lipsitz, L. (2010). In Situ Monitoring of Health in Older Adults: Technologies and Issues. Journal of the American Geriatrics Society, 58(8), pp.1579-1586. 53. Janson, S., Fahy, J., Covington, J., Paul, S., Gold, W. and Boushey, H. (2003). Effects of individual self-management education on clinical, biological, and adherence outcomes in asthma. The American Journal of Medicine, 115(8), pp.620626. 61. Biddiss, E., Brownsell, S. and Hawley, M. (2009). Predicting need for intervention in individuals with congestive heart failure using a 16 home-based telecare system. Journal Telemedicine and Telecare, 15(5), pp.226-231. of 70. Frantz, A. (2003). Current Issues Related to Home Monitoring. AACN Clinical Issues: Advanced Practice in Acute and Critical Care, 14(2), pp.232-239. 62. van den Berg, N., Schumann, M., Kraft, K. and Hoffmann, W. (2012). Telemedicine and telecare for older patients—A systematic review. Maturitas, 73(2), pp.94-114. 71. López-Viña, A. and Del Castillo-Arévalo, F. (2000). Influence of peak expiratory flow monitoring on an asthma self-management education programme. Respiratory Medicine, 94(8), pp.760-766. 63. Tuomisto, M., Terho, T., Korhonen, I., Lappalainen, R., Tuomisto, T., Laippala, P. and Turjanmaa, V. (2006). Diurnal and weekly rhythms of health-related variables in home recordings for two months. Physiology & Behavior, 87(4), pp.650658. 72. Kolbe, J. (2002). The Influence of Socioeconomic and Psychological Factors on Patient Adherence to Self-Management Strategies. Disease Management & Health Outcomes, 10(9), pp.551-570. 64. Liddy, C., Dusseault, J., Dahrouge, S., Hogg, W., Lemelin, J. and Humbert, J. (2008). Telehomecare for patients with multiple chronic illnesses. Canadian Family Physician, 54(1), pp.5865. 65. Mehra, M., Uber, P., Chomsky, D. and Oren, R. (2000). Emergence of Electronic Home Monitoring in Chronic Heart Failure: Rationale, Feasibility, and Early Results With the HomMed Sentry?-Observer? System. Congestive Heart Failure, 6(3), pp.137-139. 66. Bondmass, M., Bolger, N., Gastro, G. and Avitall, B. (1998). The Effect of Physiologic Home Monitoring and Telemanagement on Chronic Heart Failure Outcomes. The Internet Journal of Advanced Nursing Practice, 3(2). 67. Bondmass, M., Bolger, N., Castro, G. and Avitall, B. (2000). The Effect of Home Monitoring and Telemanagement on Blood Pressure Control Among African Americans. Telemedicine Journal, 6(1), pp.15-23. 68. Martínez, A., Everss, E., Rojo-Álvarez, J., Figal, D. and García-Alberola, A. (2006). A systematic review of the literature on home monitoring for patients with heart failure. Journal of Telemedicine and Telecare, 12(5), pp.234-241. 69. Cardozo, L. and Steinberg, J. (2010). Telemedicine for Recently Discharged Older Patients. Telemedicine and e-Health, 16(1), pp.4955. 17 Appendix # 1 Relev ance High Year 2009 2 High 3 Paper Type of Modality Area of Health Feasibility of blood pressure telemonitoring in patients with poor blood pressure control Blood Pressure telemonitoring device Blood Pressure 2014 Home telemonitoring in COPD: A systematic review of methodologies and patients' adherence Home telemonitoring systems Chronic Obstructive Pulmonary Disease (COPD) High 2008 Elderly comfort and compliance to modern telemedicine system at home Wireless telemedicine system at home 4 High 2004 A pilot study of long-term monitoring of human movements in the home using accelerometry 5 High 2007 6 High 7 High Sample Size Duration P Value 591 participants First 6 months Yes Systematic Review 17 articles included June to August 2012 Heart Failure Feasibility Study 1 week Wireless triaxial accelerometer (TA) Activity Monitoring of Daily Living Feasibility Study 24 non risky elderly heart patients (aged 60 +/- 5 years) (12 male, 12 female) 6 participants aged 80-86 years old Systematic review of home telemonitoring for chronic diseases: the evidence base Home telemonitoring Chronic Diseases Systematic Review 65 articles included 1990 to 2006 2003 Pilot study of a Webbased compliance monitoring device for patients with congestive heart failure Self-care compliance device and webbased monitoring system Heart Failure Pilot Study, Randomised Controlled Trial 3 months Yes 2005 Daily usage and efficiency of Home self-monitored Blood Pressure Feasibility Study 18 participants (17 male, 1 female) (aged 50 to 87 years old) 50 participants 12 months Yes 18 Type of Evaluation/Analysis Randomised Controlled Trial 2 to 3 months Aus Yes remote home monitoring in hypertensive patients over a one-year period blood pressure (26 male, 17 female) (mean age 54) (7 exclusions) 12 participants 8 High 2006 The design of an Internetbased system to maintain home monitoring adherence by lung transplant recipients Home monitoring internet-based system Lung Function Feasibility Study 9 High 2006 Mobile phone-based surveillance of cardiac patients at home Home monitoring system Heart Failure Feasibility Study 20 participants (mean age 50 years) 10 High 2002 Internet-based home monitoring of pulmonary function after lung transplantation Internet-based telemonitoring system Pulmonary Function Prospective Study 22 participants 11 High 2006 Impact of home-based monitoring on the care of patients with congestive heart failure Home-based telemonitoring Heart Failure Feasibility Study 83 participants 2 months Yes 12 High 2009 Compliance and technical feasibility of long-term health monitoring with wearable and ambient technologies Home monitoring system Well-being Feasibility Study 17 working-age participants and 19 elderly participants 13 High 2006 Impact of monitoring technology in assisted living: outcome pilot Monitoring technology in assisted living Activity Monitoring of Daily Living Outcome Pilot 22 participants (7 male, 15 female) (mean age 83.79) Working-age participants total of 1406 days and elderly participants total of 1593 days 3 months Yes 19 12 months Monitored for 90 days each (1735 days total) June 1998 to September 2000 Yes 14 High 2012 Factors relating to home telehealth acceptance and usage compliance In-home telehealth (medical alarm pendant) Vital Signs Randomised Controlled Trial 15 High 2012 Web versus App– compliance of patients in a telehealth diabetes management programme using two different technologies Mobile app and web interface Diabetes Feasibility Study 16 High 2012 TEAhM—Technologies for Enhancing Access to Health Management: A Pilot Study of Community-Based Telehealth Telehealth kiosks Blood Pressure Pilot Study, Randomised Controlled Trial 17 High 2012 A cross-sectional survey and service evaluation of simple telehealth in primary care: what do patients think? Home blood pressure readings texted to a server Blood Pressure Cross-sectional survey 18 High 2005 Designing home telecare: a case study in monitoring cystic fibrosis Home telecare system Cystic Fibrosis Case Study 5 participants (adolescents) 1 week 19 High 2010 Compliance With Home Blood Pressure Monitoring Among Middle‐Aged Korean Americans With Hypertension Home blood pressure monitoring Blood Pressure Prospective Trial 48 weeks Yes 20 High 2011 What keeps patients from adhering to a home blood Home blood pressure monitoring Blood Pressure Random Quota Sample 377 participants (age range 40 to 64 years old) (49.3%/50.7% male/female) 316 participants (mean age 61.4) N/A Yes 20 61 participants and 29 carers (age range of 63-95 years old) (mean age of 80 years) 403 participants (341 male, 62 female) (291 mainly used the mobile app, 112 mainly used the web interface) 112 participants (73 controls, 43 intervention) (mean 74.1 years old) (25% male, 75% female) 124 participants 12 or 24 weeks Yes Yes Up to 767 days usage Yes Yes 10 months 13 weeks Yes pressure program? 21 High 2008 Attitudes of primary care physicians and their patients about home blood pressure monitoring in Ontario 22 High 2000 An evaluation of an intelligent home monitoring system 23 High 2007 24 High 25 26 (35.1% male, 64.9% female) 149 participants Home blood pressure monitoring Blood Pressure Randomised Survey Intelligent home monitoring system Activity Monitoring of Daily Living Field Trial 22 participants (age range from 60s to over 85) 3 months Understanding the potential role of mobile phone‐based monitoring on asthma self‐management: qualitative study Mobile phone-based monitoring Asthma Qualitative Study 4 weeks 2008 Evaluating the impact of mobile telephone technology on type 2 diabetic patients'self‐management: the NICHE pilot study Mobile phone-based self management Diabetes Randomised Controlled Trial High 2009 Web-based guided insulin self-titration in patients with type 2 diabetes: the Di@ log study. Design of a cluster randomised controlled trial [TC1316] Web-based diabetes management Diabetes Randomised Controlled Trial 48 participants (34 adults and teenagers with asthma, 14 asthma nurses and doctors) 30 participants (majority female with mean age 55.3 years in intervention group and 56.7 years in control group) 248 participants (aged between 35-75 years) High 2008 Current status and future perspectives in telecare for elderly people suffering from Home telecare Chronic Disease Literature Review 21 54 articles selected for further N/A 3 months 12 months Published between 1990 and 2007 Yes chronic diseases A comprehensive evaluation of the impact of telemonitoring in patients with long-term conditions and social care needs: protocol for the whole systems demonstrator cluster randomised trial Attitudes of heart failure patients and health care providers towards mobile phone-based remote monitoring 27 High 2011 28 High 2010 29 High 2009 Pilot study of a virtual diabetes clinic: satisfaction and usability 30 High 2011 31 High 2011 32 High 2015 33 High 2014 A pilot project for improving paediatric diabetes outcomes using a website: the Pediatric Diabetes Education Portal Telemedical homemonitoring of diabetic foot disease using photographic foot imaging–a feasibility study Telecare for Diabetes, CHF or COPD: Effect on Quality of Life, Hospital Use and Costs. A Randomised Controlled Trial and Qualitative Evaluation. Exploring the relationship Home monitoring system Heart Failure, Diabetes and COPD Randomised Controlled Trial Mobile phone-based remote monitoring Heart Failure Mixed Methods Study Virtual diabetes clinic Diabetes Feasibility Study Paediatric Diabetes Education Portal Diabetes Pilot Trial, Feasibility Study Photographic foot imaging device (telemonitoring tool) Diabetes Electronic device data uploading Telemedicine service examination 6,000 participants (approximately) 12 months Yes Questionnaire administered to 100 patients. Semi-structured interviews with 20 patients and 16 clinicians 17 participants (6 males, 11 females) (age range 22-70 years old) 52 participants Questionnaire Sep 2009 to Feb 2010. Interviews Apr 2008 to Feb 2009. Yes Feasibility Study 22 participants 4 months Diabetes Randomised Controlled Trial and Qualitative Evaluation 171 participants (n = 98 intervention, n= 73 control) 3 to 6 months Diabetes Assessment of user Data collected N/A 22 6 months 6 months Yes Yes 34 High 2014 35 High 2013 36 High 2013 37 High 1997 38 High 2014 among user satisfaction, compliance, and clinical outcomes of telemedicine services for glucose control. Patient engagement strategies used for hypertension and their influence on selfmanagement attributes. Effects of tailored telemonitoring on heart failure patients' knowledge, self-care, selfefficacy and adherence: a randomized controlled trial. Patient self-monitoring of blood pressure and selftitration of medication in primary care: the TASMINH2 trial qualitative study of health professionals' experiences. Compliance with inhaled medication and selftreatment guidelines following a selfmanagement programme in adult asthmatics Smartphone-based home care model improved use of cardiac rehabilitation in postmyocardial infarction patients: results from a randomised controlled trial satisfaction Home blood pressure monitoring Blood Pressure Survey Telemonitoring device Heart Failure Randomised Controlled Trial Home blood pressure monitoring Blood Pressure Randomised Controlled Trial and Qualitative Study Asthma selfmanagement (peak expiratory flow (PEF) electronically registered) Asthma Evaluation of Self management programme Home monitoring through smart phone use Heart Failure Randomised Controlled Trial 23 from 81 patients who used telemedicine services 215 surveys returned (twothirds of participants aged over 65 years old) 382 (aged 71 +/SD 11.2 years) Semi-structured interviews with 13 GPs, 2 practice nurses and 1 healthcare assistant 24 participants (age range 1865 years old) 120 participants in traditional centre-based programme (n=60) and care assessment N/A 12 months Yes Yes N/A 6 weeks Yes 6 week cardiac rehabilitation and 6 month selfmaintenance Yes Yes 39 High 2014 Design of a multi-site multistate clinical trial of home monitoring of chronic disease in the community in Australia Telemedcare Clinical Monitoring Unit (CMU) Chronic Disease Intervention Control Study 40 High 2009 Home spirometry device Lung Function Retrospective, Cross Sectional Study 41 Mod 2009 Mobile phone with glucometer Diabetes Randomised Controlled Trial 42 Mod 2012 Diabetes selfmanagement Diabetes Systematic Review 43 Mod 2009 Significance of patient self‐monitoring for long‐term outcomes after lung transplantation Mobile communication using a mobile phone with a glucometer for glucose control in Type 2 patients with diabetes: as effective as an Internet-based glucose monitoring system Effects of type 2 diabetes behavioural telehealth interve ntions on glycaemic control and adherence: a systematic review Effect of adherence to home spirometry on bronchiolitis obliterans and graft survival after lung transplantation Home spirometry Lung Transplantation 7-year Prospective Cohort Study 44 Mod 2009 Telemonitoring Heart Failure Randomised Controlled Trial Adherence among telemonitored patients with heart failure to pharmacological and nonpharmacological recommendations 24 platform cardiac rehabilitation (n=60) 25 test patients each site (n=125) and 50 case matched control patients (n=250) 298 participants period 6-18 months Yes 3 months Yes 69 participants 3 months Yes 49 articles selected from 1027 results. 14 met criteria for inclusion 226 participants N/A 101 participants Nonadherence assessed longitudinally for 24 months 3 months Yes Yes Yes Yes 45 Mod 2001 46 Mod 2003 47 Mod 2007 48 Mod 2013 49 Mod 1996 50 Mod 1990 51 Mod 2013 52 Mod 2013 Compliance and effectiveness of 1 year's home telemonitoring. The report of a pilot study of patients with chronic heart failure Self-reported compliance of patients receiving antihypertensive treatment: use of a telemonitoring home care system Self-Measurement and SelfTitration in Hypertension* A Pilot Telemedicine Study Willingness of older adults to share data and privacy concerns after exposure to unobtrusive in-home monitoring Monitoring progress after lung transplantation from home-patient adherence A randomized trial to improve selfmanagement practices of adults with asthma The effect of telemonitoring at home on quality of life and self-care behaviors of patients with heart failure. Introducing the Adherence Strategy Engineering Framework (ASEF). Support for developing technologybased self-care solutions. Telemonitoring Heart Failure Pilot Study, Randomised Controlled Trial 20 participants (10 controls, 10 intervention) (mean age 75.2 years old) 50 participants (mean age 52 years old) 12 months Home-monitoring of blood pressure Blood Pressure Evaluation Home-monitoring of blood pressure Blood Pressure Multicenter, prospective, singlegroup, open-label pilot study Longitudinal Study 111 participants 8 weeks Yes Home-monitoring and computer use (in-home sensors) Human Movement 119 participants 12 months Yes Electronic spirometer/diary instrument Heart/lung transplantation Feasibility Study 41 participants (24 female, 17 male) 12 months 80 participants (40 intervention, 40 control) 7 case studies, 25 participants 90 days 12 months Randomised Controlled Trial Home-monitoring of blood pressure Heart Failure Randomised Controlled Trial (prospective design) Home-monitoring of blood pressure Blood Pressure Case Studies, Feasibility Study, Conceptual Framework 25 53 Mod 2003 Effects of individual selfmanagement education on clinical, biological, and adherence outcomes in asthma M-health for long-term management of COPD 54 Mod 2013 55 Mod 2011 56 Mod 2010 57 Mod 2014 58 Mod 2011 Uptake of a technologyassisted home-care cardiac rehabilitation program 59 Low 2008 Use of a smartphone for improved self-management of pulmonary rehabilitation Factors affecting compliance of diabetic patients toward therapeutic management Self-monitoring and other non-pharmacological interventions to improve the management of hypertension in primary care: a systematic review Heart failure patients' perceptions and use of technology to manage disease symptoms. Asthma selfmanagement Asthma Randomised Controlled Trial 65 participants (adults) 7 weeks Self-management application on a tablet device Therapeutic management COPD Feasibility Study 23 participants 1189 monitoring days Diabetes Descriptive Correlational Design 80 participants (23 males and 57 females) Self-monitoring interventions Blood Pressure Systematic Review 72 Randomised Controlled Trials met the inclusion criteria Blood pressure device or bathroom scale Heart Failure Qualitative Analysis 15 participants (mean age 64.43 years) Mobile phone and web based home monitoring Heart Failure Randomised Controlled Trial Exercise programme and selfmanagement at home with smart phone COPD Pilot Application Traditional cardiac rehab (control group n=80) vs Care Assessment Plan (intervention group n=80) Full user assessment and clinical evaluation being planned 26 Yes Yes 6 weeks N/A Yes 60 Low 2010 61 Low 2009 62 Low 2012 63 Low 2006 64 Low 2008 65 Low 2000 66 Low 1999 67 Low 2000 In situ monitoring of health in older adults: technologies and issues Predicting need for intervention in individuals with congestive heart failure using a home-based telecare system Telemedicine and telecare for older patients—a systematic review Home monitoring devices Geriatric Care Report N/A N/A Telecare monitoring system Heart Failure Feasibility Study 45 participants (elderly) 18 months Various Home monitoring based devices and systems Chronic Disease (generalised) Systematic Review 68 papers Diurnal and weekly rhythms of health-related variables in home recordings for two months Telehomecare for patients with multiple chronic illnesses Pilot study Home monitoring system Physiological measurements (well-being) Feasibility Study 14 participants (all middle-aged males) Papers published between 2007 and Feb 2012 50 to 79 days Home monitoring system Chronic Disease (generalised) Pilot Study (mixed method) 9 to 339 days Emergence of Electronic Home Monitoring in Chronic Heart Failure: Rationale, Feasibility, and Early Results With the HomMed Sentry™‐Observer™ System The effect of physiologic home monitoring and telemanagement on chronic heart failure outcomes The effect of home Home monitoring system Heart Failure Multicenter Study 8 physicians and 5 nurses caring for approx 10,000 patients (sample of 22 from RCT on 240 patients) 53 participants (78% male, 72% Caucasian, age range 17-79 years) Home monitoring system Heart Failure Feasibility Study 2 to 3 months Yes Home monitoring Blood Pressure Feasibility Study 60 participants (61 +/- 13 years, 62% African American, 67% female) 33 participants 1 to 3 months Yes 27 Statisti cal Measur es 3 months 68 Low 2006 69 Low 2010 70 Low 2003 71 Low 2000 72 Low 2002 monitoring and telemanagement on blood pressure control among African Americans A systematic review of the literature on home monitoring for patients with heart failure Telemedicine for recently discharged older patients Current issues related to home monitoring Influence of peak expiratory flow monitoring on an asthma selfmanagement education programme The influence of socioeconomic and psychological factors on patient adherence to selfmanagement strategies system (African Americans, age 51.5 +/14.3, 70% female) 42 articles included of 383 read Home monitoring systems Heart Failure Systematic Review Home-based casemanaged telemedicine Home-monitoring Chronic Diseases Observational Study 851 patients 1951 to April 2004 (varies depending on database) 2 months Chronic Diseases Review Article N/A N/A Home monitoring Self-management Asthma Randomised Controlled Trial 100 participants (aged 17-65 years) 12 months Self-management strategies Asthma Review Article N/A N/A 28 Yes Yes