Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
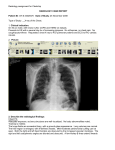
Pulmonary Edema Associated With Scuba Diving* Case Reports and Review John B. Slade, Jr, MD; Takashi Hattori, MD; Carolyn S. Ray, MD; Alfred A. Bove, MD, PhD; Paul Cianci, MD Acute pulmonary edema has been associated with cold-water immersion in swimmers and divers. We report on eight divers using a self-contained underwater breathing apparatus (scuba) who developed acute pulmonary edema manifested by dyspnea, hypoxemia, and characteristic chest radiographic findings. All cases occurred in cold water. All scuba divers were treated with complete resolution, and three have returned to diving without further episodes. Mechanisms that would contribute to a raised capillary transmural pressure or to a reduced blood-gas barrier function or integrity are discussed. Pulmonary edema in scuba divers is multifactorial, and constitutional factors may play a role. Physicians should be aware of this potential, likely underreported, problem in scuba divers. (CHEST 2001; 120:1686 –1694) Key words: altitude sickness; diving; hypoxia; immersion; pulmonary edema; respiratory distress syndrome; swimming Abbreviations: ECM ⫽ extracellular matrix; fsw ⫽ feet of sea water; HAPE ⫽ high-altitude pulmonary edema; msw ⫽ meters of sea water; scuba ⫽ self-contained underwater breathing apparatus pulmonary edema has been described preA cute viously in swimmers and divers using a selfcontained underwater breathing apparatus (scuba).1– 6 The prevalence of pulmonary edema during scuba diving and surface swimming is unknown but is probably underreported. In a survey4 of 1,250 divers, of the 460 responders, 5 (1.1%) had a history suggestive of pulmonary edema. With ⬎ 3 million scuba divers currently in the United States alone, literally thousands of divers could be at risk for developing pulmonary edema. Acute pulmonary edema occurs when the pulmonary capillary permeability is increased (noncardiogenic), when the pulmonary capillary hydrostatic pressure exceeds the plasma oncotic pressure (cardiogenic), or both. In swimmers and divers, an increased transalveolar pressure gradient due to a combination of factors has been implicated in the pathogenesis of the condition. The final common pathway appears to be stress failure of pulmonary capillaries manifested by leaks in the capillary endothelial layer and the alveolar epithe*From Doctors Medical Center (Drs. Slade, Ray, and Cianci), San Pablo, CA; Community Hospital of the Monterey Peninsula (Dr. Hattori), Monterey, CA; and Temple University Medical Center (Dr. Bove), Philadelphia, PA. Manuscript received August 24, 1999; revision accepted March 27, 2001. Correspondence to: John B. Slade, Jr, MD, Doctors Medical Center, San Pablo, San Pablo, CA 94806; e-mail: [email protected] lial layer, and sometimes the breakdown of the full thickness of the alveolar wall leading to highpermeability pulmonary edema or even frank hemorrhage.7 The exact nature of the stress in scuba divers and immersion victims is not clear but may be due to raised pulmonary capillary pressure from systemic sympathetic discharge, the development of high negative intrathoracic pressure due to multiple factors, or as-yet undefined biochemical or adrenergic responses to conditions encountered during swimming and diving. As in high-altitude pulmonary edema (HAPE), constitutional factors may predispose a subgroup of individuals to the development of pulmonary edema with scuba diving or water immersion. The occurrence of hypoxemia or severe acid-base abnormalities make prompt recognition and treatment important.8 Materials and Methods Information was collected on scuba divers from 1986 to 1999, who were referred to the Pacific Grove Hyperbaric Facility in Monterey, CA, the John Muir Medical Center in Walnut Creek, CA, or Doctors Medical Center in San Pablo, CA, for the evaluation of pulmonary edema that developed during diving. Data regarding patient diving history, details of incident dives, medications, medical history including prior episodes, laboratory and radiograph evaluations, treatments, and outcomes were reviewed and are summarized in Table 1. 1686 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21969/ on 04/29/2017 Reviews Discussion The pathophysiologic mechanisms for the development of acute pulmonary edema in apparently otherwise healthy scuba divers are not clear. In most divers, the pulmonary edema occurs without an obvious precipitating cause, can occur in shallow or deep dives and in cold or warm water, and has been reported in swimmers.2–4 Patients may have arterial blood gas findings of acidosis and hypoxemia, chest radiographic abnormalities, rarely have evidence of heart failure, and survivors respond completely to conventional therapy for pulmonary edema. Water aspiration may be a contributing or causative factor and should be considered. In our series of eight patients, the only obvious factor common to all was the history of scuba diving. Other possible contributing factors included but were not limited to, poor physical conditioning, cold water exposure, immersion effects, strenuous exer- Table 1—Case Summaries* Variables Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8 Age, yr/sex 52/M 61/M 46/F 53/F 58/F 55/F 49/F 45/M Scuba history 20 yr Experienced First dive Prior experience ⬎ 140 dives New diver 2 yr Not documented Maximum depth 85 fsw 20 fsw 15 fsw 110 fsw 110 fsw 45 fsw Unknown 40–60 fsw (26 msw) (6 msw) (4.6 msw) (33.8 msw) (33.8 msw) (13.8 msw) Water temperature 55°F 55°F 55°F 50–55°F 80s°F 50–55°F Cold 50–55°F Symptom onset Prior to ascent Prior to ascent At depth At 20 fsw During ascent At depth On surfacing At 15 fsw Symptoms and signs on Dyspnea and Dyspnea, N2 narcosis (?), Cough (frothy, pink Severe dyspnea Copious, Cough (clear, surfacing hemoptysis Dyspnea, hemoptysis hemoptysis aspirated at (fatigue with (cyanosis on surface, dive prior surfacing) hemoptysis sputum) (12–18 msw) frothy copious yellow hemoptysis fluid) day) History of symptoms and 1 wk prior No No HTN HTN, arthritis HTN, asthma Yes No Yes No Unknown Unremarkable Allergies, no Asthma, depression Childhood Chronic atrial signs Medical history asthma Family history CAD, HTN CAD, DM Medications Metoprolol Thyroid, 1 g/d; Atenolol D/C 5 mo prior Not listed asthma fibrillation (1 yr) Unremarkable CHF, CVA, cancer Unremarkable Unremarkable Not listed None ND Fluoxetine, nortryptyline None indomethacin medroxyprogesterone prn acetate, estrogens Digoxin, warfarin, Sotalol Cigarettes No No No No No No No (prior) No Alcohol consumption No Rare No Occasional Moderate Moderate Unknown Occasional Physical examination BP, 160/100; P, BP, 154/100; BP, 204/P; P, BP, 80/60, P, 100 BP, 172/72; 2/6 BP, 120/80; trace lower BP, 110/70; Bibasilar rales; heart: 84 beats/min; P, 96 beats/ 80 beats/min; beats/min; R, 18 breaths/ min; R, 22 R, 22 diffuse bilateral no rub or min; bilateral breaths/min; breaths/min; rales murmur rales bibasilar bilateral rales; rales Chest radiograph Bilateral perihilar Retic-nodular Bilateral diffuse Bilateral pulmonary Anterior, patchy infiltrates; heart bilateral pulmonary patchy perihilar vascular normal. infiltrates; edema alveolar congestion Room air: heart: click, RRR, no murmur pulmonary edema None obtained Bibasilar infiltrates L ⬎ R and mild cardiomegaly densities. Heart normal. Room air: 7.31/ extremity edema obesity Diffuse heart Blood gas measurements at systolic murmur normal. ED-100% O2: Room air: 7.33/37/ ND ND ND Sao2 (room air) 91– presentation, pH/Pao2/ 52/42; 5 L O2: 7.13/44/41; 7.27/192/46; 31; 100% O2: 94%; ECG: afib, Paco2 7.33/97/46 40% O2: ICU-4 L O2: 7.3/105/34 ventricular rate 7.4/73/42 7.34/57/43 110 beats/min; CPK 124 (NL) Diagnostic studies V̇/Q̇ scan (⫺) for ND ECG (⫺) PE; ETT (⫺); Lactic acid, 3.7 (0.5–2.2 nmol/L) CKMB (⫺) CPK (⫺); cardiolyte PFTs (⫺); ETT (⫺); scan (⫺); ETT ND stress echo (⫺) rate 110 beats/ (⫺); ECG: min; echo normal; LBBB Treatment Furosemide, O2 NTG, 40% O2 by Venti-mask Furosemide, O2 Furosemide, O2 by Furosemide, O2 albuterol, K⫹ ECG: afibrillation CPK (⫺) ND ND mask Furosemide, O2, ciprofloxacin diltiazem Resumed scuba Yes Unknown Unknown Unknown Yes Yes Unknown Unknown *M ⫽ male; F ⫽ female; CAD ⫽ coronary artery disease; HTN ⫽ hypertension; DM ⫽ diabetes mellitus; CVA ⫽ cerebrovascular accident; CHF ⫽ congestive heart failure; P ⫽ pulse; R ⫽ respiration; Sao2 ⫽ arterial oxygen saturation; ED ⫽ emergency department; RRR ⫽ regular rate and rhythm; CPK ⫽ creatinine phosphokinase; PE ⫽ pulmonary embolism; ETT ⫽ exercise tolerance test; CKMB ⫽ creatine kinase MB; (⫺) ⫽ negative; NTG ⫽ nitroglycerin; echo ⫽ echocardiogram; PFT ⫽ pulmonary function test; LBBB ⫽ left bundle-branch block; V̇/Q̇ ⫽ ventilation/perfusion; afib ⫽ afibrillation; D/C ⫽ discontinued; NL ⫽ normal; ND ⫽ not documented; ? ⫽ condition suspected. CHEST / 120 / 5 / NOVEMBER, 2001 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21969/ on 04/29/2017 1687 tion, tight-fitting wet suit, anxiety, malfunctioning regulators or other equipment, aspiration, and hypertension. All the patients in this report were middle-aged (age range, 46 to 61 years) people of average fitness. The water temperature was 50 to 55°F for six of the divers, in the low 80s for one, and was recorded as “cold” for one. None of the patients reported having strenuous exertion during the dive. One diver (case 5) had a wet suit that was too tight and was considerably apprehensive during her dive. There were no reports of equipment malfunction, but one diver (case 2) ran out of air on the day prior to his incident dive, had to “buddy-breathe” with his diving instructor, and complained of significant postdive fatigue that evening. The fatigue had resolved by the next morning when he developed pulmonary edema during his first scuba dive that day. Aspiration is included in the differential diagnosis of one diver (case 4) but is unlikely because she became symptomatic during ascent at about 20 feet of seawater (fsw), which was clearly before the apparent surface aspiration. Three of the eight patients had histories of hypertension, and four reported histories suggestive of asthma, which points to a possible role for these conditions. Six of the eight divers had prior diving experience, one was a new diver, and for one experience was not documented. Interestingly, three of the patients reported histories of similar episodes on previous scuba dives. One diver (case 1) had 20 years of diving experience, had suffered a similar episode 1 week prior, and subsequently resumed diving. One diver (case 4) also had prior diving experience. One diver (case 6) was a relatively new diver and resumed scuba following this episode. The onset of symptoms occurred while at depth, during ascent, or shortly after surfacing. Pulmonary edema occurred in water as shallow as 15 fsw (4.6 m of sea water [msw]), and as deep as 110 fsw (34 msw), with an average of 54 fsw (17 msw). Depth was not reported for one diver. There was a variable time of onset as well. In five of the divers, the onset of symptoms occurred during the first dive of the day. None of the divers were current cigarette smokers, although two had a history of tobacco use. The results of each patient’s initial physical examination were consistent with the clinical presentation of pulmonary edema; only one diver (case 4) presented initially with hypotension. Chest radiographic findings ranged from interstitial edema to diffuse, bilateral alveolar densities, which are characteristic of the radiographic findings of early and late pulmonary edema, respectively. One diver (case 8) had chest radiographic findings that were consistent with cardiogenic pulmonary edema, including heart size at the upper limits of normal (Fig 1) and cough Figure 1. Chest radiograph showing acute pulmonary edema in one diver (case 8). A mild perivascular infiltrate is suspected at the lung bases. Upper lobe vessels are prominent. productive of copious, clear yellow sputum. He had a (known) 1-year history of treated chronic atrial fibrillation. Six of the eight patients had hemoptysis, suggesting the presence of permeability pulmonary edema caused by disruption of the entire blood-gas barrier. One diver (case 6) was physically fit and was severely dyspneic following her dive. The results of her cardiac workup were negative. Her chest radiographic findings (Fig 2) demonstrated an unusual and “patchy” distribution (which is consistent with the known anatomic distribution of vascular smooth muscle in the lungs) that also can occur in patients with HAPE. Echocardiograms were performed or were available in only two patients. Neither patient showed 1688 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21969/ on 04/29/2017 Reviews Pulmonary Edema Figure 2. Chest radiograph showing acute pulmonary edema in one diver (case 6). Primarily, upper lobe distribution involves at least the left upper lobe, and probably bilateral upper lobes. This focal, patchy distribution is unusual. These finding suggest a permeability pulmonary edema. These findings, a normal heart size and infrequent interstitial edema or pleural effusion, suggest a microvascular permeability pulmonary edema. any ventricular or valvular abnormalities. In the four patients with documented initial room air arterial blood gas measurements, the results for each patient indicated metabolic acidosis (pH range, 7.13 to 7.33) with eucapnia (Paco2 range, 31 to 46 mm Hg). The development of pulmonary edema represents a pathophysiologic spectrum. On one end of this spectrum is the pure cardiogenic origin of pulmonary edema (as in congestive heart failure) due to increased pulmonary capillary hydrostatic pressure that produces edema fluid with a relatively low protein content. At the other end is a more severe, noncardiogenic form caused by increased capillary permeability, as in patients with ARDS. In patients with ARDS, the edema arises from lung cell injury rather than from increased hydrostatic filtration pressures and, thus, is considered to be noncardiogenic, at least during the initial clinical phase. Inflammation is a principal contributing factor in acute lung injury in patients with ARDS and is associated with inflammatory mediators such as tumor necrosis factor and interleukins.9 It has been well documented that chemicals and a variety of other factors can cause the alveolar-capillary leak syndrome that, potentially, can lead to acute pulmonary edema.10 Stimulant-associated pulmonary edema can result either from direct local cellular toxic reactions or microvascular pulmonary effects.11 Overdoses from diphenhydramine and cocaine abuse may have common mechanisms that are different from heroin-related pulmonary edema.12 Mechanisms have been proposed to explain the patterns of lung reaction and lung leakage that result from exposure to cigarette smoke and other particles.13 None of the eight patients in this study were current smokers. Stress failure of the pulmonary capillaries occurs in several pathologic conditions and likely plays a major role in the development of pulmonary edema in scuba divers and swimmers. The blood-gas barrier must be extremely thin to allow for the diffusion of oxygen and carbon dioxide but must maintain structural integrity under the most challenging physiologic conditions. The thin portion of this barrier is formed by the capillary endothelium, alveolar epithelium, and the extracellular matrix (ECM). The ECM consists of the fused basement membranes of the two cellular layers and confers most of the barrier strength.7,14 As capillary pressure increases, “pore stretching” of the capillary endothelial cell may occur, leading to larger tracer molecules such as hemoglobin moving into the interstitium of the alveolar wall.7 Finally, at even higher pressures, stress failure of the blood-gas barrier occurs, resulting in a high-permeability type of edema. The resultant edema fluid is characterized by a protein content approaching that of blood, due to the loss of the sieving properties of the microvascular barrier.15 Scanning electron microscopy16 and transmission CHEST / 120 / 5 / NOVEMBER, 2001 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21969/ on 04/29/2017 1689 electron microscopy17 studies have demonstrated alveolar epithelial breaks as capillary transmural pressure is raised (Fig 3). Alveolar epithelial cell active sodium transport is the primary mechanism regulating the removal of excess alveolar fluid from the distal airspaces.18 The impairment of this function (as seen in cold conditions) could contribute to the development of pulmonary edema.19 Rapid changes in gene expression for ECM proteins and growth factors occur in response to increases in capillary wall stress.20 The patchy nature of stress failure is consistent with anatomic findings of the patchy distribution of smooth muscle in small pulmonary arteries in the healthy adult lung21 and the observation of uneven vasoconstriction that occurs when the pulmonary arterial pressure rises in patients with HAPE.22 In patients with ARDS, the concept that alveolar damage is always a diffuse bilateral process is not consistent with clinical or morphologic data. Even in patients who die of respiratory failure secondary to ARDS, although the lung is (usually) extensively involved, focal areas may be inexplicably spared.23 The chest radiographic findings shown in Figure 2 indicate an unusual distribution of pulmonary edema that is consistent with focal lung involvement. Immersion Effects Immersion causes the central pooling of blood by facilitation of the venous return, which increases the preload. This physical shift of blood centrally during immersion is further aided by the high density of water, which diminishes or eliminates the usual pooling of blood in the peripheral veins that occurs in air (in this respect, immersion is analogous to a gravity-free state).24 Blood redistribution during immersion in thermoneutral water (ie, 91.4 to 95°F) and in cool water corresponds to a reduction in vital Figure 3. Scanning electron micrographs showing disruptions of the blood-gas barrier in rabbit lungs perfused in situ to high capillary transmural pressures of 52.5 cm H2O (top left, a, top right, b, and bottom left, c) and 72.5 cm H2O (bottom right, d). Top left, a: a circular disruption of the epithelial layer (open arrow) and complete ruptures of the blood-gas barrier (closed arrows) are shown. Top right, b: a break involving the whole blood-gas barrier (closed arrow) at about 2.1 m from an intercellular junction (white arrow) is shown. Bottom left, c: complete ruptures of the blood-gas barrier (closed arrows) with a flap of endothelium (open arrow) partly covering one break are shown. Bottom right, d: a slit of the blood-gas barrier (closed arrow) very close (about 0.4 m) to an intercellular junction (white arrow) is shown. Almost no breaks occurred at intercellular junctions, although many were seen within 1 m of the junctions. This suggests a considerable mechanical strength of the junctions, but one that is so rigid that the cell in the vicinity of the junction is more vulnerable to mechanical failure. Scale bars ⫽ 2 m (top right, b, and bottom left, c) and 3 m (top left, a, and bottom right, d). Reprinted by permission of West et al.17 1690 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21969/ on 04/29/2017 Reviews capacity of 5% and 10%, respectively.25 The smaller change in vital capacity that occurred in warm water indicates a significant amount of peripheral pooling persisted. For scuba divers, water is generally considered to be cold at temperatures ⬍ 77°F, and much of the surface water in the United States is below 70°F.26 In our patients, the recorded water temperatures ranged from 50°F to the mid-80s°F. At these temperatures, peripheral vasoconstriction in the water would be expected, bringing about a further increase in the central blood volume at the expense of the peripheral volume.26 Pulmonary edema associated with immersion previously has been described in 11 divers and swimmers exposed to cold water.2 Cardiac preload and afterload augmentation due to cold-induced vasoconstriction combined with immersion effects was thought to cause the pulmonary edema.2,14 Several case reports5,27–29 have associated cold exposure during swimming, scuba diving, or immersion with the onset of pulmonary edema. Rapid rewarming after prolonged hypothermia may cause vasomotor collapse, leading to acute pulmonary edema.30 Significant increases in pulmonary artery pressures due to short-term cold exposure in rats also have been demonstrated.31 In divers and swimmers, the physiologic response to cold water, combined with the centralization of blood due to immersion effects, may promote the development of pulmonary edema. Negative-Pressure Effects Clinically silent negative-pressure pulmonary edema as a consequence of acute airway obstruction or vigorous attempts to breathe against a high resistance to flow has been described.32,33 Factors that could contribute to pulmonary edema in scuba divers include scuba valve failure (rare), low tank air pressure with certain types of regulators, a tank not turned completely on, the use of a breathing apparatus with a high inspiratory resistance, and panic associated with an increased effort of breathing so that inspiratory pressure was slightly negative with respect to water pressure.34 Filling compressed air scuba tanks in locales such as the island of Hawaii with air containing volcanic dust has resulted in regulator malfunction. Relatively negative intrathoracic pressures can result from decreased lung volumes due to chest constriction as when the diver wears a tight wet suit. Central bronchial diameter varies with lung volume (M. Knafels; personal communication; July 1998), leading to increased resistance to breathing as the total lung volume decreases during a dive exposure. Resistance to breathing also is increased due to greater gas density leading to turbulent flow and an increase in the breathing apparatus internal impedance has been postulated.35 In swimmers, there is a potential to increase pulmonary capillary pressures due to negative-pressure breathing as alveolar pressure decreases below mouth pressure. Direct measurements during head-out immersion have shown a 65% increase in respiratory work associated with immersion to the xiphoid when compared with immersion to the neck under resting conditions.36 This could contribute to pulmonary edema in swimmers. Neurogenic Pulmonary Edema Pulmonary edema develops in several clinical conditions that have both cardiogenic and noncardiogenic (permeability) components. Although the pathogenesis of nervous system-induced pulmonary edema remains incompletely understood, the two major mechanisms are elevated intravascular pressure and pulmonary capillary leak. Intracranial hypertension causes a massive centrally mediated sympathetic discharge, which increases systemic and pulmonary vascular resistance and leads to high transmural pressures. The hemodynamic component is relatively brief and may unmask a pure noncardiogenic pulmonary edema.37 A report38 of pulmonary edema in association with surgical resection of a brain tumor suggests the medulla oblongata as an important anatomic site of origin for neurogenic pulmonary edema in humans. The importance of these mechanisms in our divers is unknown. HAPE Although not directly relevant to divers and swimmers, a discussion of HAPE may help to clarify the pathophysiology of pulmonary edema. HAPE is associated with high pulmonary arterial pressures, normal wedge pressures, and reduced barrier function of the pulmonary vascular wall. HAPE-prone mountaineers had significant (p ⬍ 0.01) elevations of plasma endothelin-1 levels compared to HAPEresistant control subjects. This potent pulmonary vasoconstrictor peptide causes an exaggerated pulmonary hypertension at high altitude and also augments microvascular permeability.39 Primary intracranial events elevate peripheral sympathetic activity that acts neurogenically in the lung to cause pulmonary edema and in the kidney to promote salt and water retention. Striking increases of aldosterone, vasopressin, and atrial natriuretic peptide40 likely modulate the adrenergic responses. The edema fluid CHEST / 120 / 5 / NOVEMBER, 2001 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21969/ on 04/29/2017 1691 that is produced in HAPE patients is the highpermeability type, with large concentrations of primarily alveolar macrophages and high-molecularweight proteins.41 In HAPE-prone individuals, urinary leukotriene E4 levels are elevated,42 and levels of BAL fluid cytokines (including interleukin-6 and tumor necrosis factor-␣) are markedly elevated,43 suggesting that inflammatory mechanisms play a major role in HAPE. HAPE has been associated with the major histocompatibility complex, which suggests immunogenetic mediation.44 The responses of HAPE-susceptible individuals to exercise include lower diffusing capacities of the lung for carbon monoxide, smaller functional residual capacities, and smaller increases in stroke volumes compared to HAPE-resistant subjects.45 Since HAPE tends to occur subacutely, the mechanisms involved may be more complex than for scuba divers and swimmers. Peak Exercise and Pulmonary Edema There have been several published case reports46 –50 of pulmonary edema in athletes during peak exercise and during bicycle ergometry,51 and it is well-known to occur in racehorses.52,53 Increased cardiac output during exercise rarely would be expected to raise pulmonary capillary pressure to the point of microvascular rupture in humans. However, combined with the pulmonary mechanics of effort associated with extreme exertion, capillary tolerance could be exceeded. A role for the activation of proinflammatory pathways associated with the development of pulmonary edema in patients under conditions of peak exertion has been proposed.50 An Israeli group reported3 on the development of dyspnea and pulmonary hemorrhages in 8 of 30 healthy young men engaged in an elite military fitness training program involving a 2.4-km open-sea swimming time trial. All eight young men developed shortness of breath within 45 min and prematurely terminated their swim. The conditions of all eight men resolved with treatment. Two men had recurrent episodes of pulmonary edema, hemoptysis, or both during subsequent swimming.3 Pulmonary Barotrauma Breath-hold diving has been reported to result in intra-alveolar hemorrhaging54 and death from diffuse bilateral pulmonary vascular injury.6 Pulmonary barotrauma due to lung overinflation usually is associated with a rapid or uncontrolled ascent while breathing from a compressed air source and can lead to air embolism.55 This serious condition may be second only to drowning as a cause of death among recreational scuba divers. Neither condition seems to play a role in our cases. Conclusion There are ⬎ 3 million scuba divers in the United States alone. Physicians will increasingly be asked to evaluate and treat scuba diving-related problems and to assess individuals for fitness to dive. Factors potentially contributing to the development of pulmonary edema in the diver or swimmer include poor physical condition, underlying cardiovascular dysfunction, hypertension, asthma, anxiety, and strenuous exertion before, during, or after diving. External factors contributing to the development of pulmonary edema include thermal exposure, the effects of tight wet suit wear, exposure to respiratory irritants in the compressed air source, increased work of (or resistance to) breathing due to low air pressure in the scuba tank, aspiration, particulates in the air supply, and malfunction or poor state of repair of the regulator. The quantity of pulmonary edema fluid formed in divers is presumably augmented by the centralization of blood flow from immersion and cold-exposure effects. Massive pulmonary edema significantly decreases pulmonary compliance, leading rapidly to hypoxemia and acidosis. This mechanical pulmonary failure is of sufficient scope to diminish the victim’s ability to compensate with hyperventilation, leading to the uncharacteristic arterial blood gas picture of acidosis and hypoxemia with eucapnia or hypercapnia. The onset of pulmonary edema in divers is a rapid, acute process that is usually due to patchy, focal disruption of portions or the entire thickness of the blood-gas barrier in discrete areas of the lungs, which is similar to the edema found in patients experiencing cocaine overdoses. Rapid clearing of the pulmonary edema and metabolic acidosis is expected in these patients. Bloodgas barrier disruptions are known to quickly resolve in experimental conditions after the reduction of the elevated pulmonary venous pressure. Rapid improvement is similarly seen in patients experiencing HAPE when they are taken to a lower altitude (higher oxygen partial pressure). During the healing phases, pulmonary blood flow is preferentially shunted to functional alveoli. This flow redistribution allows for rapid clinical recovery while healing of the injured focal areas occurs. All patients in this report had complete resolutions of the signs and symptoms of pulmonary edema with treatment. For divers or swimmers who experience pulmonary edema, a generic recommendation to avoid 1692 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21969/ on 04/29/2017 Reviews future exposures seems unwarranted. Many of these swimmers and divers have not suffered any recurrences on subsequent diving or swimming activities. Of the three patients in this report who were questioned (two of whom had previously experienced pulmonary edema while scuba diving), all have returned to diving with no further problems. However, all of those patients adopted more conservative diving habits. Unfortunately, there is currently no accurate way to predict whether or not a scuba diver is at risk to develop acute pulmonary edema. In those divers who have experienced a prior episode, a complete history should be obtained in an attempt to identify potential triggers that might be eliminated. Extreme conditions in future scuba dives or swimming exposures should be avoided. Health-care providers involved in the management of these patients should ask specifically about possible contributing factors. Certainly, divers with pulmonary complaints prior to entering the water should refrain from diving and should receive medical evaluations or advice before attempting to dive. Although impractical for the vast majority of divers, tests that may be of value in evaluating problems during scuba diving would include high-resolution, thin-section CT scanning, measurement of the diffusing capacity of the lung for carbon monoxide, and serial pulmonary function tests. There is still much to be learned about this rare, but potentially fatal (autopsy results from the Divers Alert Network case files of an experienced female diver were consistent with pulmonary edema and showed no significant cardiac abnormalities), complication of scuba diving. ACKNOWLEDGMENTS: We acknowledge the assistance of John B. West, MD, PhD, Claude A. Piantadosi, MD, and Anthony Woolf, MD, for their thorough reviews of the manuscript and invaluable suggestions. We also thank James L. Caruso, MD, for his assistance in providing case information from the Divers Alert Network files. References 1 Hampson NB, Dunford RG. Pulmonary edema of scuba divers. Undersea Hyperb Med 1997; 24:29 –33 2 Wilmhurst PT, Nuri M, Crowther A, et al. Cold-induced pulmonary oedema in scuba divers and swimmers, subsequent development of hypertension. Lancet 1989; 1:62– 65 3 Weiler-Ravell D, Shupak A, Goldenberg I, et al. Pulmonary oedema and hemoptysis induced by strenuous swimming. BMJ 1995; 311:361–362 4 Pons M, Blickenstorfer D, Oechslin E, et al. Pulmonary oedema in healthy persons during scuba-diving and swimming. Eur Respir J 1995; 8:762–767 5 Roeggla MG, Roeggla G, Seidler K, et al. Self-limiting pulmonary edema with alveolar hemorrhage during diving in cold water [letter]. Am J Emerg Med 1996; 14:333 6 Strauss MB, Wright PW. Thoracic squeeze diving casualty. Aerosp Med 1971; 42:673– 675 7 West JB, Mathieu-Costello O. Vulnerability of pulmonary capillaries in heart disease. Circulation 1995; 92:622– 631 8 Avery WG, Samet P, Sackner MA. The acidosis of pulmonary edema. Am J Med 1970; 48:320 –324 9 Rinaldo JE. The adult respiratory distress syndrome. In: Tierney DF, ed. Current pulmonology (vol 15). St Louis, MO: Mosby, 1994; 137–156 10 Nakamura T, Nakagawa M. Alveolar capillary leak syndrome. Ryoikibetsu Shokogun Shirizu 1986; 3:705–706 11 Albertson TE, Walby WF, Derlet RW. Stimulant-induced pulmonary toxicity. Chest 1995; 108:1140 –1149 12 Karch SB. Diphenhydramine toxicity: comparisons of postmortem findings in diphenhydramine-, cocaine-, and heroinrelated deaths. Am J Forensic Med Pathol 1998; 19:143–147 13 Kilburn KH. Particles causing lung disease. Environ Health Perspect 1984; 55:97–109 14 West JB, Mathieu-Costello O. Stress failure of pulmonary capillaries: role in lung and heart disease. Lancet 1992; 340:762–767 15 Tsukimoto KL, Mathieu-Costello O, West JB, et al. Ultrastructural appearances of pulmonary capillaries at high transmural pressures. J Appl Physiol 1991; 71:573–582 16 Costello ML, Mathieu-Costello O, West JB. Stress failure of alveolar epithelial cells studied by scanning electron microscopy. Am Rev Respir Dis 1992; 145:1446 –1455 17 West JB, Tsukimoto K, Mathieu-Costello O, et al,. Stress failure in pulmonary capillaries. J Appl Physiol 1991; 70: 1731–1742 18 Matthay MA. Function of the alveolar epithelial barrier under pathologic conditions. Chest 1994; 105(suppl):67S–74S 19 Kambara K, Jerome EH, Serihov VB, et al. Reliability of extravascular lung thermal volume measurements by thermal conductivity techniques in sheep. J Appl Physiol 1992; 73: 1449 –1456 20 West JB, Mathieu-Costello O. Structure, strength, failure, and remodeling of the pulmonary blood-gas barrier. Annu Rev Physiol 1999; 61:543–572 21 Reid L. The pulmonary circulation: remodeling in growth and disease. Am Rev Respir Dis 1979; 119:531–546 22 Viswanathan RS, Subramanian S, Lodi ST, et al. Further studies on pulmonary oedema at high altitude. Respiration 1978; 36:216 –222 23 Tomashefski JF. Pulmonary pathology of ARDS. Clin Chest Med 1990; 11:593– 619 24 Hong SK. Breath-hold diving. In: Bove AA, ed. Bove and Davis’ diving medicine. 3rd ed. Philadelphia, PA: Saunders, 1997; 65–74 25 Lundgren CE, Pasche AJ. Physiology of diving: immersion effects. In: Shilling CW, Carlston CB, Mathias RA, eds. The physician’s guide to diving medicine. New York, NY: Plenum Press, 1984; 86 –98 26 Mebane GY Hypothermia. In: Bove AA, ed. Bove and Davis’ diving medicine. 3rd ed. Philadelphia, PA: Saunders, 1997; 207–215 27 O’Keeffe KM. Non-cardiogenic pulmonary edema from accidental hypothermia: a case report. Colo Med 1980; 77:106 – 107 28 Morales CF, Strollo PJ. Noncardiogenic pulmonary edema associated with accidental hypothermia. Chest 1993; 103: 971–973 29 Cosgrove H, Guly H. Acute shortness of breath: an unusual cause. J Accid Emerg Med 1996; 13:356 –357 30 Lloyd EL. Treatment after exposure to cold. Lancet 1972; 1:491– 492 31 Kashimura O. Effects of acute exposure to cold on pulmonary arterial blood pressure in awake rats. Nippon Eiseigaku Zasshi 1993; 48:859 – 863 32 Brown RE. Negative pressure pulmonary edema. In: Berry CHEST / 120 / 5 / NOVEMBER, 2001 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21969/ on 04/29/2017 1693 33 34 35 36 37 38 39 40 41 42 43 44 FA, ed. Anesthetic management of difficult and routine pediatric patients. New York, NY: Churchill Livingstone, 1986; 169 –178 Frank LP, Schreiber GC. Pulmonary edema following acute upper airway obstruction [letter]. Anesthesiology 1986; 65: 106 National Oceanic and Atmospheric Administration. Diving manual: diving for science and technology. Washington, DC: US Government Printing Office, 1991 Chung DF, Keyes SJ, Morgan BM, et al. Mechanisms of airway narrowing in acute pulmonary oedema in dogs: influence of the vagus and lung volume. Clin Sci (Colch) 1983; 65:289 –296 Hong SK, Cerretelli P, Cruz J, et al. Mechanics of respiration during submersion in water. J Appl Physiol 1969; 38:449 – 454 Simon RP. Neurogenic pulmonary edema. Neurol Clin 1993; 11:309 –323 Keegan MT, Lanier WL. Pulmonary edema after resection of a fourth ventricle tumor: possible evidence for a medullamediated mechanism. Mayo Clin Proc 1999; 74:264 –268 Sartori CL, Vollenweider L, Scherrer U. Exaggerated endothelin release in high-altitude pulmonary edema. Circulation 1999; 99:2665–2668 Krasney JA. A neurogenic basis for acute altitude illness. Med Sci Sports Exerc 1994; 26:195–208 Schoene RB. Pulmonary edema at high altitude: review, pathophysiology, and update. Clin Chest Med 1985; 6:491– 507 Kaminsky DA, Jones K, Schoene RB, et al. Urinary leukotriene E4 levels in high-altitude pulmonary edema: a possible role for inflammation. Chest 1996; 110:939 –945 Kubo K, Hanaoka M, Hayano T, et al. Inflammatory cytokines in BAL fluid and pulmonary hemodynamics in highaltitude pulmonary edema. Respir Physiol 1998; 111:301–310 Hanaoka MK, Kubo K, Yamazaki Y, et al. Association of high-altitude pulmonary edema with the major histocompat- ibility complex. Circulation 1998; 97:1124 –1128 45 Steinacker JM, Tobias P, Menold E, et al. Lung diffusing capacity and exercise in subjects with previous high altitude pulmonary oedema. Eur Respir J 1998; 11:643– 650 46 Rasmussen BS, Elkjaer P, Juhl B. Impaired pulmonary and cardiac function after maximal exercise. J Sports Sci 1988; 6:219 –228 47 MacKechnie JK, Leary WP, Noakes TK, et al. Acute pulmonary oedema in two athletes during a 90-km running race. S Afr Med J 1979; 56:261–265 48 Noakes TD, Goodwin N, Rayner BL, et al. Water intoxication: a possible complication during endurance exercise. Med Sci Sports Exerc 1985; 17:370 –375 49 Young MF, Sciurba F, Rinaldo J. Delirium and pulmonary edema after completing a marathon. Am Rev Respir Dis 1987; 136:737–739 50 Hopkins SR, Schoene RB, West JB, et al. Intense exercise impairs the integrity of the pulmonary blood-gas barrier in elite athletes. Am J Respir Crit Care Med 1997; 155:1019 – 1094 51 Kaltenbach MD, Scherer D, Dowinsky S. Complications of exercise testing: a survey in three German speaking countries. Eur Heart J 1982; 3:199 –202 52 O’Callaghan MW, Pascoe JR, Tyler WS, et al. Exerciseinduced pulmonary haemorrhage in the horse: results of a detailed clinical, postmorten and imaging study. IV. Conclusions and implications. Equine Vet J 1987; 19:428 – 434 53 Whitehall KE, Greet TR. Collection and evaluation of tracheobronchial washes in the horse. Equine Vet J 1984; 16:499 –508 54 Boussuges A, Succo E, Bergmann E, et al. Intra-alveolar hemorrhage: an uncommon accident in a breath holding diver. Presse Med 1995; 24:1169 –1170 55 Neuman TS. Pulmonary barotraumas. In: Bove AA, ed. Bove and Davis’ diving medicine. 3rd ed. Philadelphia, PA: Saunders, 1997: 176 –183 1694 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21969/ on 04/29/2017 Reviews