Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
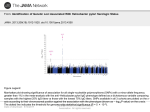
Welcome to the ‘What’s driving Parkinson’s disease?’ research programme Institute Institute of of Pharmaceutical Pharmaceutical Science Science driving What’s Parkinson’s disease? Contents 1. Quantifying the syndrome _________________________________________________________________________________________ Hegemony of the global clinical score 5 Profiling phenotype 6 2. Indicative models for the aetiopathogenesis _________________________________________________________________________________________ Model 1: Laxatives associated with improvement in rigidity, antimicrobials with worsening 8 Model 2: Hypokinesia improves with Helicobacter pylori eradication 9 Model 3: Classical spousal approach to environmental causality – Is it transmissible? 10 Model 4: Circulating leukocyte subtypes as mediators 11 Model 5: Circulating immune-inflammatory markers 12 Model 6: Changes in duodenal enterocytes may flag clinical evolution 13 Model 7: Other Helicobacter species – a zoonosis? 14 Model 8: Underlying viral infection? 15 3. Key established collaboration _________________________________________________________________________________________ King’s College London Centre for Host Microbiome Interaction with INRA Metagenopolis, Paris – microbial metagenomics 17 Institute of Pharmaceutical Science– metabolomics 18 For mini-review with original references see:Dobbs SM, Dobbs RJ, Weller C, Charlett A, Augustin A, Taylor D, Ibrahim MA, Bjarnason I. Peripheral aetiopathogenic drivers and mediators of Parkinson's disease and co-morbidities: role of gastrointestinal microbiota. J Neurovirol 2015; (Epub ahead of print) doi 10.1007/s13365-015-0357-8. 1. Quantifying the syndrome Hegemony of the global clinical score I n Parkinson’s disease (PD), the global score holds sway, but is a blunt instrument. Simple relevant tests of performance are advocated, but often with inadequate attention to their sensitivity, specificity and reliability. The time to walk an individually set distance, return to and sit in a chair, and the rate of progress at fastening a set of buttons are reliable, but lack sensitivity to dopaminergic effects. In contrast, our use of gait analysis at free walking speed has excellent reliability, usefully discriminates for PD and defines effects of time and intervention. Dichotomous classification of PD is misconceived. Normality often seems to drift into abnormality and, moreover, PD belongs to a group of conditions with overlapping phenotypes. Aetiological clues lying in pre-presentation and overlap states are obscured by nosological divisions imposed by man. Continuous physical and cognitive measures are needed, cross-referenced to the usual clinical presentation threshold. Defining phenotype by objective quantification of its facets allows for the possibility of disease facets having different, non-coincident, driving forces. The aim is a description of the phenotype in terms of the minimum number of complementary measures. Under our test conditions, measures of three cardinal signs of PD, brady/hypokinesia, rigidity and tremor, are independent and complementary, but a forth, postural abnormality, is highly dependent on brady/hypokinesia and rigidity. (Adjustment is made for pre-determined demographic / anthropometric characteristics.) Tremor seated Tremor stance/ walk Foot separat’n Cognitive efficiency Mean stride length Simian posture Defining phenotype by objective quantification allows for facets having different, noncoincident, driving forces, and dichotomous classification being misconceived Extensor rigidity Mean arterial pressure Free walking speed Flexor rigidity Reaction time Sway Illustration of between-patient relationships of measures of disease facets. Facets are represented by discs, single variable associations by lines ending at corresponding disc perimeters. The closer the discs, the closer the association. Absence of connecting lines means lack of association. 5 Profiling phenotype Our emphasis has shifted from objective monitoring of drug efficacy to exploring what lies behind the unexplained variability in those objective measures Gait traces obtained ½ and 2½ h after a levodopa combination formulation (Cover image). Amplitude of waveform (AB, BC, CD) represents stride length, flattened peaks and troughs hesitancy between strides. Lower trace gives foot separation at mid-swing (x, y, z): the patient was walking with a dangerously narrow base before medication took effect. Monitoring of flexor and extensor rigidity monitoring in a PD patient over 8 years. In general, despite clinical optimisation of long half-life antiparkinsonian treatment, withinand between-subject variation in objectively measured rigidity remains considerable 6 I vention, design and development of equipment is bespoke. Devices are inexpensive, do not require a specialist operator and are useable in a clinical (even domestic) context. Wherever possible, equipment is small and unobtrusive. Output is designed to be readily interpreted by the nonspecialist and fed back to the patient. Targets for objective assessment are the cardinal signs, major associated disability (e.g. cognitive inefficiency, inability to turn in bed) and events (falls, sleep apnoea,). A secondary, but important, consideration is commercialization to bring precise, objective measurement to routine practice. Every physiotherapist should have a ‘pocket gait analysis laboratory’: it should be a tool of the trade. The team of senior researcher Dr Clive Weller, with post-doctoral research associate Dr Luc Maréchal, brings together expertise in real time and storage telemetry, computer interfacing and deployment of recent advances in microcontrollers and nanoelectromechanical systems. It is enhanced by mutually beneficial technical and academic collaboration with Professor Kasper Althoefer and Dr Trish Nanayakkara, Robotics within Department of Informatics at KCL. 2. Indicative models for aetiopathogenesis Model 1: Laxatives associated with improvement in rigidity, antimicrobials with worsening. There is indicative evidence of a continuing role of gastrointestinal dysbiosis in pathogenesis. G astrointestinal transit is slowed in PD. We showed that constipation pre-dates the diagnosis by, on average, 3 decades: a finding upheld prospectively by the association of infrequent bowel movements and subsequent diagnosis of PD. Constipation markedly affects quality-of-life in PD. Aggregates of misfolded protein characteristic of PD, known historically as Lewy bodies, are found in the enteric nervous system (the little brain), related sympathetic ganglia, and the parasympathetic vagal nuclei in the brain stem. There is loss of dopaminergic neurons in the little brain as well as the basal ganglia. Our work shows that the flexor-rigidity of PD increases by a clinicallysignificant amount year-on-year before prescribing maintenance laxatives, plateauing after. A similar pattern is seen with bulk, osmotic and enterokinetic laxatives, pointing to a common mechanism of action on rigidity. Moreover, a guanylate cylase-C receptor agonist (linaclotide), which increases gastrointestinal-secretion, is associated with a large step-down in rigidity. In contrast, rigidity worsens cumulatively with successive antimicrobial interventions, irrespective of indication, and over and above the effect of time. This suggests that a pathological dysbiosis resulting from a first course does not recover and is exacerbated by future exposures. Time trends (95% confidence interval) in flexor rigidity in relation to initiation of laxative classes. Based on 1493 measurements in 79 PD patients. Cumulative percentage increase in flexor rigidity over baseline following a first, second and third antimicrobial course. Based on 396 assessments in 49 PD patients 8 Model 2: Hypokinesia improves with Helicobacter pylori eradication. hat peptic ulceration is prodromal paved the way to exploring Helicobacter pylori as a driver in PD. In our randomised placebo-controlled trial, biopsy-proven H. pylori eradication reduced hypokinesia of gait in PD. A longitudinal observational study showed indication specificity, in that antimicrobials for other indications did not improve hypokinesia. In the trial, while hypokinesia improved, rigidity worsened over the year post-eradication, both plateauing over the next. There was overall clinical benefit. Improved hypokinesia was independent of any antiparkinsonian medication. (Receipt of levodopa an exclusion.) Increased rigidity may flag acquisition of small-intestinal-bacterial-overgrowth, since H. pylori and hydrogen-breath-test-positivity for overgrowth are inversely related in PD. In no disease where H. pylori is causal is it present in all cases. However, current or past Helicobacter infection may be a necessary though not sufficient player in developing the full PD syndrome. There is a lack of birth cohort effect for H. pylori in PD, as in gastric cancer and peptic ulcer where causal links with H. pylori are generally accepted. Danish population registers show increased prescription of anti-Helicobacter drugs in the 5 years prior to PD diagnosis. Dopaminergic agonists can prevent duodenal ulcer relapse in man, but whether by suppressing H. pylori is unknown. T Helicobacter pylori in PD may not be a sine qua non, is definitely not sufficient, but is important. Schematic representation of effect of H. pylori eradication on hypokinesia & rigidity. Estimated mean time-trends following successful blinded-active (red) and open-active (orange), and placebo (blue). At present, the level of evidence is 1b (Centre for Evidence Based Medicine, Oxford, 2009) since this is the only trial. 9 Model 3: Classical spousal approach to environmental causality – Is it transmissible? PD patients’ spouses show a tendency towards parkinsonism, and share relative lymphopenia, abnormal bowel function and small-intestinalbacterial-overgrowth. I n our case-control study, spouses of PD patients were a short but highly significant ‘distance-down-the-pathway’ with respect to objective measures of PD facets. Marked, multifarious, relevant differences (physiological/psychomotor/ dermatological), between spouses and control couples are difficult to explain by selective mating or learned/reactive behaviour. In a large cohort, patients and spouses were found to have relative lymphopenia (with particular effect on B cells). There is a proportional increase in natural killer cell count in PD patients, in CD4+ in spouses. Half of the patients and a third of spouses have chronic functional bowel abnormality. Like patients, two-thirds of spouses are hydrogen-breath-test-positive for small-intestinal-bacterial-overgrowth. The spousal findings are not directly attributable to H. pylori. Indeed, spouses have a lower frequency of Helicobacter anti-urease IgG enzyme-linked immunosorbent assay seropositivity than either PD patients or controls, as though an acquired dysbiosis had suppressed it. Crude prevalence rate estimates for frank PD in 34 European studies range widely, the estimate lying within the binomial exact 95% CI for our entire spouse cohort in only one study. A prognostic index for parkinsonism based on brady-/hypo-kinesia variables in 104 subjects with PD, 144 without) applied in 20 index controls (C), their spouses (Cs), 20 patients (P) with clinically-definite (treated) PD and their spouses (Ps), cohabiting for half-a-century. Means (95% C.I.) shown. P and C matched for age and gender. P<0.0001 for predicted probability in Ps cf. C + Cs combined. 10 Model 4: Circulating leukocyte subtypes as mediators. A majority of PD patients have small-intestinal-bacterial-overgrowth at presentation, probably a consequence of caeco-ileal reflux. Blood leukocyte subtypes associated with hydrogen-breathtest positivity for overgrowth (higher natural-killer and total CD4+ counts, lower neutrophils) are the same as those associated with PD facets. The higher the natural-killer count, the shorter stride, slower speed and greater flexor-rigidity (adjusted for patient characteristics). Cellular associations held after allowing for potentially confounding effect of hydrogen-breath-test results or Helicobacter status. Indeed, increased brady/hypokinesia was noted with Helicobacter-positivity, over and above that explained by natural-killer count, and of a magnitude equivalent to that of a levodopa challenge. Association of rigidity with a higher natural-killer count is modulated by the total CD4+ count. The CD4+ subset includes regulatory T-cells which inhibit natural-killer effector mechanisms. Tremor is worse with lower neutrophils: this may reflect neutrophil sequestration in the gut. There are biological gradients of facets of PD on blood leukocyte subtype counts Relationship of PD facets to leucocyte subtype counts in 38 patients, untreated or on stable long-t½ PD-medication. Points shown are average per person: all values for a longitudinal outcome used to estimate regression lines. Relationships held on including levodopa-takers. N.B. Effect of natural killer count on stride length and rigidity independent: no association over our test conditions (bottom right). Relationship of rigidity to CD4+ count to flexor-rigidity, after adjustment for natural-killer count. 11 Model 5: Circulating immuno-inflammatory markers. Biological gradients of facets of PD on circulating immunoinflammatory markers W e have described biological gradients of objective measures of facets on two systemic markers of inflammation, serum cortisol and tumour-necrosis-factor-α. Others have subsequently shown gradients of global motor scores on peripheral blood mononuclear cell production of cytokines and expression of nuclear factor κB. We found that serum interleukin-6 increases with age and is elevated in PD by an amount equivalent to 10 years’ ageing. Others have subsequently shown that a higher interleukin-6 concentration is predictive of incident PD. Systemic immuno-inflammatory activation can increase homocysteine production. Hyperhomocysteinemia is found in 43% PD patients. It is partially explained by a lower serum B12 concentration with no complementary effect of folate. (Methyltetraydrofolate acts as a methyl donor, and cobalamin is a co-factor, in detoxifying homocysteine by remethylation to methionine by methionine synthetase.) Hyperhomocysteinemia is not explained by Helicobacter-status (gastric atrophy being uncommon in PD). Small-intestinalbacterial-overgrowth will increase bacterial utilisation of B12 and provokes a systemic immuno-inflammatory response. Indeed, significant numbers of large irregularly-shaped secondary lysosomes in duodenal lining cells accompany overgrowth in PD, signifying that it is not an innocent bystander. Using the western blot profile of IgG antibodies against electrophoreticallyseparated H. pylori antigens, the predicted probability of being labelled as having PD was greatest with cytotoxin-associated-gene-product positivity and vacuolating-toxin negativity, and urease-B negativity. With this H. pylori antibody pattern, the odds for having PD were increased five-fold at age 80 years. The predictive ability was not confined to those with current infection. Association between serum homocysteine and B12 concentrations in PD. Although, no evidence of frank B12 deficiency in PD, more patients than expected had a concentration in the ‘equivocal range’ or below. Increased demand from immunoinflammatory activation may render an ‘equivocal’ concentration pathological. Homocysteine 2 % higher per year post-diagnosis, and not explained by anti-parkinsonian treatment. Electron-micrographs illustrating cloud of irregular lysosomes in a duodenal lining cell (enterocyte) in a PD patient with small-intestinal-bacterial-overgrowth 12 Model 6: Changes in duodenal enterocytes may flag clinical evolution. I n PD, dysfunction of the cell power houses, mitochondria, is described in skeletal muscle and blood platelets, as well as in the basal ganglia. We have found abnormal forms of mitochondria in duodenal lining cells (enterocytes) in PD. Long thin mitochondria, associated with roughendoplasmic-reticulum indicating functionality, were commonly seen, in the presence of small-intestinal-bacterial-overgrowth, absence of recent H. pylori infection. The complex branching seen may result from failure to divide. With current or recent H. pylori infection, arrays encapsulated in a doublemembrane were found in half of cases, lying among normal mitochondria. There is a report of similar “mitochondrial” inclusions in cerebral neurons in Creutzfeldt-Jakob-like-disease. Alternatively, these bodies might be viroplasms not mitochondria. Our electron microscopists had not previously observed similar bodies, but subsequently found examples in archived duodenal biopsies from two patients with human immunodeficiency virus infection. PD is a disease of mitochondrial dysfunction: different mitochondrial dysmorphology in enterocytes characterises putative gastrointestinal drivers Electron-micrographs of duodenal enterocytes from PD patients. Above: long thin mitochondria seen to predominate at low magnification. Complex branching of a mitochondrion is shown at intermediate magnification. Below: double-membraned, encapsulated arrays lie amongst normal mitochondria. Arrays seen longitudinally and in transverse section at higher magnification. 13 Model 7: Other Helicobacter species – a zoonosis? arkinson’s disease has been linked with rural living and farm experience. A study of 6 million death certificates from 26 US states found the proportional mortality from PD was significantly higher in livestock farmers than in non-farmers, but lower in crop farmers. Agrochemicals used in these sectors are different, but transmission of infections from animal hosts (zoonotic) is a more compelling explanation. Zoonotic-transmission of bacteria of the genus Helicobacter is a strong, and potentially remediable, candidate. Species, usually resident in domestic and farm animals, can cause human gastric disease. Several of these ‘spiral’ non-H. pylori Helicobacter species (NHPH) are found in dogs and cats, H. suis (the most common Helicobacter, after H. pylori, to infect humans) in pigs. In our unpublished preliminary survey, H. suis was present in 60 % of 111 UK pig stomachs on microscopic examination, and its DNA detected in stool. As determined by a Ghent University in-house molecular assay for H. suis, its relative frequency compared with H. pylori was 10 times greater in 60 of our PD patients, than in 256 patients from UK gastroenterology-services. Risk of death in PD during follow-up was 8 times greater with H. suis-positivity, compared with those negative. This contrasts with all-cause Kaplan-Meier plot of 19 PD-patients with H. suis mortality being less in those with H. pylori, despite excess DNA detected in gastric biopsy (black line) mortality from gastric cancer. In none of these PD patients compared with 40 without (grey). were spiral Helicobacters seen on histopathology. Little is known, about the epidemiology of zoonotic Helicobacters. They are hard to culture from human gastric biopsy, characteristically patchy and sparse on gastric histopathology, in man, and there is a lack of rigorous molecular diagnostic tests. A validated molecular screening method for NHPH DNA in stool is neeeded. We have described a U-turn in brady/hypokinesia (from wheelchair-bound to being able to walk 3 miles) in a PD-patient, after Spiral Helicobacter in a PD patient associated eradicating a spiral Helicobacter. with chronic antral gastritis The broad brush of epidemiology provides enigmatic aetiopathogenic clues in PD P . Other sources of zoonotic non H. pylori (spiral) gastric Helicobacters 14 Model 8: Underlying viral infection? aecal overload and small-intestinal-bacterial-overgrowth are predisposed to by the slow gastrointestinal transit of PD, and may have detrimental feedback on it, but what initiates that slow transit? Could there be a viral primer? Enteroviruses infect via the gastrointestinal tract and are associated with neurological syndromes. Indeed, there is recent evidence of an enterovirus as a cause of encephalitis lethargica and post-encephalitic parkinsonism. Moreover, in our pilot study using faecal samples taken at start of a diarrhoeal episode, frequency of enterovirus genogroup B RNA appeared high in PD patients and their spouses. A viral primer could also be involved in the relative lymphopenia seen in both PD-patients and their spouses, compared with controls. This robust finding was not explained by anti-parkinsonian medication, Helicobacter-status or breath-hydrogen. A relatively benign retrovirus might explain relative lymphopenia and the slow transit. (Jejunal autonomic denervation is described with human immunodeficiency virus (HIV) infection.) The comparatively high frequency of Dientamoeba fragilis (18 % of PD probands and their spouses cf. 3 % of routine parasitology requests), which we have found in stool, could flag mild acquired-immunodeficiency. The epidemiology of IP and HIV are distinct, but parkinsonism is seen in uncomplicated HIVinfection (as well as with opportunistic infections in acquired immunodeficiency syndrome). Although Lewy bodies are not reported in HIV, motor dysfunction compatible with basal ganglia damage is found early, and basal ganglia dopaminergic cell loss is seen without clinical parkinsonism. In simian immunodeficiency virus-infected monkeys, nigrostriatal dopamine is halved within 2 months. There has been no systematic search for candidate or undiscovered viruses in PD using modern molecular methodology. F A viral primer for slow transit and relative lymphopenia cannot be dismissed. 15 3. Key collaborations King’s College London Centre for Host Microbiome Interaction with INRA Metagenopolis, Paris – microbial metagenomics. G erm-free mice move more and take more risks: they have increased striatal synaptogenesis and dopamine/serotonin turnover. In specific-pathogen-free mice, non-absorbable antimicrobials increase exploratory behaviour and hippocampal brain-derived neurotrophic factor (BDNF). Gavage of caecal contents from a more outgoing mouse strain into a more timid increases both exploratory behaviour and BDNF, and vice versa: these effects were independent of vagal integrity. Specific probiotics cause behavioural change. Important associations between stool bacterial microbiota and human health have been identified. Indeed, there is evidence that stool microbial metagenomics can discriminate better for chronic disease than human genomics. Modifying the GI microbiota may modify disease. Psychiatric illness in irritable bowel syndrome, inflammatory bowel disease and autistic spectrum disorder have been ascribed to dysbiosis. Irritable bowel syndrome with constipation is common in PD. Autism recalls the restricted behaviour of PD. An inflammation-associated form of depression is described. Exhibition of the non-absorbable broad-spectrum antimicrobial, rifaximin, was accompanied by amelioration of hepatic encephalopathy-associated parkinsonism and of characteristic imaging features in globus pallidus in 3 patients with cirrhosis and portosystemic shunting, without change in blood ammonia and electroencephalogram. Two approaches to defining the gut microbiome in PD, using 16S ribosomal RNA gene sequencing (studying 72 patients/72 controls and 38/34, respectively) have been reported, [47, 48] but with no consensus. In the larger of these almost all PD-patients were on anti-parkinsonian medication and there was a high frequency of cerebro- and cardio-vascular co-morbidities and related medications in the controls. Definite characterisation of the microbiome in PD is needed in terms of gene function as well as taxonomically. There is real potential for the collateral benefit of a new generation of animal models, to test cause/effect hypotheses and aid discovery of specifically-targeted, disease-modifying medicines. To date, PD models have relied on surgical, chemical or genetic lesions, and are thus downstream of, or out-with, environmental driving processes. Stanislav Dusko Ehrlich Director Centre for HostMicrobiome Interaction, King’s College London: Research Director Emeritus, Institut National de la Recherche Agronomique, France “One of the most important pioneers in the study of the human microbiome” European Research Council. 17 Institute of Pharmaceutical Science – metabolomics M Peter John Hylands Director Institute of Pharmaceutical Science Professor of Pharmaceutical Chemistry, Pharmaceutical Science Head Department of Pharmacy and Forensic Science “During my tenure, Pharmacy and Pharmacology at King’s College London ranked as 3rd in World (QS ranking, 2014); 91% of our research outputs rated as world-leading/ internationally excellent (Research Excellence Framework, 2014); in unit assessment 3, we ranked 1st in UK for research quality and volume.” 18 etabolomic interest in PD and Alzheimer’s disease has concentrated on markers of damage (e.g. hypoxia, oxidative stress and membrane lipid remodelling) in blood and breath, rather than influence of the metabolome on the disease process. From an aetiopathogenic standpoint, a key question, is whether the metabolome regulates systemic inflammation. In mice, short chain fatty acids, such as butyrate, produced by colonic bacterial fermentation, promote colonic regulatory T-cells (T-reg) which suppress pro-inflammatory cells. This suggests a mechanism for the apparent CD4+ (presumably T-reg component) modulation of rigidity and fits with PD patients’ spouses having a proportional (potentially protective) increase in total CD4+ count. However, whilst oral administration of short chain fatty acids to germ free mice, to address their deficit, increased colonic T-regs, it had no wider effect on mesenteric lymphnode, splenic or thymic T-regs. Human studies have linked fermentation products to behaviour. However, there appears to be contradictory evidence. Faecal propionic acid concentrations have been correlated with anxiety in irritable bowel syndrome (IBS), but those with constipation (IBS-C) have fewer short chain fatty acids producing bacteria in stool but no less anxiety. Mitochondrial dysfunction is described in substantia nigra in PD (complex I) and multiple-system atrophy (complex IV), and in platelets in PD. Hydrogen sulphide is known to inhibit mitochondrial complex IV at higher concentrations. IBS-C patients have more sulfide producers. However, again there is contradictory evidence. In a rodent model of PD, hydrogen sulphide was protective against neurodegeneration, not only by reducing oxidative stress but also by inhibiting neuro-inflammation. This neuroprotection may be predicated on it being a chemically-lesioned model, and/or be dependent on H2S dosage. Others have found that a hydrogen sulphide donor ameliorated naproxeninduced small-intestine enteropathy in rats, and restored naproxen-induced changes in microbiota. In chemically-induced colitis in mice, the donor reduced inflammation, and restored microbial biofilm and deficient mucus production. In vitro, hydrogen sulphide donors promoted formation of biofilms by bacteria derived from human colon. They inhibited potentially damaging planktonic bacteria. As with the microbiome, information relevant to PD is sketchy: our systematic approach to the disease complex is much needed.