Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Psychopharmacology wikipedia , lookup
Psychedelic therapy wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Compounding wikipedia , lookup
Orphan drug wikipedia , lookup
Electronic prescribing wikipedia , lookup
Pharmacognosy wikipedia , lookup
Drug design wikipedia , lookup
Theralizumab wikipedia , lookup
Drug discovery wikipedia , lookup
Neuropharmacology wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacovigilance wikipedia , lookup
Prescription costs wikipedia , lookup
Drug interaction wikipedia , lookup
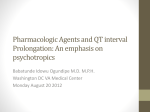
Suspect Moxifloxacin Induced Torsades de Pointes: A case report Ya-Wen * Yang , Hui-Hsiung Lai, Hui-Chuan Lin Department of Pharmacy, Ditmanson Medical Foundation Chia-Yi Christian Hospital Introduction Discussion Torsade de pointes (TdP) is a potentially lifethreatening polymorphic ventricular tachyarrhythmia associated with QT prolongation. Causes of TdP include congenital prolonged QT interval syndromes and acquired diseases, most commonly associated with drug therapy and electrolyte abnormalities. Fluoroquinolones have been reported to prolong the QTc interval and precipitate TdP, but moxifloxacin-induced TdP is still rare. We present a patient with major depressvie disorder who developed TdP during moxifloxacin therapy for pneumonia. Case report A 64-year-old female presented to the emergency department complaining of general weakness and chillness since that morning. Medical history included major depressvie disorder, hypertension and cerebral ischemic disease. Her routine medications were shown at Fig 1. On arrival, T/P/R:38.8/108/18, BP:151/84mmHg. Chest X-ray revealed bilateral infiltrates. Laboratory data showed hyponatremia (Na:116 mmol/L) and hypo-osmolarity (245 mosm/L). Moxifloxacin 400 mg was initiated intravenously for the empirical treatment of pneumonia. Approximately 5 hours later, sudden onset of conscious loss and trismus was noted. EKG showed ventricular tachycardia, then CPCR applied immediately. A diagnosis of TdP was made. She regained spontaneous circulation and was intubated with mechanical ventilator support. Moxifloxacin was discontinued and replaced with amoxicillin/clavulanic acid. Normal saline challenge was also given to correct hyponatremia. Her consciousness was fully recovered and became hemodynamic stable. No further episodes of TdP were noted. Drug Aripiprazole Venlafaxine Zolpidem Lorazepam Flunarizine Fexofenadine Famotidine Dosage 7.5 mg HS 75 mg TID 10 mg HS 1 mg PRHS 10 mg QN 60 mg BID 20 mg BID Fig. 1 Medication record of the patient Start & Stop Date Over 10 years 102, Mar till now 102, Mar till now 102, Mar to 104, Jul 104, Apr to June 104, Apr to June 104, Apr to June Like all fluoroquinolones, moxifloxacin has the potential to prolong the QTc interval, but TdP is very rare. Risk factors of TdP include female sex, advanced age, underlying heart disease, electrolyte imbalance, concomitant drug use that prolongs the QTc interval, severe bradycardia and presence of other diseases. This patient didn’t have previous underlying heart disease, in addition, hyponatremia may not contribute to TdP. But several routine medications have been associated with QTc interval prolongation, including aripiprazole, venlafaxine and famotidine. Concurrent use of these drugs may have additive effects on the QT interval, although there were no episodes of TdP noted before. Therefore, moxifloxacin was assumed to be the predisposing factor for the development of TdP. It also had a strong temporal relationship with the occurrence of TdP. The use of the Naranjo adverse drug reaction probability scale indicated a possible relationship (score of 4) between the TdP observed and moxifloxacin therapy in this patient. Naranjo Algorithm for ADR Causality Assessment Yes No 1. Are there previous conclusive reports of this reaction? 2. Did the adverse event appear after the suspect drug was administered? 3. Did the adverse reaction improve when the drug was discontinued? 4. Did the adverse reaction reappear when the drug was readministered? 5. Are there alternate causes that could have caused the reaction? 6. Did the reaction appear when a placebo was given? 7. Was the drug detected in any body fluid in toxic concentrations? 8. Was the reaction more severe when the dose was increased or less severe when decreased? 9. Did the patient have a similar reaction to the same or similar drugs in any previous exposure? 10. Was the adverse event confirmed by any objective evidence? +1 +2 +1 +2 -1 -1 +1 0 -1 0 -1 +2 +1 0 Don't Know 0 0 0 0 0 0 0 +1 0 0 +1 +1 0 0 0 0 Total score = Conclusion The drugs that have the potential to prolong the QTc interval must be used cautiously in patients with multiple risk factors for TdP. Careful assessment of the risk/benefit ratio is important before prescribing these drugs. Reference 1. N Engl J Med. 2004 Mar 4;350(10):1013-22 2. Cardiol J. 2008;15(1):71-3. 3. Am J Med Sci. 2009 Aug;338(2):164-6 Score +1 +2 +1 0 -1 0 0 0 0 +1 4