Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Antimicrobial resistance wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Epidemiology wikipedia , lookup
Public health genomics wikipedia , lookup
Diseases of poverty wikipedia , lookup
Marburg virus disease wikipedia , lookup
Compartmental models in epidemiology wikipedia , lookup
Focal infection theory wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
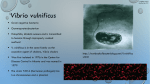
ID Case Conference January 23, 2008 Carlos M. Perez, MD, FACP Associate Professor of Medicine Pontificia Universidad Catolica de Chile The Case • HPI: ♂, 53 yo, Diabetic, otherwise healthy. After returning from a 5 days business trip to El Salvador (San Salvador, capital), developed fever, generalized malaise and severe burning pain on his right upper extremity. He ate at Hotel and nearby “safe” restaurants. No mosquito bites. No contact with animals. No sexual contacts. • PMH: Type 2 Diabetes mellitus insulin dependent. Alcoholic liver disease ? • PSH: Unremarkable • Medications: Insulin NPH. Metformin • NKDA • SH: Married. Etoh abuse. No tobacco use. • ROS: Fever, Malaise, RUE pain and lesions. Physical exam • P: 120 x min. BP: 90/40. T: 37°C, RR: 24 x min. Agitated. • Skin: - R arm: Edema, erythema, tenderness with blue-gray patches and ecchymoses - L forearm: Erythema, edema and bullae - Both legs: Erytema and bullae • HEENT, Lungs, Heart, abdomen unremarkable on admission. Clinical course • Admitted to UCI. Persisted hypotensive despite crystalloids/colloids, noradrenaline/adrenaline infusion. Hemodynamics: PCWP 25 mm Hg. CI: 4.57 L/min/m2. SVR: 494 dyne.sec/cm-5.. Febrile up to 39°C. Antibiotics started: Ceftazidime + ciprofloxacin+ metronidazol+ cloxacilin. One dose Amikacin. Hypoxic requiring mechanical support. Bilateral infiltrates on CXR consistent with ARDS. Anuric (Multiorgan system failure). • Skin lesion progressed rapidly (hours) Laboratory • Hematocrit 42 %, leucocytes 6,700 ( 10 % bands), Platelets: 103.000 60,000 Sed rate 21 mm. CRP 31 (NV 0-0.9). Creatinine 1.6. BUN 28. Na 131. K 3,0. Glucose 318. Bilirubin: 1.45. ALT 277 AST 119. AP 112. CPK 1258 (NV < 195), PT 48 % 26 %. Lactate 6,9 mmol/L (NV < 2,4) Discussion Blood cultures At 7 hours of incubation grew up a Lactose negative Gram negative rod Blood cultures Vibrio vulnificus Clinical course • Family said that patient had consumption of raw oysters in El Salvador. Doxycyclin added after identification of GNR (20 hours after admission). • No improvement despite vasoactive drugs, continuous hemofiltration, respiratory mechanical support, antibiotics. Surgical debridement not possible. Patient died 68 hours after admission. • See Abstract for Poblete R, Andresen M, Perez C et al. Rev Med Chile 2002;130:787-91 Vibrio vulnificus infections • Gram-negative bacterium in the Vibrio family, which can cause serious wound infections and septicemia. • It is the leading cause of shellfish-associated deaths in the United States. Infection due to V. vulnificus is most common in individuals who have chronic, underlying illness, with persons with liver disease or hemochromatosis at greatest risk. Vibrio vulnificus infections • Virulence of V. vulnificus has been associated with the presence of a polysaccharide capsule. • Certain carbotypes of V. vulnificus may be more likely than others to cause human illness. • V. vulnificus contains a lipopolysaccharide (LPS) but, in contrast to Enterobacteriaceae, the LPS of V. vulnificus is not a strong trigger for release of tumor necrosis factor (TNF)-alpha and other shock-related cytokines. Capsular polysaccharide itself may directly trigger some cytokine responses, contributing to the development of the shock syndrome. Vibrio vulnificus infections • Growth of V. vulnificus is dependent in part upon the availability of iron. Growth of the organism in human serum is related directly to the percentage saturation of transferrin with iron. When transferrin iron saturation exceeds 70 percent, growth of the bacterium is nearly exponential. Vibrio vulnificus infections • Epidemiology: As with other members of the species Vibrio, V. vulnificus exists as a free-living bacterium inhabiting estuarine or marine environments. Filter-feeding shellfish, such as oysters, concentrate bacteria.V. vulnificus can be isolated from virtually all oysters harvested in the Chesapeake Bay () and the United States Gulf Coast when water temperatures exceed 20ºC. www.chesakpeakebaysampler.com Vibrio vulnificus infections • Epidemiology: Certain populations are at higher risk for serious infection with V. vulnificus. These include: Alcoholic cirrhosis: 31 to 43 percent Underlying liver disease including cirrhosis (unspecified etiology) and chronic hepatitis: 24 to 31 percent Alcohol abuse without documented liver disease: 12 to 27 percent Hereditary hemochromatosis: 12 percent Chronic diseases such as diabetes mellitus, rheumatoid arthritis, thalassemia major, chronic renal failure, "preleukemia", and lymphoma:7 to 8 percent Vibrio vulnificus infections • Clinical manifestions : Wound infections:V. vulnificus may contaminate wounds exposed to estuarine waters, shellfish, or fish. Typical examples include hand injuries related to opening oysters or leg lacerations related to entering, exiting, or launching boats. The infections are usually mild. However, in high-risk individuals, the infection may spread rapidly, producing severe myositis and fasciitis reminiscent of gas gangrene. Vibrio vulnificus infections • Clinical manifestions : Primary septicemia — Primary V. vulnificus septicemia is associated with ingestion of raw or undercooked shellfish, particularly raw oysters. Patients with primary septicemia generally have underlying liver disease, alcoholism, hereditary hemochromatosis, or a chronic disease. Approximately one-third of patients with primary septicemia present in shock or become hypotensive within 12 hours of hospital admission. Three-fourths of patients have distinctive bullous skin lesions Thrombocytopenia is common, and often there is evidence of DIC. Vibrio vulnificus infections • Mortality rates exceeding 40 percent have been reported in other case series, with a case fatality rate of more than 90 percent among those who become hypotensive Vibrio vulnificus infections • Treatment: In vitro and in vivo studies in mice have demonstrated an apparent synergism between minocycline and cefotaxime in the treatment of serious V. vulnificus infections. Subsequent studies showed comparable survival in mice treated with "newer" quinolones. Recommended: Minocycline or doxycycline (100 mg PO twice daily) plus either cefotaxime (2 gm IV every eight hours) or ceftriaxone (1-2 g IV daily). A reasonable alternative is levofloxacin (500 mg once daily). Vibrio vulnificus infections • Prevention: Persons in high-risk groups should avoid eating raw or undercooked shellfish, particularly oysters. Such persons should also avoid situations in which estuarine-associated wounds are likely to occur. Search PubMed • Vibrio Vulnificus Infection Case Reports Review Differential Diagnosis Drug Therapy Note: In order to see PubMed results, use ViewSlide Show, or hit F5