Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Lyme disease microbiology wikipedia , lookup
Bacterial morphological plasticity wikipedia , lookup
Ascending cholangitis wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Urinary tract infection wikipedia , lookup
History of virology wikipedia , lookup
Globalization and disease wikipedia , lookup
Triclocarban wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Hepatitis C wikipedia , lookup
Infection control wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Neonatal infection wikipedia , lookup
Hepatitis B wikipedia , lookup
Neisseria meningitidis wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Gastroenteritis wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
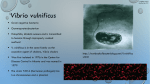
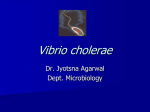
Vibrio Infections Michael Addidle Vibrios Taxonomy Species Genera V. cholerae V. vulnificus Family Vibrios V. parahaemolyticus Vibrionaciae Non-enteric, fermentative, gramnegative rods that are oxidase positive and motile by means of a polar flagella Aeromonas Plesiomonas (amongst others) Vibrios • Most vibrios require saline for growth.(halophilic). However Vibrio cholerae & Vibrio mimicus can survive in both saltwater and freshwater. • Prefer alkaline environments. • Flourish in shallow waters with temperatures greater than 20 degrees. Ie Estuarine environments in the summer. • Survive quite happily in filterfeeding shell fish, such as oysters and pipis. • Greater than 90% of clinical disease due to vibrios in NZ occurs during the summer months. Vibrio cholerae Aetiological agent of cholera Divided into Serogroups on basis of O (somatic antigen) Only serogroups 01 and 0139 are associated with epidemic and pandemic cholera. Often clinically more serious because of production of classical cholera toxin. Vibrio cholerae: bacteriology • Curved gram negative bacillus • Single polar flagellum • Flagellar H antigen and somatic O antigen. • O antigen used to classify V. cholerae into serogroups (01 and 0139 are most well known) • Two biotypes of 01 (classical and El Tor) History of Cholera • “Cholera like illness” described by Hippocrates circa 500 BC • Cholera means “flow of bile” • The Italian doctor Filippo Pacini was the first to discover the cholera bacterium (Vibrio cholerae) in 1854 when cholera hit Florence. • The first recorded cholera pandemic of 1817-1823 spread from India to Southeast Asia, Central Asia, the Middle East and Russia. • 1961-1970s - Seventh pandemic began in Indonesia, called El Tor. Has since spread to many countries. Epidemiology of Vibrio cholerae • • • • • Large infective dose required. Person to person spread uncommon. Most common where poor sanitation and in particular where mass displacement of population has occured Usually acquired through contaminated food or water. Avoidance of unboiled water, ice cubes, food from street vendors, undercooked seafood. To cause infection, organisms must first pass the highly acidic secretions in stomach. (alkaline loving) Infecting dose 10,000,000,000 orgs Therefore people with gastrectomy or on ant- acids are more susceptible. 100-1000 orgs. Incubation period few hours to 5 days. Vibrio cholerae: Pathogenicity • Classical cholera 01/0139 strains usually produce a classical toxin. Non 01/0139 strains usually don’t • Classical Cholera toxin:- Non-invasive, consists of A and B subunits. B subunit facilitates binding and A subunit activates Adenylate Cyclase, leading to increase in cAMP in enterocyte. • cAMP leads to increased Chloride excretion from the enterocyte and decreased sodium reabsorption, leading to osmotic gradient, and water passes out of the cells into the intestinal lumen. “Rice water stool” • Many non-01/0139 strains are “non-toxigenic”. Actually other toxins some of which are invasive. It has also been hypothesized that the cystic fibrosis genetic mutation has been maintained in humans due to a selective advantage: heterozygous carriers of the mutation (who are thus not affected by cystic fibrosis) are more resistant to V. cholerae infections. “Cholera gravis” •Most people asymptomatic or mild illness only. However shed bacteria for 1-2 wks into the environment. • Severe illness, dehydration renal failure, metabolic acidosis and death. Diagnosis of Cholera • In epidemic “field situation”, dark field or wet film showing motile comma shaped bacteria usually sufficient. Motility inhibited by specific anti-sera. • Stool can be cultured in Alkaline Peptone water to select out vibrios. • TCBS (Thiosulphate Citrate Bile Salts) agar or Tellurite Taurocholate Gelatin Agar (TTGA). • Yellow oxidase positive colonies are suspicious • Suspicious colonies confirmed using API20E • V cholerae 01 and 0139 strains can be detected with specific anti-sera. • Latex agglutination, EIA or PCR can be used to look for cholera toxin TCBS Medium The high concentrations of thiosulfate and citrate and the strong alkalinity of this medium largely inhibit the growth of Enterobacteriaceae. Ox bile and cholate suppress primarily enterococci. Any coliform bacteria, which may grow, cannot metabolize sucrose. Only a few sucrose-positive Proteus strains can grow to form yellow, vibrid-like colonies Treatment of Cholera • Aggressive rehydration is necessary for serious cases. • Tetracyclines are the drug of choice. However in some parts of the world, resistance is becoming a problem. Quinolones also have good activity. • In pregnant and breastfeeding women, and children, Azithromycin is useful. Cholera Vaccine • Parenteral whole cell killed vaccine is available. Only 50% protection from 01 for 6 months, not recommended by WHO • Oral, killed, whole cell vaccine licensed for use in Europe, 1-2yrs protection after 2 doses. Vibrio vulnificus • First identified in the 1970s, can cause serious wound infections and septicaemia. • Usually infects patients with immunocompromise, particularly patients with underlying liver disease. • V. vulnificus found commonly in saltwater estuarine environments. (Isolated from virtually all oysters harvested in the Chesapeake Bay and the United States Gulf Coast when water temperatures exceeded 20ºC) Vibrio vulnificus: Pathogenicity Factors • Polysaccheride Capsule Anti-capsular antibodies are protective • Iron – Bacterial growth in human serum is directly related to percentage transferrin saturation with iron. Vibrio vulnificus Infection: Acquisition • Eating uncooked shellfish(especially in summer) • Wading in shallow estuarine environments where patient has skin breaks to the legs. Risk Factors for Vibrio vulnificus septicaemia • Alcoholic cirrhosis — 31 to 43 percent • Underlying liver disease including cirrhosis (unspecified etiology) and chronic hepatitis — 24 to 31 percent • Alcohol abuse without documented liver disease — 12 to 27 percent • Hereditary hemochromatosis — 12 percent • Chronic diseases such as diabetes mellitus, rheumatoid arthritis, thalassemia major, chronic renal failure, "preleukemia", and lymphoma — 7 to 8 percent Diagnosis of Vibrio vulnificus Infection • • • • Severe clinical picture Blue Green colonies on TCBS agar Halophilic API20E will give you a good idea, but other Vibrio species closely related biochemically. Treatment of Vibrio vulnificus Infection • Should consist of a 3rd generation Cephalosporin and a Tetracycline • Newer fluoroquinolones also effective. • Macrolides probably are also effective. Vibrio parahaemolyticus : What diseases does it cause? • Causes seafood associated diarrhoeal illness(usually oysters), and less commonly wound infections & septicaemia. • Pathogenicity associated with production of a thermostable haemolysin (Vp-TDH) in most cases. • A lot of V. parahaemolyticus bacteria don’t contain pathogenicity factors and are nonpathogenic. Vibrio parahaemolyticus How is it diagnosed and treated? • TCBS agar. Alkaline peptone water may be used as an enrichment broth, particularly when culturing stools. • Non-sucrose fermentor, therefore blue-green colonies on TCBS. • API 20 E ID, ?with additional NaCl • Clinically significant isolates will generally either be haemolytic or be urease positive. • Again treatment of severe disease should involve a 3rd generation cephalosporin and oral tetracycline Other Vibrios V. fluvialis V. mimicus V. furnissii V. Hollisae V. alginolyticus V. damsela Diarrhoeal Illness Wound Infections Summary • Vibrios can cause serious disease. The main three are V.cholerae, V. vulnificus & V. parahaemolyticus. • Appropriate plates should be set up when clinically suspected. • Reasonably easy to identify to Vibrio genus level, more difficult sometimes to get the species.