Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Orphan drug wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Compounding wikipedia , lookup
Neuropharmacology wikipedia , lookup
Plateau principle wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Prescription costs wikipedia , lookup
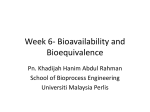
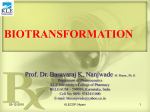
Prescription drug prices in the United States wikipedia , lookup
Drug design wikipedia , lookup
Drug discovery wikipedia , lookup
Drug interaction wikipedia , lookup
DRUG BIOAVAILABILITY Prof. Dr. Basavaraj K. Nanjwade M. Pharm., Ph. D Department of Pharmaceutics KLE University’s College of Pharmacy BELGAUM – 590010, Karnataka, India Cell No; 0091 9742431000 E-mail: [email protected] 18/11/2010 KLECOP, Nipani 1 Contents • • • • • • Introduction Objectives of bioavailability studies Considerations in bioavailability studies Bioavailability concept Importance of bioavailability Equivalent concept… Chemical, Pharmaceutical, Bioequivalence & Therapeutic equivalence. • Measurement of bioavailability 1. Pharmacokinetic method 2. Pharmacodynamic method • Measurement of Rate of absorption 1. The method of ‘Residuals’ 2. Wagner Nelson Method 18/11/2010 KLECOP, Nipani 2 Contents • Bioequivalence studies & Its importance Introduction FDA Determinations of Bioequivalence Main Terms FDA Methods to Determine Bioequivalence Bases for Determining Bioequivalence Design And Evaluation of Bioequivalence Studies Evaluation of the Data Clinical importance of bioequivalence studies 18/11/2010 KLECOP, Nipani 3 Introduction • The therapeutic effectiveness of a drug depends upon the ability of the dosage form to deliver the medicament to its site of action at a rate & amount sufficient to elicit the desired P’cological response. • This attribute of the dosage form is referred to as physiologic availability or bioavailability. 18/11/2010 KLECOP, Nipani 4 Introduction • The term bioavailability is defined as the rate and extent of absorption of unchanged drug from its dosage form. • A rapid onset of action is desired as in the treatment of acute conditions like asthma, pain, etc. • A slower absorption is desired when aim is to prolong the duration of action. 18/11/2010 KLECOP, Nipani 5 Introduction • The influence of route of administration on drug’s bioavailability is generally in the foll. order parenteral > oral > rectal > topical • Most drugs are administered orally, for reason of stability and convenience. • The dose available to patient – Bioavailable dose. 18/11/2010 KLECOP, Nipani 6 Introduction • The amount of drug that reaches the systemic circulation – systemic availability. • Bioavailable fraction (F), refers to the fraction of administered dose that enters the systemic circulation. • F = 18/11/2010 Bioavailable dose Administered dose KLECOP, Nipani 7 Objectives of bioavailability studies • It is important in 1. Primary stages of development of a suitable dosage form for new drug entity. 2. Determination of influence of excipients, patient related factors and interaction with other drugs on the efficiency of absorption. 18/11/2010 KLECOP, Nipani 8 Objectives of bioavailability studies 3. Development of new formulations of the existing drugs. 4. Control of quality of a drug product during early stages of marketing (to determine the influence of processing factors, storage & stability of absorption). 18/11/2010 KLECOP, Nipani 9 Considerations in bioavailability studies • Bioavailability – absolute vs. relative • Single dose vs. multiple dose • Human volunteer – healthy subject vs. patients 18/11/2010 KLECOP, Nipani 10 Bioavailability – absolute vs. relative • Absolute bioavailability : when the systemic availability of the drug administered orally is determined in comparison to its i.v. administration. • Relative bioavailability : when the systemic availability of the drug administered orally is compared with that of an oral standard of the same drug. 18/11/2010 KLECOP, Nipani 11 Plasma concentration Plasma concentration vs. time profile of a drug ingested orally & intravenously. 70 60 i.v. route 50 40 oral route 30 20 10 0 0 18/11/2010 2 4 TimeKLECOP, (hours) Nipani 6 8 10 12 Single dose vs. multiple dose Single dose • Very common & easy Multiple dose • Difficult to control • Less exposure to drug & less tedious • More exposure to drug & tedious • Difficult to predict steady state • Time consuming 18/11/2010 KLECOP, Nipani 13 Time to reach steady state Concentration due to repeated doses Concentration due to a single dose 18/11/2010 KLECOP, Nipani 14 Single dose vs. multiple dose • Multiple dose study has several advantages like 1. More accurately reflects the manner in which the drug should be used. 2. Drugs levels are higher due to cumulative effect which makes its determination possible even by less sensitive analytical methods. 18/11/2010 KLECOP, Nipani 15 Single dose vs. multiple dose 3. Better evaluation of the performance of controlled release formulation is possible. 4. Small intersubject variability is observed which allows use of fewer subjects. 5. Nonlinearity in pharmacokinetics, if present, can be easily detected. 18/11/2010 KLECOP, Nipani 16 Human volunteer – healthy subject vs. patients • Ideally, the bioavailability study should be carried out in patients for whom the drug is intended to be used. • Advantages : 1. Patient is benefited from the study. 2. Reflects better therapeutic efficacy of drug. 18/11/2010 KLECOP, Nipani 17 Human volunteer – healthy subject vs. patients 3. Drug absorption pattern in disease state can be evaluated. 4. Avoids the ethical quandary of administering drug to healthy subjects. 18/11/2010 KLECOP, Nipani 18 Human volunteer – healthy subject vs. patients • There are some drawbacks of using patients as volunteers. • Stringent conditions such as fasting state required is difficult to be followed by the patients. • Studies are therefore performed in young (20-40 yrs.), healthy males adult volunteers. 18/11/2010 KLECOP, Nipani 19 Human volunteer – healthy subject vs. patients • Female volunteers are used only when drugs such as oral contraceptives are to be tested. • No. of subject- extent of intersubject variability – minimum required to obtain reliable data. • They must be informed about the importance of Study conditions to be followed Possible hazards if KLECOP, any. Nipani 18/11/2010 20 Human volunteer – healthy subject vs. patients • Medical examination should be performed. • Drug washout period for min. of ten biological half lives must be allowed for between two studies in same subject. 18/11/2010 KLECOP, Nipani 21 Bioavailability Concept • Rate and extent at which therapeutically active drug reaches systemic circulation. • The fraction of administered dose that reaches the systemic circulation in contrast to that stated on label. • Rate & extent of absorption of unchanged drug from its dosage form. • A measure relative to some standard of rate & amount of drug ,which reaches the systemic circulation unchanged following the administration of dosage form. 18/11/2010 KLECOP, Nipani 22 Why bioavailability studies…? • FDA requires that the drug product is safe and effective. • Measure of bioavailability: AUC/dose • Absolute availability - for drugs with approved NDA, bioavailability studies are required for new drug formulations -bioequivalence to the reference formulation • Relative availability - for drugs without full NDA, bioequivalence to the reference drug in the standard formulation • For determining safety & efficacy of drug product. 18/11/2010 KLECOP, Nipani 23 Concept of Equivalents • A comparative term. • One drug product is similar with respect to a specific characters or function to another . • Defined a set of standard. • Four types … 1. Chemical 2. Pharmaceutical 3. Bioequivalence 4 .Therapeutic 18/11/2010 KLECOP, Nipani 24 Concept of Equivalents 1. Chemical Equivalence Two or more drug products which contain same amount of same active ingredient. 2. Pharmaceutical Equivalence Identical in strength,quality,purity, content uniformity & disintegration – dissolution characters … they may differ in containing different excipient. 18/11/2010 KLECOP, Nipani 25 Concept of Equivalents 3. Bioequivalence A relative term which denotes ..the drug substance in two or more identical dosage form reaches the systemic circulation at the same relative rate & to same relative extent. 4. Therapeutic Equivalence Two or more bioequivalent having same therapeutically active ingredient elicit pharmacological effects & can control the disease to same extent. 18/11/2010 KLECOP, Nipani 26 Measurement of bioavailability • Pharmacokinetic methods ( indirect ) 1. Blood analysis 2. Urinary excretion data • Pharmacodynamic methods ( direct ) 1. Acute pharmacological response 2. Therapeutic response 18/11/2010 KLECOP, Nipani 27 Blood analysis • Plasma level time studies or The plasma concentration – time curve or blood level curve. • A direct relationship exists concentration of drug at the site of action & concentration of drug in the plasma. • Serial blood samples are taken after drug administration & analyzed for drug concentration. • A typical blood level curve obtained after oral administration of drug. 18/11/2010 KLECOP, Nipani 28 18/11/2010 KLECOP, Nipani 29 Parameters determined Pharmacokinetic parameters • Peak Plasma Concentration (Cmax) • Time of Peak concentration (tmax). • Area Under Curve (AUC) • • • • • 18/11/2010 Pharmacodynamics parameters Minimum Effective Concentration (MEC) / Minimum Inhibitory Concentration (MIC). Maximum Safe Concentration (MSC) / Maximum Safe Dose (MSD). Duration of action Onset of action. Intensity of action. KLECOP, Nipani 30 Parameters determined • AUC or Extent of absorption can be measured by 3 methods… 1.Planimeter Instrument for mechanically measuring the area 2. Cut & weigh method AUC is cut & weighed on analytical balance. The weight obtained is converted to proper unit by dividing it by the wt of a unit area of same paper. 3. Trapezoidal method 18/11/2010 KLECOP, Nipani 31 Parameters determined 3. Trapezoidal method AUC = ½ ( C1 + C2) (t2 – t1) + ½ (C2 + C3) (t3 – t2) +……. ½ (C n-1 + C n ) (tn – tn-1 ) C = Concentration t = time subscript= sample number AUC = Area Under Curve 18/11/2010 KLECOP, Nipani 32 Parameters determined Relative bioavailability F rel = ( AUC) drug . (Dose) standard (AUC) standard .(Dose) drug Absolute bioavailability Fab = 18/11/2010 (AUC)drug . (Dose) IV (AUC)IV . (Dose) drug KLECOP, Nipani 33 Parameters determined •From the following blood data obtained after the oral administration of 50mg of drug A. calculate the AUC? Time in hr Plasma drug con in mcg/ml 1 2 5.5 9.2 3 14.9 4 5 10.3 7.3 6 2.2 AUC = ½ (5.5 +9.2) (2-1) + ½ (9.2+14.9) (3-2) + ½ (14.9+10.3) (4-3) ½ (10.3+ 7.1)(5-4) + ½ (7.1 +2.2) (6-5) AUC = 45.35 mcg/ml hr 18/11/2010 KLECOP, Nipani 34 Parameters determined • The AUC of a new sustained release diclofenac sodium developed in the lab after giving in a dose of 100mg was found to be 250.30 mcg/ml hr.The AUC of the standard marketed sustained release tablets of the same at the same dose was found to be 261.35 mcg/ml hr. what is the the relative bioavailability of he same drug. F rel = 250.30 X 100 261.35 X 100 = 0.9577 or 95.77% 18/11/2010 KLECOP, Nipani 35 Parameters determined • The AUC of salbutamol sulphate from a 10 mg IV dose was found to be 94.6mcg/ml hr.when the same dose was given orally, the AUC was found to be 60.5 mcg/ml hr. What is the absolute bioavailability of the drug? Fabs = 60.5 X 10 94.6 X 10 Fabs = 0.6395 or 63.95 18/11/2010 KLECOP, Nipani 36 Urinary excretion data • The method of determination bioavailability provided that the active ingredient is excreted unchanged in the significant quantity of urine. • The cumulative amount of active drug excreted in urine is directly proportional to extent of systemic drug absorption. • The rate of drug excretion is directly proportional to rate of systemic drug absorption. 18/11/2010 KLECOP, Nipani 37 Advantages • Useful when there is lack of sufficiently sensitive analytical techniques to measure concentration of drug in plasma. • Noninvasive method therefore better subject compliance. • Convenience of collecting urine samples in comparison to drawing of blood periodically. • If any case the urine drug concentration is low, assaying of larger sample volume is relatively more. • Direct measurement of bioavailability, both absolute & relative is possible without the necessity of fitting the data to the mathematical model. 18/11/2010 KLECOP, Nipani 38 Advantages 18/11/2010 KLECOP, Nipani 39 Advantages • Bioavailability is determined by…. F= (U (U ) oral . D IV ) IV . D oral U = Cumulative amt of unchanged drug excreted in urine D IV = IV dose D oral = oral dose F = absolute bioavailability 18/11/2010 KLECOP, Nipani 40 Advantages • When equal doses are administered Intravenously & Orally….. F = (U (U ) oral ) IV F = (U (U ) test ) standard 18/11/2010 KLECOP, Nipani 41 Advantages • When drug A was administered IV to a group of volunteers, 80% of the 500mg dose was recovered unchanged in the urine. When the same drug was administered to the same volunteers orally.280 mg was recovered unchanged in urine. What is the absolute bioavailability of Drug A following oral administration. Absolute bioavailability = (cumulative amt.of drug excreted)sample (cumulative amt.of drug excreted)IV = 280 400 = 0.7 or 70% 18/11/2010 KLECOP, Nipani 42 Acute pharmacological response • Bioavailability can be determined from the acute pharmacologic effect – time curve as well as from dose response graph. • DISADVANTAGE is that pharmacological response tends to more variable & accurate correlation between the measured response & drug available from the formulation is difficult. 18/11/2010 KLECOP, Nipani 43 Therapeutic response • This method is based on the observing the clinical response to a drug formulation given to a patients suffering from disease for which it is intended to be used. • Ex …for anti inflammatory drugs, the reduction in the inflammation is determined. • The major DRAWBACK is …quantification of observed response is too improper to allow for reasonable assessment of relative bioavailability between two dosage forms of a same drug. 18/11/2010 KLECOP, Nipani 44 Rate of Absorption • AUC/dose gives an average extent of bioavailability. • The rate of absorption is usually also important for the onset of drug action. • The time of peak plasma concentration is used often as a measure of the rate of drug absorption. • The peak plasma concentration is also an important parameter - for keeping the drug concentration within the therapeutic window. • Absorption can be characterized by evaluating the absorption rate constant Ka from the plasma concentration –time data. 18/11/2010 KLECOP, Nipani 45 The method of ‘Residuals’ • Also called as Feathering or peeling or stripping. ASSUMPTIONS • Absorption & elimination process follows 1st order kinetics. • Absorption from the dosage form is complete. • Ka is at least five times larger than Ke • Kinetic model is AG 18/11/2010 Ka AB Kc KLECOP, Nipani AE 46 The method of ‘Residuals’ 18/11/2010 KLECOP, Nipani 47 The method of ‘Residuals’ • This technique is used to resolve a multiexponential curve into its individual components. • For a drug that follows one compartment kinetics & administered e.v, the concentration of drug in plasma is expressed by… C= Ka F X0 Vd ( Ka –KE ) [ e –kEt – e –Kat ] 1 If Ka F X0 / Vd ( Ka – kE ) = A, a hybrid constant then, C=Ae 18/11/2010 –kEt -A e –Kat KLECOP, Nipani 2 48 The method of ‘Residuals’ • During the elimination phase, when the absorption is almost over, Ka > > KE & the value of second exponential e –Kat approaches zero whereas the 1st exponential e –kEt retains some finite value….at this time the equation is C = A e –kEt in log form log C = log A – KEt/ 2.303 3 4 Where C is the back extrapolated plasma concentration value. A plot of log C versus t yields a biexponential curve with a terminal linear phase having slope KE/ 2.303. 18/11/2010 KLECOP, Nipani 49 The method of ‘Residuals’ • Back extrapolation of this straight line to zero yields y-intercept equal to log A. • Subtraction of true plasma concentration values that is equation 2 from the extrapolated plasma concentration values that is equation 3 yields a series of residual concentration values Cr ( C - C ) = Cr = A e –Kat , in log form the equation is : log Cr = log A - Kat/ 2.303 18/11/2010 KLECOP, Nipani 50 The method of ‘Residuals’ • A plot of logCr versus t yields a straight line with slope –Ka / 2.303 & y intercept log A. • Absorption half life can be computed from Ka using the relation 0.693/Ka …thus the method of residual enables resolution of the biexponential plasma level time curve into its exponential components. • The technique works best when the difference between Ka & KE is large ( Ka >= 3) 18/11/2010 KLECOP, Nipani 51 Wagner Nelson Method ASSUMPTIONS • The body behaves as a single homogenous compartment. • Drug elimination obeys 1st order kinetics. DISADVANTAGES • The absorption & elimination processes can be quite similar & still accurate determination of Ka can not be made. • The absorption process doesn’t have to be 1st order. • The kinetics of absorption may be zero order, mixed order, mixed zero order & 1st order or even more complex. • This method involves determination of Ka from percent absorbed –time plot & does not require the assumption of zero . 18/11/2010 KLECOP, Nipani 52 Wagner Nelson Method • The amount of drug in the body X & the amt of drug eliminated in the body XE thus : XA = X + X E If the amt of drug in the body is X = V.dC…the amt of drug eliminated at any time t can be calculated as .. XE = KE Vd ( AUC)to Substitution of values of X & XE in above equation… XA = Vd C + KE Vd ( AUC)to from this equation we can get the value for drug absorbed in to the systemic circulation from time zero to 18/11/2010 KLECOP, Nipani 53 Wagner Nelson Method 18/11/2010 KLECOP, Nipani 54 BIOEQUIVALENCE STUDIES & ITS IMPORTANCE 18/11/2010 KLECOP, Nipani 55 BIOEQUIVALENCE STUDIES • Bioavailability & bioequivalence data is required to be furnished with application of new drugs, as required under schedule Y, depending upon the type of application being submitted. • Both bioavailability & bioequivalence focus on release of drug substance from its dosage form & subsequent absorption into systemic circulation. 18/11/2010 KLECOP, Nipani 56 • 1. 2. 3. 4. Several test methods are available to asses equivalence, including; Comparative bioequivalence studies, in which the active drug substance or one or more metabolites is measured in accessible biological fluid such as plasma, blood or urine. Comparatives pharmacodynamic studies in humans Comparative clinical trials In-vitro dissolution tests 18/11/2010 KLECOP, Nipani 57 FDA Determinations of Bioequivalence Main Terms • • • • Pharmaceutical equivalents Pharmaceutical alternatives Therapeutic equivalents Bioequivalence 18/11/2010 KLECOP, Nipani 58 Pharmaceutical Equivalents • Drug products are considered pharmaceutical equivalents if they contain the same active ingredient (s), have the same dosage form and route of administration, and are identical in strength or concentration • Equivalent products contain the same amount of ingredient in the same dosage form but may differ in characteristics, such as shape, release mechanisms, and packaging 18/11/2010 KLECOP, Nipani 59 Pharmaceutical Alternatives • Drug products are considered pharmaceutical alternatives if they contain the same therapeutic moiety, are different salts, esters, or complexes of the same moiety, are different dosage forms, or are different strengths • Other pharmaceutical alternatives – Different dosage forms and strengths within a single product line by a single manufacturer – Extended-release formulations when compared with immediate- or standard-release formulations 18/11/2010 KLECOP, Nipani 60 Therapeutic Equivalents • Drug products are considered therapeutic equivalents if they are all of the following – – – – – Pharmaceutical equivalents Bioequivalent Approved as safe and effective Adequately labeled Manufactured in compliance with current Good Manufacturing Practice regulations • Therapeutic equivalents are expected to have the same clinical effect and safety profile 18/11/2010 KLECOP, Nipani 61 Bioequivalence • Bioequivalence of a drug product is achieved if its extent & rate of absorption are not statistically significantly different from those of the reference product when administered at the same molar dose. 18/11/2010 KLECOP, Nipani 62 FDA Methods to Determine Bioequivalence • Generic drug manufacturers must demonstrate that a drug is bioequivalent to a reference drug product • In order of FDA preference, methods used to define bioequivalence – Pharmacokinetic studies – Pharmacodynamic studies – Comparative clinical trials – In vitro studies 18/11/2010 KLECOP, Nipani 63 Important PK parameters Cmax: the observed maximum concentration of a drug measure of the rate of absorption AUC: tmax: time at which Cmax is observed area under the concentration-time curve measure of the extent of absorption measure of the rate of absorption 18/11/2010 KLECOP, Nipani 64 Studies Different approach for establishing equivalence PD studies 18/11/2010 clinical studies KLECOP, Nipani in vitro methods 65 Methods for Assessing Bioavailability & Bioequivalence • Plasma Drug Concentration:1. The time for peak plasma (blood) concentration (tmax) 2. The peak plasma drug concentration (cmax) 3. The area under the plasma drug concentration versus time curve (AUC) 18/11/2010 KLECOP, Nipani Contd… 66 Plasma concentration time profile Cmax AUC Tmax 18/11/2010 KLECOP, Nipani 67 • Urinary Drug Excretion:- 1. Cumulative amount of drug excreted in the urine (Du) 2. The rate of drug excretion in the urine (dDu/dt) 3. The time for maximum urinary excretion (t) 18/11/2010 KLECOP, Nipani 68 • Acute pharmacodynamic effect:1. Max. pharmacodynamic effect (Emax) 2. Time for max. pharmacodynamic effect 3. Area under pharmacodynamic effect versus time curve 4. Onset time for pharmacodynamic effect 18/11/2010 KLECOP, Nipani 69 • Clinical observations Well controlled clinical trials • In-Vitro studies Drug dissolution. 18/11/2010 KLECOP, Nipani 70 • Area Under Curve:AUC is the measurement of the extent of the drug bioavailability. It is the area under the drug plasma level-time curve from t =0 & t = ∞, and is equal to the amount of unchanged drug reaching the general circulation divided clearance [ AUC]0∞ = ∫0∞Cpdt [ AUC]0∞ = FD0 = FDO/ kVD Clearance 18/11/2010 KLECOP, Nipani 71 Where F = fraction of dose absorbed Do = dose, k = elimination rate constant, VD = volume of distribution AUC is independent of route of administration and process of drug elimination as long as the elimination process don’t change. The AUC can be determined by numerical integration procedure such as trapezoidal rule method. The units for AUC are concentration time ( μg hr/ml) 18/11/2010 KLECOP, Nipani 72 • For many drugs, AUC is directly proportional to the dose, for eg. If a single dose of drug is increased from 250- 1000mg the AUC will also show a four fold increase fig Plasma level time curve following administration of single doses of (A)250mg, (B)500mg & (C)1000mg of drug. 18/11/2010 KLECOP, Nipani 73 Linear relationship between AUC & dose 18/11/2010 KLECOP, Nipani 74 • In some cases the AUC is not directly proportional to the administered dose for all dosage levels, for eg. As the dosage of the drug is increased, one of the pathway for drug elimination becomes saturated, fig Relationship between AUC & dose when metabolism is saturable 18/11/2010 . KLECOP, Nipani 75 • Drug elimination includes metabolism and excretion. • for drugs such as salicylates and phenytoin continuous increase of dose causes saturation of one of the enzyme pathway for drug metabolism and consequent prolongation of elimination of half life. • The AUC thus increases disproportionally to the increase in dose because smaller amount of drug is being eliminated. 18/11/2010 KLECOP, Nipani 76 • When AUC is not directly proportional to the dose, bioavailability of the drug is difficult to evaluate because drug kinetics may be dose dependent. 18/11/2010 KLECOP, Nipani 77 Urinary Drug Excretion Data • It is an indirect method for estimating bioavailability. • The drug must be excreted in significant quantities as unchanged drug in the urine, timely urine samples must be collected and total amount of urinary excretion must be obtained. 18/11/2010 KLECOP, Nipani 78 • Du∞:- The cumulative amount of drug excreted in the urine, Du∞ is directly related to total amount of drug absorbed. Experimentally, urine samples are collected periodically after administration of the drug product. Each urine specimen is analyzed for free drug with a specific assay. 18/11/2010 KLECOP, Nipani 79 Graph is plotted between cumulative drug excreted to the collection time interval. 18/11/2010 KLECOP, Nipani 80 • The relationship between cumulative amount of drug excreted in urine and plasma level time curve is shown in fig., ( 1) 18/11/2010 KLECOP, Nipani 81 • When the drug is almost completely eliminated (point c), the plasma concentration approaches zero and maximum amount of the drug excreted in the urine, Du∞ is obtained 18/11/2010 KLECOP, Nipani 82 • dDu/dt Because most drugs are eliminated by first order rate process, the rate of drug excretion is dependent on first order elimination rate constant k and the concentration of drug in the plasma Cp. In fig, the maximum rate of drug excretion would be at point B, the minimum rate of drug excretion would be at point A and C. 18/11/2010 KLECOP, Nipani 83 (2) Graph comparing rate of drug excretion w.r. to time should be similar in shape as the plasma level- time curve for that drug. 18/11/2010 KLECOP, Nipani 84 • t∞ :it is the total time for the drug to be excreted. In fig 1 & 2, slope of curve segment A-B is related to the rate of drug absorption, whereas point C is related to the total time required after drug administration for the drug to be absorbed and completely excreted ( t = ∞). 18/11/2010 KLECOP, Nipani 85 Acute Pharmacodynamic effect • An Acute Pharmacodynamic effect such as an effect on pupil diameter, heart rate, or B.P can be used as an index of drug bioavailability. • In this case, an acute pharmacodynamic effect- time curve is constructed. Measurement of pharmacodynamic effect should be made with sufficient frequency to permit a reasonable estimate of the total AUC for a time period at least three times a half life of the drug. 18/11/2010 KLECOP, Nipani 86 • In this to determine bioavailability requires demonstration of a dose related response. • Bioavailability is determined by characterization of dose-response curve. • PD parameters that are obtained include total area under the acute PD effect- time curve, peak PD effect, & time for peak PD effect. • onset time & duration of PK effect may also be included in the analysis of data. 18/11/2010 KLECOP, Nipani 87 Clinical Observations • Well-controlled clinical trials in humans that establish the safety & effectiveness of the drug product. • This approach is least accurate, least sensitive & least reproducible of the general approaches for determining in-vivo bioavailability. 18/11/2010 KLECOP, Nipani 88 • The FDA only consider this approach when analytical methods are not available to permit use of one of the approaches described above. • An E.g. of this approach is for the determination of bioequivalence of two topical antifungal products by different mfgs. Containing the same active antifungal agent (ketoconazole) 18/11/2010 KLECOP, Nipani 89 In-Vitro Studies • Under certain conditions give an indication of drug bioavailability. Ideally, in-vitro dissolution rate should correlate with invivo drug bioavailability. 18/11/2010 KLECOP, Nipani 90 Bases for Determining Bioequivalence • Bioequivalence is established if the in-vivo bioavailability of a test drug product (Generic product) does not differ significantly in the products rate & extent of drug absorption, as determined by comparison of measured parameters (eg, concentration of active drug ingredient in blood, urinary excretion rate, or PD effects), from that of the reference material (Brand name product). 18/11/2010 KLECOP, Nipani 91 Design And Evaluation of Bioequivalence Studies • Bioequivalence studies are performed to compare bioavailability of generic drug product to the brand name product. • Design and evaluation of bioequivalence studies requires comparative inputs from; PKs, statisticians, clinicians, bioanalytical chemist, & others. 18/11/2010 KLECOP, Nipani 92 18/11/2010 KLECOP, Nipani 93 • Basic design for BE is determined by ; 1. The scientific questions to be answered, 2. The nature of reference material & dosage form to be tested, 3. The availability of analytical methods, 4. Benefit-risk considerations with regards to testing in humans. • For some generic drugs, FDA offers general guidelines for conducting these studies. 18/11/2010 KLECOP, Nipani 94 • Eg, “Statistical procedure for bioequivalence studies using a standard two-treatment crossover design” • The publication addresses three specific aspects, including; 1. Logarithmic transformation of PK data, 2. Sequence effect 3. Outlier consideration. • With such guidelines, the principal investigator should prepare a detailed Protocol for the study. 18/11/2010 KLECOP, Nipani 95 • For bioequivalence studies, both test & reference drug formulations contain pharmaceutical equivalent drug in the same dose strength, in similar dosage forms (immediate release or controlled release), & both are given by the same route of administration. • Both single &/or a multiple dose (steady state) study required. 18/11/2010 KLECOP, Nipani 96 • Prior to initiation of the study, the Institutional Review Board (IRB) of the clinical facility in which the study is to be performed must approve the study. • Generally study is performed in normal, healthy male volunteers. • The number of subjects depend upon the expected intersubject variability. • The subject is generally fasted 10 to 12 hrs (overnight) prior to drug administration & may continue to fast for 2 to 4 hr period after dosing. 18/11/2010 KLECOP, Nipani 97 Reference standard • Before beginning an in-vivo bioequivalence study, the total content of active drug substance in the Test product must be within 5% of reference product. 18/11/2010 KLECOP, Nipani 98 Study Design • The FDA, Division of Bioequivalence, Office of Generic Drugs provides a guidance for the performance of In-vitro dissolution & in-vivo bioequivalence studies. • Currently, three different studies may be required for solid oral dosage forms, including; 18/11/2010 KLECOP, Nipani 99 1. Fasting study 2. Food intervention study 3. Multiple dose (steady state) Fasting study:• Bioequivalence studies are evaluated by single dose, two-period, two-treatment, two-sequence, open label, randomized crossover design comparing equal doses of the test and reference products in fasted, adult, healthy subjects. 18/11/2010 KLECOP, Nipani 100 • This study required for all immediate release and modified release oral dosage forms. • Both male and female subjects used in the study. • Blood sampling is performed just prior (zero time) to the dose and at appropriate intervals after the dose to obtain an adequate plasmadrug concentration versus time profile. • No other medication is normally given to subject for atleast one week prior to the study. 18/11/2010 KLECOP, Nipani 101 Food intervention study:• This study is single dose, randomized, three-treatment, three-period, sixsegments, crossover, limited food effect study comparing equal dosage of the test product given under fasting conditions with those of the test and reference products given immediately after a standard high fat content breakfast. • For eg. Ibuprofen 18/11/2010 KLECOP, Nipani 102 Multiple dose ( steady state study ):- • A multiple dose steady state, randomized, twotreatment, two-way, crossover study comparing equal dosage of the test and reference products in the adult, healthy subject is required for the oral extended release (controlled release) drug products in addition to a single dose fasting study and food intervention study. • Three consecutive trough concentrations (Cmin) on three consecutive days should be determined to ascertain that the subjects are at steady state. 18/11/2010 KLECOP, Nipani 103 • The last morning dose is given to the subject after an overnight fast with continuous fasting for atleast two hours following dose administration. • Blood sampling is performed similarly to the single dose study. 18/11/2010 KLECOP, Nipani 104 Crossover Designs • Subjects who meet the inclusion and exclusion study criteria and have given informed consent are selected at random. • Each subject recieves the test drug product and the reference product. • E.g. of Latin square crossover design for a bioequivalence study In human volunteers, comparing three different drug formulations (A, B, C) are described in tables 18/11/2010 KLECOP, Nipani 105 Crossover Designs Subject Drug Product 1 Study period 1 A Study period 2 B Study period 3 C 2 B C A 3 C A B 4 A C B 5 C B A 6 B A C 18/11/2010 KLECOP, Nipani 106 • The Latin square design plans the clinical trial so that each subjects receives each drug product only once, with adequate time between medications for the elimination of drug from the body. • In this design, each subject is his own control, and subject-to-subject variation is reduced. • The variation due to sequence, period and treatment (formulation) are reduced, so that all patients don’t receive the same drug product on the same day and in the same order 18/11/2010 KLECOP, Nipani 107 • Possible carry-over effect from any particular drug product are minimized by changing the sequence in which the drug products are given to the subjects as in the table. • This Latin square design for bioequivalence study of 4 drug products in 16 volunteers may also be performed. • After each subject recieves the drug product, blood samples are collected at the appropriate time intervals so that valid blood drug level-time curve is obtained. 18/11/2010 KLECOP, Nipani 108 • The time intervals should be spaced so that peak blood concentration, total AUC, and the absorption and the elimination phases of the curve may be well described. • In some cases the measurement of drug in urine may be necessary. • Period refers to the time period in which study is performed. 18/11/2010 KLECOP, Nipani 109 • A two period study, referred to as two legged study, means that the study is performed on two different days (time periods) seperated by a wash out period during which most of drug has been eliminated from the body- generally 10 elimination half lives. • A sequence refers to the number of different orders in the treatment groups in a study. 18/11/2010 KLECOP, Nipani 110 • E.g. two-sequence, two-period study designed as follows:Period 1 Period 2 Sequence 1 T R Sequence 2 R T R = reference , T = treatment As shown in the table 18/11/2010 KLECOP, Nipani 111 Evaluation of the Data • Analytical method:The method for measurement of the drug must be validated for accuracy, precision, sensitivity, and specificity. Data should be presented in tabulated and graphical form for evaluation. The plasma drug conc. Versus time curve for each drug product and each subject should be available. 18/11/2010 KLECOP, Nipani 112 • Pharmacokinetic evaluation of the data:For single dose studies, including fasting study or food intervention study, the PK analyse include calculation for each subject of the AUC to the last quantifiable concentration (AUC0-t) and to infinity (AUC0-∞), Tmax and Cmax. Elimination rate constant k, elimination half life t ½ may be estimated. 18/11/2010 KLECOP, Nipani 113 • Statistical evaluation of the data:To prove bio-equivalence, there must be no statistical difference between the bioavailability of test product and reference product. Statistical approaches assume that the data are distributed according normal distribution or bell shaped curve. The log transformation of the bioavailability data (Cmax, AUC) is performed prior to statistical data evaluation for bioequivalence determination. 18/11/2010 KLECOP, Nipani 114 • Analysis of variance (ANOVA):It is a statistical procedure used to test the data for difference within and between treatment and controlled groups. The ANOVA may evaluate variability in subjects, treatment groups, study periods, formulation and other variables depending on study design. 18/11/2010 KLECOP, Nipani 115 • One sided tests procedure:This is also referred as confidence interval approach. This method is used to demonstrate if the bioavailability of the drug from the test formulation is too low or high in comparison to the reference drug. For a single dose, fasting study, analysis of variance (ANOVA) is usually performed on the log-transformed AUC and Cmax. There should be no statistical difference between mean AUC and Cmax parameters for the test (generic) and refernce drug products. 18/11/2010 KLECOP, Nipani 116 In addition, 90% confidence intervals about the ratio of the mean for AUC and Cmax values of the test drug should not be less than 0.80 (80%) nor greater than 1.25 (125%) of the reference product based on log-transformed data. 18/11/2010 KLECOP, Nipani 117 Clinical importance of bioequivalence studies • Bioequivalence of different formulations of the same drug substance involves equivalence with respect to the rate and extent of systemic absorption. • Generally two formulations whose rate and extent of absorption differ by 20% or less are considered bioequivalent • When a therapeutic objectives of the drug are considered, an equivalent clinical response should be obtained from the comparison dosage form if the plasma drug concentration remain above MEC for appropriate interval and don’t reach the MTC. 18/11/2010 KLECOP, Nipani 118 Clinical importance of bioequivalence studies • Bioequivalence studies should be conducted for the comparison of two medicinal products containing the same active substance. • Two products marketed by different licensees, containing same active ingredient(s), must be shown to be therapeutically equivalent to one another in order to be considered interchangeable. 18/11/2010 KLECOP, Nipani 119 Special concerns in bioavailability & bioequivalence studies. • The bioequivalence determination of the drugs that are not absorbed systemically form the site of application is difficult to assess. For this non-systemic absorbable drugs surrogate marker is needed for the bioequivalence determination • Possible surrogate markers for bioequivalence studies are given in table. 18/11/2010 KLECOP, Nipani 120 Drug product Possible surrogate marker for bioequivalence MDI Albuterol FEV1 Topical steroid Hydrocortisone Skin blanching Anion exchange cholestryamine Binding to bile resin acids Antacids Mg and Al Neutraliztion of hydroxide gel acid Topical ketoconazole Drug uptake into antifungal stratum corneum 18/11/2010 Drug KLECOP, Nipani 121 Reference standard • Before beginning an in-vivo bioequivalence study, the total content of active drug substance in the Test product must be within 5% of reference product. 18/11/2010 KLECOP, Nipani 122 References • Dissolution, bioavailability & bioequivalence – Hamed M. Abdou, Mack publishing company, Pg.no. 297-299. • Biopharmaceutics & pharmacokinetics – D.M.Bramhankar, S.B.Jaiswal, Pg.no. 297-299. • Biopharmaceutics & pharmacokinetics – Robert E. Notari, 2nd edition, Marcel Dekker. •18/11/2010 www.google.com KLECOP, Nipani 123 References • “Applied Biopharmaceutics & pharmacokinetics”, Leon Shargel & Andrew B.C. • Leon Shargel, Andrew Yu; “Applied biopharmaceutics & Pharmacokinetics”, 4th edition • Peter G. Welling, Francis L.S. Tse; “Pharmaceutical Bioequivalence”, Vol 48, Dekker Series. 18/11/2010 KLECOP, Nipani 124 THANK YOU Cell No: 0091 9742431000 E-mail: [email protected] 18/11/2010 KLECOP, Nipani 125