Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
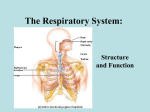
Respiratory Emergencies Beyond the Objectives 1 Discussion Points: Respiratory Anatomy & Physiology Pathophysiology Assessment of the Respiratory System Management of Respiratory Disorders Specific Respiratory Diseases 2 Anatomy & Physiology Review • Function • Takes in oxygen • Disposes of wastes • Carbon dioxide • Excess water 3 Anatomy & Physiology Review a) Nose and mouth b) Oropharynx c) Nasopharynx d) Pharynx c) Epiglottis d) Larynx e) Cricoid cartilage 4 Anatomy & Physiology Review Lower Airway a) Trachea b) Lungs c) Bronchi d) Bronchioles e) Alveoli f) Diaphragm g) Intercostal Muscles 5 Anatomy & Physiology Review • Bronchioles • Smallest airways • Walls consist entirely of smooth muscle (no cartilage present) • Constriction increases resistance to airflow • Dilation reduces resistance to airflow 6 Anatomy & Physiology Review • Alveoli • Air sacs • Site of oxygen and carbon dioxide exchange with blood 7 Anatomy & Physiology Review Pleura -Visceral -Parietal 8 Anatomy & Physiology Review • Inhalation • Diaphragm and intercostal muscles contract, increasing the size of the thoracic cavity. • Air flows into the lungs. - Active Process 9 Anatomy & Physiology Review • Exhalation -Diaphragm and intercostal muscles relax decreasing the size of the thoracic cavity. -Air flows out of the lungs. -passive process 10 Anatomy & Physiology Review • Alveolar/capillary exchange • Oxygen-rich air enters the alveoli during each inspiration. • Oxygen-poor blood in the capillaries passes into the alveoli. • Oxygen enters the capillaries as carbon dioxide enters the alveoli. 11 Anatomy & Physiology Review • Capillary/cellular exchange • Cells give up carbon dioxide to the capillaries. • Capillaries give up oxygen to the cells. O2 + Glucose The Cell CO2 + H2O 12 Adequate/Inadequate Breathing Assess….. Rate Rhythm Quality 13 Adequate/Inadequate Breathing • Rate • Normal Rate • Adult – 12-20/minute • Child – 15-30/minute • Infant – 25-50/minute 14 Adequate/Inadequate Breathing • Rhythm • Regular • Irregular 15 Adequate/Inadequate Breathing • Quality • Breath Sounds • Effort of Breathing • Chest Expansion 16 Adequate/Inadequate Breathing • Other indications that your patient is breathing inadequately. • • • • • Cyanosis Cool Clammy Skin Nasal Flaring Agonal Respirations Tripoding 17 Anatomy & Physiology Review • Infant & Child Airway Considerations • • • • • • Smaller airway passages Large tongue Softer pliable structures Cricoid cartilage is narrowest point. Heavily dependant on diaphragm Larger head 18 Breathing Difficulty (Signs & Symptoms) Shortness of Breath Restlessness Increased Pulse Rate Increased Breathing Rate Skin Color Changes • Cyanotic • Pale • Flushed 19 Breathing Difficulty (Signs & Symptoms) Noisy Breathing Inability to Speak Retractions Shallow or Slow Breathing Abdominal Breathing Coughing Irregular Breathing Rhythms Patient Position 20 Assessment of the Respiratory Emergency Scene Size-up • Threats to Safety • Identify rescue environments having decreased oxygen levels. • Gases and other chemical or biological agents. • Clues to Patient Information 21 Assessment of the Respiratory Emergency • Initial Assessment • General Impression • Position • Color • Ability to speak • Respiratory effort • LOC • AVPU • Chief Complaint/Apparent Life Threats 22 Assessment of the Respiratory Emergency Initial Assessment (cont): Airway -Assure there is no obstruction -Proper ventilation cannot take place without an adequate airway. Breathing -Absent or abnormal breath sounds -Speaking limited to 1–2 words -Use of accessory muscles or presence of retractions Circulation -Tachycardia -Severe central cyanosis, pallor, or diaphoresis 23 Focused History & Physical Exam History SAMPLE History OPQRST History • • • • Paroxysmal nocturnal dyspnea and orthopnea Coughing and hemoptysis Associated chest pain Smoking history or exposure to secondary smoke Similar Past Episodes 24 Focused History & Physical Exam Physical Examination Inspection • Look for asymmetry, increased diameter, or paradoxical motion. Palpation • Feel for subcutaneous emphysema or tracheal deviation. Percussion 25 Focused History & Physical Exam Physical Examination (cont.) Auscultation • Normal Breath Sounds • Clear • Equal • Abnormal Breath Sounds • • • • Stridor Wheezing Rhonchi Rales/crackles 26 Focused History & Physical Exam Physical Examination (cont.) Extremities • Look for peripheral cyanosis. • Look for swelling and redness, indicative of a venous clot. • Look for finger clubbing, which indicates chronic hypoxia. 27 Focused History & Physical Exam Vital Signs Heart Rate • Tachycardia. Blood Pressure • Pulsus paradoxus. Respiratory Rate • Observe for trends. 28 Focused History & Physical Exam • Assume that an elevated respiratory rate in a patient with dyspnea is caused by hypoxia. A persistently slow rate indicates impending respiratory arrest. 29 Focused History & Physical Exam • Diagnostic Testing • Pulse Oximetry • Inaccurate readings 30 Focused History & Physical Exam • Other Diagnostic Testing • Peak Flow • Dextrose Monitoring??? 31 Management of Respiratory Emergencies Basic Principles • Maintain the airway. • Protect the cervical spine if trauma is suspected. • Patients breathing inadequately should be assisted with artificial ventilation. • Any patient with respiratory distress should receive oxygen. • Oxygen should never be withheld from a patient suspected of suffering from hypoxia. 32 Management of Respiratory Emergencies Basic Principles (cont.) All patients in respiratory distress are a priority transport. They have the potential to decline very rapidly. 33 What Kind of Respiratory Emergencies Might I Encounter??? 34 Upper-Airway Obstruction • Common Causes • Tongue, Foreign Matter, Trauma, Burns • Allergic Reaction, Infection • Assessment • Differentiate cause. 35 Upper-Airway Obstruction Management • Conscious Patient • If the patient is able to speak, encourage coughing. • If the patient is unable to speak, perform abdominal thrusts. • Determine if there is a complete obstruction or poor air exchange. • If either one is present, provide up to five abdominal thrusts in rapid succession. • If they fail, repeat until obstruction is relieved or patient becomes unconscious. 36 Upper-Airway Obstruction Management (cont.) • Unconscious Patient • Open the airway • Attempt to visualize obstruction • Attempt to give two ventilations. • If they fail, reposition the head and reattempt. • Begin CPR 37 Adult Respiratory Distress Syndrome • • • • • • • • • Sepsis Aspiration Pneumonia Pulmonary Injury Burns/Inhalation Injury Oxygen Toxicity Drugs High Altitude Hypothermia • • • • • • Near-Drowning Syndrome Head Injury Pulmonary Emboli Tumor Destruction Pancreatitis Invasive Procedures • Bypass, hemodialysis • Hypoxia, Hypotension, or Cardiac Arrest 38 Adult Respiratory Distress Syndrome Pathophysiology • High Mortality • Multiple Organ Failure • Affects Interstitial Fluid • Causes increase in fluid in the interstitial space • Disrupts diffusion and perfusion Assessment • Symptoms Related to Underlying Cause • Abnormal Breath Sounds • Crackles and rales 39 Adult Respiratory Distress Syndrome Management • Manage the underlying condition. • Provide supplemental oxygen. • Support respiratory effort. • Provide positive pressure ventilation if respiratory failure is imminent. • Monitor vital signs. 40 Obstructive Lung Disease Types • Emphysema • Chronic Bronchitis • Asthma Causes • Genetic Disposition • Smoking and Other Risk Factors 41 Emphysema • Pathophysiology • Exposure to Noxious Substances • Exposure results in the destruction of the walls of the alveoli. • Weakens the walls of the small bronchioles and results in increased residual volume. • Cor Pulmonale – hypertrophy of the right ventricle • Polycythemia – an excess of red blood cells • Increased Risk of Infection 42 Emphysema Assessment • History • Recent weight loss, dyspnea with exertion • Cigarette and tobacco usage • Lack of Cough 43 Emphysema Assessment • Physical Exam Barrel chest Prolonged expiration and rapid rest phase Thin Pink skin due to extra red cell production “Pink puffer” Hypertrophy of accessory muscles 44 Chronic Bronchitis Pathophysiology • Results from an increase in mucussecreting cells in the respiratory tree. • Alveoli relatively unaffected. • Decreased alveolar ventilation. Assessment • History • Frequent respiratory infections. • Productive cough. 45 Chronic Bronchitis Assessment (cont.) • Physical Exam • Often overweight • Rhonchi present on auscultation • Jugular vein distention • Ankle edema • Hepatic congestion • “Blue bloater” 46 Bronchitis and Emphysema Management • Establish and maintain airway. • Support breathing. • • • • Find position of comfort. Provide O2 Monitor oxygen saturation. Be prepared to ventilate. • Establish IV access. • Administer medications. 47 Asthma Pathophysiology • Chronic Inflammatory Disorder • Results in widespread but variable air flow obstruction. • The airway becomes hyperresponsive. • Induced by a trigger, which can vary by individual. • Trigger causes release of histamine, causing bronchoconstriction and bronchial edema. • 6–8 hours later, immune system cells invade the bronchial mucosa and cause additional edema. 48 Asthma Assessment • Identify immediate threats. • Obtain history. • SAMPLE & OPQRST history • History of asthma-related hospitalization? • History of respiratory failure/ventilator use? 49 Asthma Assessment (cont.) • Physical Exam • Presenting signs may include dyspnea, wheezing, cough. • Wheezing is not present in all asthmatics. • Speech may be limited to 1–2 consecutive words. • Look for hyperinflation of the chest and accessory muscle use. • Carefully auscultate breath sounds. 50 Asthma Management • Treatment goals: • Correct hypoxia. • Reverse bronchospasm. • Reduce inflammation. • Maintain the airway. • Support breathing. • High-flow oxygen or assisted ventilations as indicated. 51 Asthma Management (cont.) – Establish IV access. • Administer medications. Status Asthmaticus • A severe, prolonged attack that cannot be broken by bronchodilators. • Greatly diminished breath sounds. • Recognize imminent respiratory arrest. 52 Upper Respiratory Infection (URI) Upper Respiratory Infections • Frequent patient complaint. • Common pediatric complaint. • Rarely life threatening. Pathophysiology • Frequently caused by viral and bacterial infections. • Affect multiple parts of the upper airway. • Typically resolve after several days of symptoms. 53 Upper Respiratory Infection (URI) 54 Upper Respiratory Infection (URI) • Assessment • Look for underlying illness. • Evaluate pediatrics for epiglottitis. • Management • Maintain the airway. • Support breathing. • Treat signs and symptoms. 55 Pneumonia Infection of the Lungs • Immune-Suppressed Patients Pathophysiology • Bacterial & Viral Infections • Hospital-acquired vs. community-acquired. • Infection can spread throughout lungs. • Alveoli may collapse, resulting in a ventilation disorder. 56 Pneumonia Assessment • Focused History & Physical Exam • SAMPLE & OPQRST: • Recent fever, chills, weakness, and malaise • Deep, productive cough with associated pleuritic pain • Tachypnea and tachycardia may be present. • Breath sounds: • Presence of rales/crackles in affected lung segments • Decreased air movement in the affected lung 57 Pneumonia Management • Maintain the airway. • Support breathing. • High-flow oxygen or assisted ventilation as indicated. • Monitor vital signs. • Establish IV access. • Avoid fluid overload. 58 Lung Cancer General Pathophysiology • Majority are caused by carcinogens secondary to cigarette smoking or occupational exposure. • May start elsewhere and spread to lungs. • High mortality. Assessment • Focused History & Physical Exam • SAMPLE & OPQRST history • Cancer-related treatments and hospitalizations. • Physical exam • Evaluate for severe respiratory distress. Management • Follow general principles. • Administer oxygen, support ventilation. 59 Toxic Inhalation Pathophysiology • Includes inhalation of heated air, chemical irritants, and steam. • Airway obstruction due to edema and laryngospasm due to thermal and chemical burns. Assessment • Focused History & Physical Exam • SAMPLE & OPQRST history • Determine nature of substance. • Length of exposure and loss of consciousness. 60 Toxic Inhalation Management • Ensure scene safety. • Enter a scene only if properly trained and equipped. • Remove the patient from the toxic environment. • Maintain the airway. • Early, aggressive management may be indicated. • Support breathing & provide O2. • Establish IV access. • Transport promptly. 61 Carbon Monoxide Inhalation Carbon Monoxide • Odorless, Colorless Gas • Results from the incomplete combustion of carbon-containing compounds. • Often builds up to dangerous levels in confined spaces such as mines, autos, and poorly ventilated homes. • Hazardous to Rescuers 62 Carbon Monoxide Inhalation Pathophysiology • Binds to Hemoglobin • Prevents oxygen from binding and creates hypoxia at the cellular level. Assessment • Focused History & Physical Exam • SAMPLE & OPQRST history • Determine source and length of exposure. • Presence of headache, confusion, agitation, lack of coordination, loss of consciousness, and seizures. 63 Carbon Monoxide Inhalation Management • Ensure scene safety. • Enter a scene only if properly trained and equipped. • Remove the patient from the toxic environment. • Maintain the airway. • Support breathing. • High-flow oxygen or assisted ventilations as indicated. • Establish IV access. • Transport promptly. 64 Pulmonary Embolism Pathophysiology • Obstruction of a Pulmonary Artery • Emboli may be of air, thrombus, fat, or amniotic fluid. • Foreign bodies may also cause an embolus. • Risk Factors • Recent surgery, long-bone fractures, pregnancy. • Pregnant or postpartum. • Oral contraceptive use, tobacco use. 65 Pulmonary Embolism Assessment • Focused History & Physical Exam • SAMPLE & OPQRST history • Presence of risk factors • Sudden onset of severe dyspnea and pain • Cough, often blood-tinged • Physical exam • Signs of heart failure, including JVD and hypotension • Warm, swollen extremities 66 Pulmonary Embolism Management • Maintain the airway. • Support breathing. • High-flow oxygen or assist ventilations as indicated. • Establish IV access. • Monitor vital signs closely. • Transport to appropriate facility. 67 Spontaneous Pneumothorax • Pathophysiology • Pneumothorax • Occurs in the absence of blunt or penetrating trauma. • Risk Factors • Assessment • Focused History • • • • • SAMPLE & OPQRST history Presence of risk factors Rapid onset of symptoms Sharp, pleuritic chest or shoulder pain Often precipitated by coughing or lifting 68 Spontaneous Pneumothorax Assessment (cont.) • Physical Exam: • Decreased or absent breath sounds on affected side • Tachypnea, diaphoresis, and pallor Management • Maintain the airway. • Support breathing. • Monitor for tension pneumothorax. • JVD and tracheal deviation away from the affected side. 69 Hyperventilation Syndrome 70 Hyperventilation Syndrome Assessment • Focused History & Physical Exam • SAMPLE & OPQRST history • Fatigue, nervousness, dizziness, dyspnea, chest pain • Numbness and tingling in hands, mouth, and feet • Presence of tachypnea and tachycardia • Spasms of the fingers and feet 71 Hyperventilation Syndrome Management • Maintain the airway. • Support breathing. • Provide high-flow oxygen or assist ventilations as indicated. • Do NOT allow the patient to rebreathe exhaled air. • Reassure the patient. 72 Croup Pathophysiology • Infection of the larynx causing an upper airway obstruction. Assessment • • • • Children < 3 years of age. Low grade fever Slow onset Barky cough 73 Croup • Management • • • • Calm Patient Oxygen Cool Air Prepare for assist ventilations 74 Epiglottitis Pathophysiology • Infection and enflamation of the epiglottis causing an upper airway obstruction. Assessment • • • • Children > 3 years of age. High grade fever Rapid onset Drooling 75 Epiglottitis • Management • Calm Patient • Oxygen • Encourage sitting position • Prepare for assist ventilations 76 Prescribed Inhalers Generic Names: -albuterol -isoetharine -metaproteranol Trade Names: -Proventil -Ventolin -Bronkosol -Alupent -Metaprel 77 QUESTIONS ? 78