Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
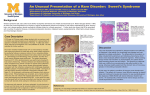
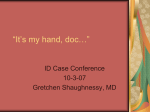
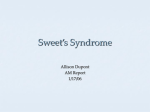
The case of the sassy blistering woman Andy J. Chien University of Washington Department of Medicine Division of Dermatology Introducing J.M. • ID: 65 yo F with two week history of “blisters” • Admitted initially to St. Joseph’s hospital, but then transferred to UWMC for further evaluation when KOH prep of blister fluid from heel showed hyphal elements • Blisters began on each heel, then progressed up the legs, and then involved the hands. Started as red spots, progressed to blisters and painful bumps. • 4-day history of eruption on the face • Blisters began 3 days after patient started furosemide for ankle edema • Cold-like symptoms occurred shortly before first blisters appeared • Review of systems unremarkable. No F/C/NS/wt loss. Excellent appetite. No arthralgias/myalgias. Organ-based ROS all negative. J.M.’s Past Medical History • Pyoderma gangrenosum since 2001– flares if prednisone < 20 mg/day. Had skin grafts in 2001 on legs. • “monoclonal gammopathy” of some type with recent bone marrow biopsy • HTN • Hyperlipidemia • Osteoporosis • Fibrocystic breast disease • Active 45 pack-year smoking history • S/P hysterectomy • H/O colonization with MRSA J.M.’s Medication History • • • • • • • • • • • • Allergies/Intolerances: codeine, diazepam Prednisone 20 mg qd Azathioprine 50 mg bid Furosemide 40 mg qd (started 17 days ago) Simvastatin Potassium chloride Premarin ASA Alendronate Alprazolam Celexa MVI Physical Examination • VS: T = 35.9o C, P = 106, BP = 111/67, RR = 20, SaO2 = 93% on RA • Gen: sassy elderly female lying in bed in NAD, interactions appropriate. • HEENT: anicteric, OP clear. • Neck: no masses/LAD. Normal JVP. • Abdomen: No masses, no HSM. • LN: No cervical, axillary or inguinal LAD. • Ext: No clubbing. Trace bilateral LE pitting edema. Good peripheral pulses. • Neuro: alert and oriented with no focal deficits noted. Physical Examination Physical Examination Physical Examination Physical Examination Physical Examination Laboratory and diagnostic studies • Chem 7: Na = 129, K = 3.4, Cl = 85, HCO3 = 25, BUN = 35, Cr = 1.1, Glu = 144 • CBC: WBC = 19.6 with neutrophils = 18.03 (92%), Hct = 34 (MCV 91) • Ca/Mg/Phos, LFTs, INR unremarkable • UA and urine culture normal • Blood cultures with no growth • Direct exam of blister fluid on left leg x 3 showed 2-4+ WBCs, no organisms. Bacterial, fungal and viral cultures negative. Viral FA negative. • CXR: emphysematous changes with no masses or infiltrates • EKG: NSR with RAD, LV hypertrophy by voltage criteria Differential diagnosis • • • • • Acute febrile neutrophilic dermatosis Pyoderma gangrenosum Drug reaction Cutaneous malignancy Infection secondary to immunosuppresion Histopathology “Right palm plaque” “Left leg bulla” Histopathology Differential diagnosis • • • • • Acute febrile neutrophilic dermatosis Pyoderma gangrenosum Drug reaction Cutaneous malignancy Infection secondary to immunosuppresion Sweet’s original report in 1964 • 8 female patients between 32 and 55 seen over 15 years • Patients were ill • One or more asymmetric erythmatous patches progressing to raised painful plaques (0.5-4 cm) • Some plaques gave the illusion of a “multiocular blister”, some had small central pustules • Active phase was 1-2 months depending on treatment with steroids • No scarring • No other physical exam abnormalities • Infection workups unrevealing • Five of eight had one or more recurrences • Neutrophilic infiltrates seen on pathology • Diff dx: erythema multiforme, erythema elevatum diutinum, pyoderma gangrenosum, erythema nodosum, bromide/iodide eruption • Postulated a steroid responsive reactive process • Martin Luther King wins the Nobel Peace Prize and the Civil Acts Right is signed by LBJ • The Palestine Liberation Organization is founded • Khruschev is deposed in Moscow and replaced by Brezhnev • Conflict in Vietnam escalates as US warships are attacked in the Gulf of Tonkin • Nelson Mandela given life sentence (but will be freed in 1990 and elected president of S. Africa in 1994) • Japan unveils the “bullet train” (130 mph top speed) • • • • • • • • “I Want To Hold Your Hand” tops the charts The Rolling Stones begin their first tour of the US The mini-skirt debuts and is a hit worldwide Sidney Poitier wins an Oscar for his performance in “Lilies of the Field” (Best picture? “Tom Jones”) Caldecott Medal awarded to Maurice Sendak for “Where the Wild Things Are” Cassius Clay wins the world heavyweight title Summer Olympics held in Tokyo, winter Olympics held in Innsbruck St. Louis beats the Yankees (4-3) for the World Series title (Bob Gibson is the MVP) Sweet’s syndrome • Fever • Neutrophil leukocytosis of the blood • Painful plaques/nodules on the limbs, face and neck – 0.5 – 12 cm in size, enlarge over days-weeks – red-purple in color – single or multiple, often asymmetric – can be bullous/vesicular in appearance • Histologically dense infiltrates with mature PMNs – usually infiltrate in superficial dermis, +/- eos and lymphs – can be diffuse or perivascular – papillary edema common – epidermis usually spared; occasional spongiosis, exocytosis, subcorneal pustule • No evidence of infection • Responds to corticosteroids Additional features of Sweet’s syndrome • • • • • • • • • • Pathergy – biopsy sites, trauma, radiation tx, sunburn Oral lesions – mucosal ulcers, swollen tongue Eyes – conjunctivitis, scleritis, iritis, glaucoma, hemorrhage Bones – arthralgias, aseptic osteomyelitis, aseptic osteitis, neutrophils in synovial aspirates CNS – aseptic meningitis, neuro sxs, central pareses, pysch sxs Liver – lab abnormalities Kidney – lab abnormalities Intestines – lower GI sxs Lungs – lesions on bronch, abnormalities on CXR Musculoskeletal – myalgias Clinical settings of Sweet’s syndrome • “Classic” Sweet’s syndrome • Malignancy-associated Sweet’s Syndrome (MASS) • Drug-induced Sweet’s syndrome Classic Sweet’s syndrome • • • • • • • F:M ~ 4:1 No racial preference Ages 30-50 (youngest reported 7 wks old) Idiopathic Infections (Strep - URI, Yersinia -GI) Pregnancy Inflammatory bowel disease Malignancy-associated Sweet’s syndrome • M=F • Incidence difficult to establish (7-56%). Cohen and Kurzrock reviewed 448 patients with Sweet’s; 20% had evidence of a solid or hematologic tumor • Hematologic malignancies: AML most common • Solid tumors: GU, breasts, GI tract Diagnostic criteria for classic Sweet’s or MASS Major criteria (both required) 1. Abrupt onset of painful erythematous plaques or nodules 2. Dense neutrophilic infiltrate (without evidence of LCV?) Minor criteria (two of four required) 1. Fever > 38o C 2. History of associated illness or malignancy 3. Response to treatment with potassium iodide or steroids 4. Three of four lab abnormalities: - WBC > 8000 - Neutrophils > 70% - ESR > 20 - Positive CRP Cohen PR and Kurzrock R, Clin Dermatol (2000) 18, 265-282 Su WP and Liu HN, Cutis (1986) 37, 167-174 Diseases reported in association with Sweet’s syndrome • • • • • • • • • • • • • • • AML Myelodysplasia CML Multiple myeloma Solid tumors (GU, GI and breast) Crohn’s Ulcerative colitis Rheumatoid arthritis SLE Thyroid disease (Grave’s, Hashimoto’s) Post-infection (bacterial, fungal, parasitic) Behcet’s Sarcoidosis Erythema nodosum Pregnancy Malignancies IBD Autoimmune Infection Other Drug-induced Sweet’s syndrome • F:M = 3:1 • G-CSF is big culprit • All-trans-RA, CBZ, hydralazine, OCPs, minocycline, nitrofurantoin, TMP-SMX • M.W. Cobb: JAAD 1989, “Furosemide-induced eruption simulating Sweet’s syndrome” – Clinical and histological features of Sweet’s syndrome, but no fever Diagnostic criteria for druginduced Sweet’s syndrome All five criteria required 1. 2. 3. 4. Abrupt onset of painful plaques or nodules Dense neutrophilic infiltrate (without evidence of LCV?) Fever > 38o C Temporal relation between drug onset and clinical onset OR temporally related recurrence after rechallenge with drug 5. Temporal relation between withdrawal of drug OR resolution with systemic corticosteroids Adapted from Cohen PR and Kurzrock R, Clin Dermatol (2000) 18, 265-282 and Walker DC and Cohen PR, J Am Acad Dermatol (1996) 34, 918-923 Clinical features in Sweet’s syndrome Classic Heme Malignancy Solid Tumor DrugInduced Epidemiology -Female -Prior URI/GI infxn. -Recurrence 80 75-90 30 50 (33/66) 16 (11/69) 69 (37/54) 59 20 41 71 21 67 Symptoms -Fever > 38C -Musculosk. involv. -Ocular involv. 80-90 12-56 17-72 88 (50/57) 26 (18/69) 7 (5/69) 79 34 15 100 21 21 Lesion locations -Upper extrem. -Head/neck -Trunk/back -Lower extrem. -Oral mucous memb. 80 50 30 Infreq. 2 89 (58/65) 63 (41/65) 42 (27/65) 49 (32/65) 12 (8/65) 97 52 33 48 3 71 43 50 36 7 Lab findings -Neutrophilia -Elev. ESR -Anemia -Abnormal renal fxn. 80 90 Infreq. 11-50 47 (29/62) 100 (25/25) 68 (40/49) 15 (10/69) 60 95 50 7 38 100 50 0 Adapted from Cohen PR and Kurzrock R, Clin Dermatol (2000) 18, 265-282 Vasculitis and the histopathology of Sweet’s syndrome • 28 biopsy specimens from 21 patients satisfying diagnostic criteria for Sweet’s syndrome (classic or MASS) • Vasculitis: fibrinoid necrosis and intramural inflammation • Vasculitis as defined found in 6/28 specimens (21%) • Evidence of RBC extravasation and intramural inflammatory cells seen in 21/28 specimens (79%) • Specimens with vasculitis examined by IF for presence of IgG, IgM, IgA and C3 with appropriate controls • No immune complex deposition detected with Sweet’s samples • Proposal: vasculitis can be seen as an epiphenomenon in Sweet’s syndrome Malone JC et al., Arch Dermatol (2002) 138, 345-349. Pathogenesis of Sweet’s syndrome ? The non-infectious neutrophilic dermatoses • • Non-angiocentric – Psoriasis – Reiter’s syndrome – Subcorneal pustular dermatosis (Sneddon-Wilkinson) – Acne fulminans – Neutrophilic eccrine hidradenitis – Blastomycosis-like pyoderma (pyoderma vegetans) Angiocentric – Vessel wall destruction (leukocytoclastic vasculitis, polyarteritis nodosa) – No vessel wall destruction • Acute febrile neutrophilic dermatosis (Sweet’s) • Pyoderma gangrenosum • Behcet’s disease • Pustular vasculitis • Bowel-associated dermatosis-arthritis syndrome (BADAS) • Rheumatoid neutrophilic dermatosis • Pyostomatitis vegetans • Pustular eruption of ulcerative colitis • Neutrophilic dermatosis of the dorsal hand • Familial Mediterranean fever Overlapping of the neutrophilic dermatoses Sweet’s Clin. Appear. PG papules nodules ulcers Pathergy yes yes Oral involv. ulcers ulcers Eye involv. conjunctivitis Iritis, scleritis Joint involv. arthritis Associations Histopath heme malig. IBD e. nodosum sarcoid thyroid dz. RA SLE Behcet’s superficial dermis Sned-Wilk Behcet’s papules nodules ulcers, Sweet’s-like, PG-like -- -- yes -- -- ulcers keratitis, vasculitis -- keratitis, vasculitis uveitis, vasculitis arthritis arthritis arthritis arthritis heme malig. IBD heme malig. IBD e. nodosum heme malig. IBD e. nodosum sarcoid thyroid dz. RA SLE Behcet’s ulcer pustules EED heme malig. thyroid dz. RA SLE PG subcorneal pustules RA PG Sweet’s, PG sup/mid dermis LCV LCV IL-17 Stem cell IL-3 CFU-GEMM CFU-GM IL-6 GM-CSF all-trans retinoic acid CFU-G myeloblast T MP G-CSF promyelocyte myelocyte metamyelocyte B N E KC band IgG Phagocytosis C3b IL-8 C5a LTB4 PAF fMLP Chemoattractants and chemotaxis IL-1 IL-2 TNFa G-CSF GM-CSF Neutrophil activators Classic chemoattractant g Ga Ras GTP b GTP PLC IP3 DAG Ca PKC PI3K Raf Rho Adhesion, chemotaxis, ROS MEK Rac cPLA2 MAPK AA Adhesion, ROS Adapted from Burg ND and Pillinger MH (2001) Clin Immunol 99, 7-17 Adhesion, transcription, aggregation Membrane ruffling, ROS Adhesion CD11/CD18 b1 integrin L-selectin PECAM IL-8 C5a LTB4 PAF fMLP IgG Phagocytosis C3b 12-HETE Keratinocytes Chemoattractants and chemotaxis IL-1 IL-2 TNFa G-CSF GM-CSF Neutrophil activators b1 and b2 integrins 3. infiltration E and P selectin PECAM ICAM 2. transmigration 1. “rolling” sialyl Lewis X CD11/CD18 (LAD) Adapted from Von Den Driesch (2000) Clin Dermatol 18, 233-244 Adhesion CD11/CD18 b1 integrin L-selectin IL-8 C5a LTB4 PAF fMLP IgG Phagocytosis C3b Enzymatic destruction -cathepsins -azurocidins/defensins -elastases -lysozymes -phospholipases -glycosidases PECAM Reactive oxygen species (NADPH oxidase) Chemoattractants and chemotaxis IL-1 IL-2 TNFa G-CSF GM-CSF Neutrophil activators IgG Phagocytosis C3b Interference with phagocytosis: dapsone Adhesion CD11/CD18 L-selectin b1 integrin PECAM Interference with integrin-mediated adhesion: -corticosteroids -dapsone Interference with Chemotaxis: - potassium iodide - colchicine - tetracycline IL-8 C5a LTB4 PAF fMLP Inhibtion of TNFa: thalidomide Chemoattractants and chemotaxis IL-1 IL-2 TNFa G-CSF GM-CSF Neutrophil activators Inhibits secretion of neutrophil lysosome: - colchicine Enzymatic destruction -cathepsins -azurocidins/defensins -elastases -lysozymes -phospholipases -glycosidases Reactive oxygen species (NADPH oxidase) Scavenge ROS: -dapsone Inhibit generation Of ROS: -thalidomide -tetracycline -erythromycin -metronidazole -sulfasalazine (also induces PMN apoptosis) Scientific advances since 1964 • • • • • • • • • • • • • First beta-blocker synthesized (propranalol, 1964) First human heart transplant (1967) Restriction endonucleases discovered (1968) Interleukin-1 is identified (1972) Acyclovir is developed (1972) Computer assisted tomography invented (1973) DNA sequencing is developed (1977) In vitro fertilization is accomplished (1978) Polymerase chain reaction developed (1983) HIV identified (1984) Dolly is cloned (1996) Human genome working draft is completed (2000) Fleckman declares pathogenesis of Sweet’s still unclear (2002) Treatment of Sweet’s syndrome • Spontaneous resolution – 4/8 of women in Sweet’s original report – 9 published reports from 1964-1997 – 33/208 (16%) with spontaneous resolution • Cure underlying condition – infection, cancer • Discontinue offending medications • No randomized control trials exist for documenting the effectiveness of pharmacologic interventions Corticosteroids • Still the treatment of choice • Systemic: – 0.5-1.5 mg/kg/day average from a dozen studies – Tapered over 1 – 12 weeks – Pulsed methylprednisolone 250 – 1000 g/day x 3 days • Topical: – Fluocinonide, diflorasone – Primary or adjuvant therapy • Intralesional: – TAC at 3 – 10 mg/cc • ACTH Other therapeutic agents • Potassium Iodide (>10 reports/series) – 300 - 950 mg/day • Colchicine (5 reports/series) – 1 – 1.5 mg qd/qod • Cyclosporine (5 case reports/series) – 2 – 10 mg/kg/day • NSAIDS (8 reports/series) – Indomethacin, 150 – 750 mg qd/qod – Not always useful Other therapeutic agents • Antimicrobials – Tetracycline class – Antimicrobials implicated in drug-induced Sweet’s • Sulfones (9 reports/series) – Dapsone 100 – 200 mg qod – Sulfapyridine also used for IBD • Infliximab – Crohn’s disease Less exciting, but somebody tried it • Salicylates • Clofazimine – 200 mg qd x 4 wks, then 100 mg qd x 4 wks – Enhances PMN phagocytic activity – Red-gray skin pigmentation, drug-related icthyosis • Etretinate – Good response in patient with agnogenic myeloid metaplasia • IFN-alpha – Systemic and IL in patient with CML • Danazol • Pentoxifylline • Antihistamines • Cytotoxic agents – AZA, MTX, cyclophosphamide, chlorambucil • • • • • • • • Derm residents: ova awaiting fertilization. Dank: alas, also just an unfertilized ovum. Kuechle: learning to walk, awaiting first ballet lesson. Sidbury: learning to walk, soon to be forced by older brother to play basketball left-handed. Hornung: in a Southern California grocery store, asking her mother when she was going to turn four. Kern: cynical New York second-grader. Kirby: starting high school in Seattle. Milner: dreaming of Bonaparte and waiting to start his residency in dermatology at the UW • Iwamoto: skiing in Switzerland and miserably trying to learn Swiss-German while speaking only Japanese. • Berg: having a smashing time as a three year-old in London, not yet planning on a career in medicine. • Lantz: happy 4-year old Republican in Vancouver, Washington • Argenyi: going through sixth grade in Budapest, Hungary, insisting that he was a “very well-behaved boy”. • Colven: pimping fellow pre-schoolers on “Mother Goose Nursery Rhymes” reading assignment. • Sybert: starting tenth grade, fending off would-be suitors, and falling in love with Mr. Zaccaro, the social studies teacher. • Still a virgin… • Fleckman: demonstrating with Mario Savio (1942-1996) and the Free Speech Movement at Berkeley, birthplace of the “sit-in”. During 1964, a skeptical young Phil develops a distrust of news media coverage. • Olerud: awarded first of two team MVP awards, one year before being awarded “John Olerud Award” and First Team AllAmerican. Courting future Mrs. Olerud. • Raugi: about to start senior year of high school with abundant hair on both head and legs, doing research for $1.25/hour at Palo Alto, trying to figure out where Vietnam was, developing a passion for golf, disdaining Beatlemania, and spending countless hours watching… • …BULLFIGHTING FROM TIJUANA?!? Acknowledgments • Phil Fleckman • Bob Underwood Selected References • • • • • • • • • Burg, ND and Pillinger, MH (2001) “The neutrophil: function and regulation in innate and humoral immunity” Clin Immunol 99, 7-17. Callen, JP (2002) “Neutrophilic dermatoses” Dermatol Clin 20, 409-419. Cohen, PR and Kurzrock, R (2000) “Sweet’s syndrome: a neutrophilic dermatoses classically associated with acute onset and fever” Clin in Dermatol 18, 265-282. Cohen, PR and Kurzrock, R (2002) “Sweet’s syndrome: A review of current treatment options” Am J Clin Dermatol 3, 117-31. Cronstein et al. (1992) “A mechanism for the antiinflammatory effects of corticosteroids: the glucocorticoid receptor regulates leukocyte adhesion to endothelial cells and expression of ELAM-1 and ICAM-1” Proc Natl Acad Sci USA 89, 9991-9995. Miyachi, Y (2000) “Pharmacologic modulations of neutrophils” Clin in Dermatol 18, 369-373. Schroder, J-M (2000) “Chemoattractants as mediators of neutrophilic tissue recruitment” Clin in Dermatol 18, 245-263. Sweet, RD (1964) “An acute febrile neutrophilic dermatosis” Br J Dermatol 79, 351-356. Von Den Driesch, P (2000) “Polymorphonuclears: Structure, function and mechanisms of involvement in skin disease” Clin in Dermatol 18, 233-44.