Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
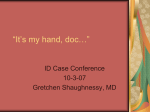
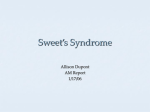
A CASE OF RASH…A HARBINGER OF MORE SERIOUS ILLNESS? CASSIE HAJEK, MD SANFORD ADULT MEDICINE S E P T E M B E R 1 3 TH, 2 0 1 3 32-YEAR-OLD WOMAN WITH RASH • CC: Rash • 32-year-old woman who presented with a rash that started 5 days earlier. • She noted a tender bump on the right lower leg and thought she had bumped her leg. Over the next couple of days, she began to acquire more lesions on the lower legs. • 24-48 hours after the initial tender nodule on the leg, she started to notice lesions on her shoulders and upper trunk. These had more of a sunburn kind of quality to them. • She was out on the deck a few nights before she developed the lesions on the upper trunk, but did not recall getting any insect bites, and the lesions were not itchy • The rash progressed for 2 days, then stabilized • The lesions on the lower legs remained tender, but this improved with ibuprofen. • 2 days after the onset of the rash, she was seen in acute care and started on triamcinolone 0.5% cream which she applied to the lesions on the upper trunk with some relief • She was recently exposed to mycoplasma, but denies any other exposures. ROS • • • • • • • • • • • • Constitutional: No unexpected change in weight, no fatigue, no fevers, sweats or chills. HEENT: Eye: No recent significant change in vision, no eye pain, redness, or discharge. Nose: She had a mild runny nose and cold-type symptoms approximately 6 weeks earlier Ear: No ear pain, no tinnitus or vertigo, no recent change in hearing. Mouth/Throat: No sore throat, no difficulty swallowing, no recent change in voice or hoarseness. Neck: No lumps or masses, no swollen glands, no recent swelling in thyroid area, no significant pain in neck. Pulmonary: No chronic cough, sputum, or hemoptysis, no dyspnea on exertion, no wheezing, no shortness of breath Cardiovascular: No orthopnea, no chest pain, no diaphoresis, no edema, no palpitations, no claudication symptoms. Gastrointestinal: chronic on/off diarrhea - seems to be correlated with stress and nervousness, no abdominal pain, no melena, no hematochezia, no significant change in appetite, no nausea or vomiting Musculoskeletal/Extremities: mild generalized arthralgias, no noted joint swelling or redness. Heme/Allergy/Immune: No abnormal bleeding, no bruising, no night sweats, no history of DVT. Skin/Integumentary: as mentioned in HPI Neurologic: No chronic headaches, no seizures, no weakness, no numbness or tingling. Psychiatric: No depression, no anxiety, no psychosis. Endocrine: Negative for polydipsia, dry mouth, polyuria, and heat or cold intolerance. GU: Denies abnormal vaginal bleeding, discharge or unusual pelvic pain, no dysuria, frequency or hematuria ADDITIONAL HISTORY Past Medical History: negative Past Surgical History: negative Medications: Nuvaring –discontinued one week prior to presentation Allergies: NKDA Family Medical History: • Mother – gastric adenocarcinoma • There is no known family history of any other cancer, connective tissue disease, inflammatory bowel disease Social History • Married • Works as a nurse in the intensive care unit • Occasional alcohol use and no tobacco or illicit drug use PHYSICAL EXAM • Vital signs: T = 97.8, P = 76, R = 14, BP = 104/72 • General: well-appearing woman in no acute distress • HEENT: Pupils are round and react to light. There is no eyelid pallor. Tympanic membranes are clear. Pharynx is moist and non-erythematous. Neck: Trachea is midline. There is no thyromegaly. • Lymph: There is no cervical, supraclavicular, groin or axillary adenopathy • Heart: Regular rate, no obvious murmur. PMI is not displaced. • Lungs: Lungs are clear to auscultation and percussion. • Abdomen: Abdomen is soft. Positive bowel sounds. No bruits, no masses. • Extremities: Strong pulses without edema. • Neurologic: Range of motion in the neck is appropriate. Peripheral sensation appropriate to light touch. • Musculoskeletal: Mild tenderness to palpation in bilateral elbows, no joint swelling or erythema; other joints WNL • Skin: • • Upper arms, shoulders, upper back and chest had several pink, pseudo-vesicular lesions with some that were slightly lighter centrally with erythema at the periphery but no targetoid lesions Bilateral lower extremities: numerous dull, erythematous, tender, indurated papules and nodules. No ulceration is appreciated. No surrounding induration or impressive erythema RASH DIAGNOSTIC TESTING • • • • • • • • • • • CBC: WNL CMP: WNL ESR: WNL CRP: WNL Rapid strep with reflex culture: negative ASO titer: negative ANA screen: negative HIV: negative Mycoplasma titers: negative Peripheral smear: normal UA: negative BIOPSY RESULTS • Leg: • Dermatitis with minimal spongiosis, focal lichenoid change and vacuolar cell change with extravasated red blood cells • Biopsy lacked subcutaneous tissue component to evaluate for erythema nodosum. • Back: • Neutrophilic dermatitis • Consistent with Sweet’s syndrome SWEET’S SYNDROME DEFINITION • Acute febrile neutrophilic dermatosis • Described by Robert Sweet in 1964 • Characterized by erythematous plaques, nodules, or papules accompanied by fever, malaise, or arthralgias • Biopsy contains diffuse infiltrate of neutrophils in the papillary dermis • Female predominance SWEET’S SYNDROME THREE SUBTYPES • Classic (idiopathic) • Sudden onset of the typical skin findings and histopathology without associated vasculitis • Associated symptoms may include fever, preceding infection, arthralgia, or conjunctivitis • Lab findings can include leukocytosis or elevated ESR • Malignancy-associated • Acute myelogenous leukemia – most common hematologic malignancy • Genitourinary tumors – most common solid tumor • Suspected with consistent constitutional symptoms or family history • Drug-induced • Temporal relationship between drug ingestion and onset of symptoms • Granulocyte-colony stimulating factor and trimethoprimsulfamethoxazole SWEET’S SYNDROME DIAGNOSTIC CRITERIA Major Criteria 1. Abrupt onset of tender or painful erythematous or violaceous plaques or nodules 2. Predominantly neutrophilic infiltration in dermis without leukocytoclastic vasculitis Minor Criteria 1. Preceding fever or infection 2. Association with malignant lesion, pregnancy, inflammatory bowel disease, upper respiratory or gastrointestinal infection 3. Good response to systemically administered corticosteroids and not to antibiotics 4. Abnormal lab values: elevated ESR, leukocytosis Presence of 2 Major and 2 Minor criteria establish the diagnosis SWEET’S SYNDROME TREATMENT AND PROGNOSIS • Classical • • • • • • • • • • Systemic corticosteroids for diffuses disease Intralesional/topical corticosteroids for limited disease Improvement begins within 48 hours of treatment Resolution in 1-2 weeks May require taper over several weeks Drug-induced – discontinue offending agent Malignancy-associated – treat underlying malignancy Spontaneous resolution possible in weeks to months Skin lesions generally resolve without scarring Recurrence occurs in ~30% of patients BACK TO OUR PATIENT… • CT Chest/Abdomen/Pelvis: Inflammatory bowel changes involving the terminal ileum with two areas of stricture present, mild diffuse fatty infiltration of the liver with no large lymph nodes seen, minimal mesenteric fat stranding present • Colonoscopy with ileal biopsy: ileocolonic mucosa demonstrated architectural distortion, mixed lymphoplasmacytic inflammation with ulceration, and acute inflammation that was felt consistent with idiopathic inflammatory bowel disease • EGD: negative FINAL DIAGNOSIS AND OUTCOME • Sweet’s Syndrome secondary to underlying Crohn’s disease • Patient initially refused systemic steroids as she did not want them to affect her colon biopsy • After colon biopsy, she was started on budesonide and azathioprine with significant improvement of her chronic diarrhea • Skin manifestations gradually resolving ANY QUESTIONS? REFERENCES • Cohen P. Sweet’s Syndrome – a comprehensive review of an acute febrile neutrophilic dermatitis. Orphanet Journal of Rare Disease. 2007; 2:34 • Rochet N, Chavan R, Cappel M, Wada D, Gibson L. Sweet syndrome: Clinical presentation, associations and response to treatment in 77 patients. J Am Acad Derm. 2013; 10:1-8 SWEET’S SYNDROME EXTRACUTANEOUS MANIFESTATIONS • • • • • • • • • • • • Bone - Acute sterile arthritis, arthralgias, focal aseptic osteitis, pigmented villonodular synovitis, sterile osteomyelitis Central nervous system - Acute benign encephalitis, aseptic meningitis, brain SPECT abnormalities, brain stem lesions, cerebrospinal fluid abnormalities, computerized axial tomography abnormalities, electroencephalogram abnormalities, encephalitis, Guillain- Barre syndrome, idiopathic hypertrophic cranial pachymeningitis, idiopathic progressive bilateral sensorineural hearing loss, magnetic resonance imaging abnormalities, neurologic symptoms, "neuro-Sweet disease", pareses of central origin, polyneuropathy, psychiatric symptoms Ears - Tender red nodules and pustules that coalesced to form plaques in the external auditory canal and the tympanic membrane Eyes - Blepharitis, conjunctival erythematous lesions with tissue biopsy showing neutrophilic inflammation, conjunctival hemorrhage, conjunctivitis, dacryoadenitis, episcleritis, glaucoma, iridocyclitis, iritis, limbal nodules, ocular congestion, periocular swelling, peripheral ulcerative keratitis, retinal vasculitis, scleritis, uveitis Kidneys - Mesangiocapillary glomerulonephritis, urinalysis abnormalities (hematuria and proteinuria) Intestines - Intestine with extensive and diffuse neutrophilic inflammation, neutrophilic ileal infiltrate, pancolitis (culturenegative) Liver - Hepatic portal triad with neutrophilic inflammation, hepatic serum enzyme abnormalities, hepatomegaly Heart - Aortic stenosis (segmental), aortitis (neutrophilic and segmental), cardiomegaly, coronary artery occlusion, heart failure, myocardial infiltration by neutrophils, vascular (aorta, bracheocephalic trunk and coronary arteries) dilatation Lung - Bronchi (main stem) with red-bordered pustules, bronchi with neutrophilic inflammation, pleural effusion showing abundant neutrophils without microorganisms, progressive pharyngeal mucosal infiltration and edema resulting in upperairway obstruction, and chest roentgenogram abnormalities: corticosteroid-responsive culture-negative infiltratives, pulmonary tissue with neutrophilic inflammation Mouth - Aphthous-like superficial lesions (buccal mucosa, tongue), bullae and vesicles (hemorrhagic: labial and gingival mucosa), gingival hyperplasia, necrotizing ulcerative periodontitis, nodules (necrotic: labial mucosa), papules (macerated: palate and tongue), pustules (individual and grouped: palate and pharynx), swelling (tongue), ulcers (buccal mucosa and palate) Muscles- Magnetic resonance imaging (T1-weighted and T2-weighted) abnormalities: high signal intensities due to myositis and fasciitis, myalgias (in up to half of the patients with idiopathic Sweet's syndrome), myositis (neutrophilic), tendinitis, tenosynovitis Spleen – Splenomegaly