Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
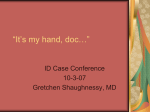
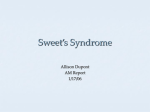
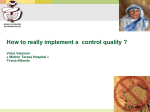
An Unusual Presentation of a Rare Disorder: Sweet’s Syndrome Anjan Chakrabarti MD , Diane Hall MD , Francis J. McBee Orzulak MD 1 Department of Internal Medicine, University of Michigan, Ann Arbor 2 Department of Pathology, University of Michigan, Ann Arbor 3 Department of Pediatrics and Communicable Diseases, University of Michigan, Ann Arbor 1 2 1,3 Background Sweet’s Syndrome (SS, also called acute febrile neutrophilic dermatosis) was initially characterized by Dr. Robert Douglas Sweet in 1964, at which time it was described as an eruption of painful erythematous plaques and nodules; it was further characterized by fever, leukocy1 tosis, and a dense papillary dermal neutrophilic infiltrate evident on a biopsy specimen . Further study has shown that SS is associated with a number of systemic illnesses, including hematopoietic disorders, malignant lesions, paraproteinemia, inflammatory bowel disease 2 and rheumatologic disease . a. b. 200x c. Figure 1 (left): violaceous bullous nodule on an erythematous base as seen in this patient Case Description A 20 year old Chinese male college student with no previous medical history was being treated as an outpatient for a presumptive diagnosis of cellulitis and abscesses of his legs. A CBC was drawn which returned a hemoglobin of 6.0 and platelets of 33,000. He was admitted for further work-up. Figure 2 (below): features of the RCMD subtype of MDS in the bone marrow biopsy of this patient are demonstrated by pelgeroid neutrophils (a, black arrow), dimorphic red cells (a, red arrow), erythrodysplasia (b, arrow), ringed sideroblasts (c, arrow), and dysplastic megakaryocytes (d, arrows) His exam revealed multiple tender 2-4 cm subcutaneous nodules with overlying erythema on both legs which were initially thought to be erythema nodosum raising a concern for an underlying illness. These nodules eventually developed into bullous lesions (see figure 1). Dermatology and Hematology were consulted, and skin and bone marrow biopsies were performed. The patient developed fevers and CT of the abdomen/pelvis was performed showing diffuse colonic thickening. Infectious Disease and Gastroenterology were consulted due to further concern for sepsis and/or inflammatory bowel disease. Bone marrow biopsy demonstrated features consistent with the refractory cytopenia with multilineage dysplasia (RCMD) subtype of myelodysplastic syndrome (MDS - see figure 2) and skin biopsy showed nonspecific neutrophilic infiltration (see figure 3). He underwent colonoscopy with biopsies which were entirely normal. Rheumatology was consulted, and a myriad of labs were sent; the only values that returned abnormal were a positive lupus anticoagulant and elevated ESR/CRP. At this point the case was discussed with all involved consultants and decision was made to treat with steroids while waiting for infectious workup to return. He improved with steroids: his fevers subsided, his skin lesions improved, and his blood counts remained stable but did not recover. He was discharged with a diagnosis of SS and myelodysplastic syndrome and follow-up with various consultants. 1000x 1000x 1000x 400x 20x Figure 3 (left): composite of skin biopsy for this patient at low magnification (a) shows most neutrophilic activity at the level of the deep dermis and subcutaneous tissue; higher magnifications (b and c) demonstrate neutrophilic infiltration at these levels 400x Discussion This case illustrates the potential for delayed treatment and difficulty of diagnosis in the setting of a complicated rare disease and management by multiple consultants. The differential for this patient, initially, included both autoimmune and infectious phenomena, which tend to have drastically different treatment regimens. While awaiting biopsy results and evaluation by subspecialists, this patient developed worsening fevers and skin lesions. The decision to initiate steroids was a difficult one considering the side effect profile for this young, otherwise healthy patient and the inherent risks of immunosupression in the setting of possible infection. In this case, the patient’s condition did improve once steroids were initiated. The patient did, however, have difficulty weaning his steroid dose and continued to develop skin lesions; he was eventually given the diagnosis of MDS-RCMD with steroid refractory Sweet’s Syndrome. He subsequently underwent bone marrow biopsy and had overall improvement in his condition. References Sweet RD. An acute febrile neutrophilic dermatosis. Br J Dermatol 1964;76:349-356 2 Fett DL, Gibson LE, Su WP. Sweet’s Syndrome: Systemic Signs and Symptoms and Associated Disorders. Mayo Clin Proc. 1995;70:234-240 1