Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
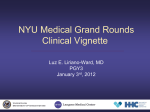
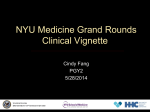
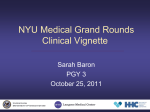
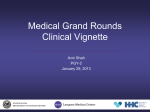
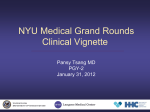
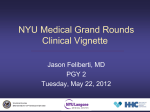
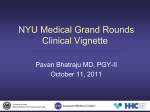
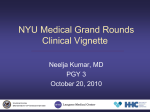
NYU Medical Grand Rounds Clinical Vignette Ramin S Hastings, MD PGY-3 September 8, 2010 UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Chief Complaint • 47 year old male presents with chest pain for two days UNITED STATES DEPARTMENT OF VETERANS AFFAIRS History of Present Illness • Mr. R is a 47 year old male with asthma and hypertension who was in his usual state of good health with a baseline exercise tolerance of fifteen blocks, until two days prior to admission when he developed new onset chest pain while lying down before going to bed. •The patient stated the pain was a substernal pressure, as if “someone was trying to push my heart through my back.” •The pain was non-radiating, and associated with mild shortness of breath, nausea, and diaphoresis. It resolved on its own after ten minutes. UNITED STATES DEPARTMENT OF VETERANS AFFAIRS History of Present Illness • He went to sleep, and the following day was free of symptoms until that night when a similar attack of chest pain occurred, again lasting about ten minutes. • On the day of admission he was at work, again not exerting himself, when he developed similar chest pain. • The pain lasted fifteen minutes, and he was drenched in sweat. He then decided to present to the emergency room for care. UNITED STATES DEPARTMENT OF VETERANS AFFAIRS History of Present Illness •On arrival to the emergency room, he was chest pain free, without complaint UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Additional History •Past Medical History: • Asthma – diagnosed in childhood, never intubated, approximately two exacerbations per year • Hypertension – diagnosed 5 years ago poorly controlled •Past Surgical History: • Right hand fracture repair after motor vehicle accident (10 years ago) •Social History: • Smokes one to two packs of cigarettes per day for the past 30 years, previously heavy alcohol and cocaine abuse, quit three years ago • Currently homeless and living in a shelter, works at a deli •Family History: •Adopted and does not know family history well •Allergies: • No known drug allergies •Medications: • Albuterol metered dose inhaler, 2 puffs as needed • Fluticasone 220 mcg 1 puff every 12 hours • Nifedipine 30 mg three times a day (however patient was not taking) UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Physical Examination •General: Obese African American male lying in stretcher in no acute distress •Vital Signs: T: 97.1 BP: 198/112 HR: 94 RR: 16 and O2 sat: 98% •Remainder of Physical Exam was normal UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Laboratory Findings •CBC: White Blood Cell Count 11.5 •Remainder of CBC was within normal limits •Basic Metabolic panel: Glucose 106 •Remainder of basic was within normal limits •Hepatic panel: within normal limits •Troponin 0.170 (normal 0.08) UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Initial EKG UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Other Studies •Electrocardiogram: Normal sinus rhythm at 70 beats per minute, normal axis, normal intervals, T-wave inversions in leads II/III/Avf and V3-V6, Left Ventricular Hypertrophy, no ST segment changes •Chest X-Ray: no consolidations, no pulmonary edema UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Differential Diagnosis • Acute coronary syndrome • Demand ischemia in the setting of uncontrolled hypertension UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Hospital Course • Hospital Day 1: – Patient was started on aspirin, clopidogrel, heparin, and simvastatin – His blood pressure was controlled with calcium channel blockers – Trans-thoracic echocardiogram was performed showing: • Concentric left ventricular hypertrophy • Normal left ventricular ejection fraction • Normal left ventricular wall motion UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Hospital Course • Hospital Day 2: – Nuclear pharmacologic stress test was performed showing: • No evidence of vasodilator-induced ischemia or decreased coronary artery flow reserve • No evidence of prior myocardial infarction • Normal wall motion and thickening with left ventricular ejection fraction of 54% – Given the normal echocardiogram and stress test the plan was to obtain a coronary computerized tomography angiography on the following day UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Hospital Course • Hospital Day 3: – The patient had been chest pain free until this day, when he developed severe chest pain much like his prior episodes – Electrocardiogram was repeated UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Repeat EKG UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Hospital Course • Hospital Day 3 Continued: – He was treated with nitroglycerin with relief of the pain and normalization of the findings on electrocardiogram – He was admitted to the Coronary Care Unit and emergently brought to the catheterization laboratory UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Cardiac Catheterization UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Hospital Course • Hospital Day 3 Continued: – Cardiac catheterization revealed: • A 90% lesion was noted in the proximal left anterior descending artery • A Promus stent was placed – Post-catheterization care was performed in the coronary care unit where he remained chest pain free • Hospital Day 5: – The patient was discharged from the hospital UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Final Diagnosis • Atherosclerotic heart disease with acute coronary syndrome UNITED STATES DEPARTMENT OF VETERANS AFFAIRS