Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
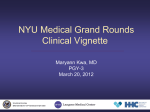
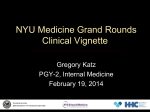
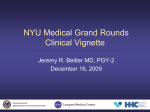
NYU Medical Grand Rounds Clinical Vignette Pavan Bhatraju MD, PGY-II October 11, 2011 UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Chief Complaint • 38 y/o M Firefighter presented 13 days after the 9/11 World Trade Center attack with 2 days of • • • • • myalgias fever dry cough pleuritic chest pain progressive dyspnea with minimal exertion UNITED STATES DEPARTMENT OF VETERANS AFFAIRS History of Present Illness •Usual state of good health when he arrived at the World Trade Center terrorist attack 20 minutes after the first tower collapsed •Worked 16 hr days and did not use respiratory protection for 10 of 13 days UNITED STATES DEPARTMENT OF VETERANS AFFAIRS History of Present Illness • 11 days PTA he developed a productive cough with blackish sputum that self-resolved in one day • 2 days PTA he developed, cough, fever, myalgias, anterior pleuritic chest discomfort, and dyspnea on exertion with less than one block UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Additional History •Past Medical and •None •Surgical History •None •Social History: •Smoking – 5 pack year history, stopped 20 years ago •Family History: •Non-contributory •Allergies: •None •Medications: •none UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Physical Examination •General: muscular adult male, diaphoretic, in moderate distress •Vital Signs: • T:38.6 BP:130/90 HR:120 • O2 sat: 90% on room air RR:35 •Pulmonary: accessory muscle use, bibasilar decreased breath sounds •Remainder of Physical Exam was Normal. UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Laboratory Findings •CBC: •WBC – 22,600 cells/mm3, • Differential (N = 91%, L = 3% M = 5% E = 1%) •Remainder of CBC was within normal limits •Basic Metabolic panel and Hepatic Panel: •Within normal limits •Arterial Blood Gas on Room Air: •pH 7.46 •paO2 53 mmHg •paCO2 32 mmHg •HC03 23 mEq/L •O2 sat 89% UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Other Studies •Chest X-Ray and CT Scan: • Patchy ground glass opacifications • Thickening of respiratory airways • Bilateral pleural effusions. UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Differential Diagnosis • Lung Injury – Dust Induced – Infection Related • Bioterrorism induced Pneumonia (Anthrax) UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Hospital Course • Hospital Day 1: – He was admitted to the MICU and treated with • oxygen • levofloxacin • methylprednisolone – Bronchoalveolar Lavage - 730,000 cells/ml (normal <250,000 cells/ml) • Differential E = 70%, M = 18%, L = 8% N = 4% – Total IgE was 58 ng/ml (normal <180 ng/ml) – BAL fluid IgE was 0.4 ng/ml UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Asbestos Si Elemental Analysis Mg Fe Ca Glass Au Fly Ash Hospital Course • Hospital Day 9: – Clinically improved with repeat CT showing near complete resolution. – He was discharged with 3 weeks of corticosteroid therapy • Pulmonary Function Tests: • • • • • FEV1 = 2.6 L (71%) FVC = 3.8 L (86%) FEV1/FVC = 68% DLCO = 23.1 ml/mmHg/min (77%) His oxygen saturation at rest (94%) dropped to 87% after a brisk walk of 150 ft. UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Post-Discharge • Worked as a firefighter for the next 3 years • Developed increasing dyspnea and irritant sensitivity • Repeat PFTs showed worsening airflow obstruction with a bronchodilator response • Received disability retirement for reactive airways disease UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Final Diagnosis • Acute Eosinophilic Pneumonia • Subsequent onset of reactive airways disease UNITED STATES DEPARTMENT OF VETERANS AFFAIRS