Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
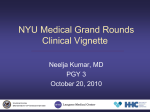
NYU Medical Grand Rounds Clinical Vignette Jeremy R. Beitler MD, PGY-2 December 16, 2009 UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Chief Complaint A 66-year-old man presents complaining of substernal chest and epigastric pain for thirty minutes. UNITED STATES DEPARTMENT OF VETERANS AFFAIRS History of Present Illness • The patient was in his usual state of good health until thirty minutes prior to presentation in the emergency room. • He reported a previously unlimited exercise tolerance. • He denied having previous episodes of chest pain. UNITED STATES DEPARTMENT OF VETERANS AFFAIRS History of Present Illness • Thirty minutes prior to presentation, the patient noted the sudden onset of non-radiating substernal chest pressure while climbing a flight of stairs. • The pain did not resolve with rest. • The chest pain was associated with dyspnea, diaphoresis, epigastric discomfort and a single episode of vomiting. • EMS was called. Aspirin 162mg was administered and the patient was brought to the Bellevue Hospital Emergency Room. UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Additional History Past Medical History • Hypercholesterolemia Family History • Mother: Diabetes mellitus • Father: Emphysema Past Surgical History • Appendectomy UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Social History • Lifetime non-smoker • Denies alcohol use • Denies illicit drug use Outpatient Medications Aspirin 81mg Daily Simvastatin 40mg QHS No known allergies UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Physical Examination General: Slightly pale and diaphoretic man in mild distress Vitals: T 97.0F, BP 134/92, HR 55, RR 22 O2 saturation: 99% on room air Cardiac: Non-displaced point of maximal impulse, no murmurs or rubs, no elevation of jugular venous pressure, 2+ distal pulses Pulmonary: Clear to auscultation Abdominal: Mild epigastric tenderness The remainder of the physical exam was normal. UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Initial Studies CBC: Within normal limits Basic Metabolic Panel: Within normal limits Hepatic Panel: Within normal limits Troponin-I: 0.128 ug/dL (< 0.059 ug/dL) CXR: Within normal limits UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Electrocardiogram UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Working Diagnosis Non-ST Elevation Myocardial Infarction UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Hospital Course • Fifteen minutes after arriving in the emergency room, the patient’s blood pressure fell to 80/30 mmHg. A 1 Liter bolus of normal saline was administered with return of a normal blood pressure. • Due to the transient hypotension, the cardiology consult service was called to evaluate the patient. • At the time of the cardiology consultant’s examination, the patient had developed diffuse bilateral rales. The ECG was interpreted as extensive anterior infarction with ongoing ischemia. • The ST-elevation myocardial infarction team activated, and Clopidogrel 600mg and Atorvastatin 80mg were administered. UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Hospital Course • The patient was taken emergently to the cardiac catheterization laboratory where diagnostic angiography demonstrated: • Total occlusion of the proximal LAD with angiographic features consistent with acute thrombus • 90% stenosis of the mid RCA • During the procedure, the patient developed ventricular fibrillation. He was successfully defibrillated and maintained on lidocaine. • Percutaneous coronary intervention was performed on the proximal LAD lesion with deployment of a drug-eluting stent. • Door-to-Balloon Time: 70 Minutes UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Hospital Course • The patient was admitted to the coronary care unit for observation and initiation of optimal medical therapy. • Troponin measurements peaked at levels greater than 50 ug/dL. • Transthoracic echocardiography demonstrated an LVEF of 33% with severe hypokinesis of the intraventricular septum, anterior walls and apical regions. UNITED STATES DEPARTMENT OF VETERANS AFFAIRS Final Diagnosis Acute Transmural Anterior Wall Myocardial Infarction UNITED STATES DEPARTMENT OF VETERANS AFFAIRS