Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
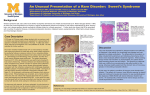
“It’s my hand, doc…” ID Case Conference 10-3-07 Gretchen Shaughnessy, MD CC: L hand wound 52 year old gentleman with HTN who presents in June 07 for a second opinion of a left hand wound. He states that since October 2006 he’s had recurrent ulcers on his left hand. He thinks he’s had about 6 since October, they usually last about a week and clear up with antibiotics. In the past he’s been on amicycline, augmentin, nad levofloxacin. The lesions appear to be getting more severe and in April of 2007 he was hospitalized for 4 days, given IV vancomycin, and then discharged on levofloxacin. In mid-May 2007 he noticed a small errythematous bump on his left 2nd MTP joint. He began scratching it and using a topical antiseptic but it progressed and opened with pus and grew in diameter. His PCP prescribed levofloxacin and referred him to dermatology. The dermatologist added minocycline but the wound continued to progress, turning black at the edges and growing in size. HPI (cont) He was admitted to Nash Regional in June 2007 where a biopsy of the lesion was inconclusive. Blood cultures, wound cultures, biopsy cultures for fungal, bacterial, and AFB were all negative. Left hand film revealed no evidence of osteomyelitis. HIV was negative. He was started on Vancomycin, Primaxin, and Biaxin during his course and was ultimately d/c'd on biaxin and doxycycline with a preliminary diagnosis of Mycobacterium marinum because of occupational exposure. Given the pt's overall minimal improvement, he presented to UNC ER for a second opinion. HPI Timeline October 2006 – started getting ulcers on L hand, each lasts a few weeks, seems to resolve in a few weeks. April 2006 – ulcer is larger than usual, doesn’t respond to outpatient antibiotics, patient is hospitalized and improves with vanc, d/ced on levofloxacin Mid-May 2006 – small errythematous bump develops on hand, topical antiseptic applied Early June 2006 – large ulcer present, hospitalized at OSH – started on vanc Late June 2006 – goes to UNC ED for second opinion. PMH Back Surgery many years ago – no hardware left in place HTN – well controlled on meds Recurrent hand ulcers as described in HPI NKDA Social History Lives in Rocky Mount with wife. Works in pressure washing and typically wears gloves but occasionally tears in them. He denies recent travel, denies livestock and exoctic animal exposure; they do have 3 dogs in the home. Denies any fists fights/hand trauma. Denies known interaction with military or middle east travelers. Denies tobacco, alcohol, or drugs. No significant family history. Medications Vasotec 20mg bid Ziac 10mg daily Norvasc 10mg daily ABX (started 6/17) Biaxin 500mg bid Doxycyline 100mg bid ROS The pt denies fevers, chills but since October pt endorses 27lb wt loss and intermittent left arm tingling. He denies palpable LAD, chest pain, shortness of breath. He denies abdominal pain, n/v/d, bloody stools. He denies change in UOP, dysuria, hematuria. Physical Exam BP 201 / 97-->161/83. HR: 71. RR: 19. Temp: 37.1 oral. O2 saturation: 98 % RA pleasant, NAD, well appearing PERRL, EOMI, sclera clear OP pink and moist, no exudative lesions supple no cervical, supraclavicular, axillary LAD RRR, with 3/6 systolic murmur loudest at LUSB CTA bilat no c/w soft, nontender, normoactive bs, no masses/organomegaly no CVA tenderness no LEE, 2+ radial/dp pulses. Left hand wound described in skin exam, mildly tender to palpation. A&Ox3, CN II-XII grossly intact. Skin exam 4cm x 4cm ulcer at 2nd MTP joint. Central yellowish granulation, dark purple edges. Dry, mildly erythematous. Nontender. Derm consult description: 3 cm wound with 1.5 cm central, punchedout ulceration (? biopsy site), and violaceous wound edges, desquamative wound edges. L antecubital with pustule. No tenderness, warmth, or induration. Labs 143 101 13 4.5 29 0.9 101 Ca 9.3 Mg 2.2 Phos 4.2 B12 318 Folate 4.7 ACE 7 ANA negative DS DNA negative 8.6 12.2 277 36.1 Diff – 6.1 – 1.4 – 0.7 – 0.2 – 0 MCV 108 MCHC 37 ESR 41 CRP 5.2 SPEP – decrease in gamma globulins Total Protein 6.9 Monoclonal component – IgG kappa but conc too low to quantify Discussion Pathology Skin, left hand, biopsy - Neutrophilic dermatosis with overlying pseudoepitheliomatous hyperplasia The AFB, GMS, and Gram stains are negative for infectious organisms. The differential diagnosis includes Sweet's syndrome. After reviewing the slides from the OSH, dermatology gave this patient the diagnosis of Sweet’s Syndrome Sweet’s Syndrome One of the neutrophilic dermatoses Pathologic dx - Intense epidermal and/or dermal inflammatory infiltrate composed mostly of neutrophils with no evidence of infection or vasculitis First described in 1964 by Dr. Sweet in eight female patients Pathogenesis Unknown Initial hypotheses of immune complex vasculitis, T-cell activation, or altered neutrophil function were not confirmed with experimental data Current hypothesis is cytokine dysregulation Sweet's syndrome has been described as a complication of granulocyte-colony stimulating factor (G-CSF) therapy, supporting this theory Associated Conditions 20-25% of patients with Sweet's syndrome have an associated malignancy Most hematopoietic – MDS or AML ~15% of malignancy associated Sweet’s syndrome are assocated with solid tumors genitourinary, breast, and gastrointestinal tract most common Associated Conditions (cont) Bacterial infections — vaccinations, streptococcus, mycobacterium, Yersinia, typhus, salmonella Viral infections — cytomegalovirus, chronic active hepatitis, HIV Drugs — lithium, furosemide, hydralazine, oral contraceptives, minocycline, imatinib, mesylate and tmp/smx. Autoimmune and collagen vascular diseases — rheumatoid arthritis, systemic lupus erythematosus, mixed connective tissue disease, Hashimoto thyroiditis, Sjögren's syndrome, Behcet's disease Inflammatory bowel disease — Crohn's disease, ulcerative colitis Other — pregnancy, complement deficiency, subacute necrotizing Iymphadenitis, and Poem's syndrome Primary Features Cutaneous eruption consisting of erythematous papules and plaques a dermal nonvasculitic neutrophilic infiltration on biopsy Fever Peripheral neutrophilia Dermatologic Findings Erythematous to violaceous tender papules which enlarge to form plaques with an irregular pseudovesicular surface True pustulation and blistering can occur Plaques usu a few centimeters in diameter. May cause pain or burning sensation, not pruritic. Most common areas – dorsum of hands, face, neck, upper extremeties. More Images See UpToDate Available online at UNC Health Sciences Library [on campus only] Systemic symptoms Fever in 40-80% Can be intermittent URI or flu-like illness can precede cutaneous lesions Eye involvement with conjuntivitis, episcleritis, iridocyclitis 1/3rd of pts have arthralgias, myalgia, arthritis – asymmetric, nonerosive, mostly knees and wrists Internal organ involvement can include neutrophilic alveolitis, sterile osteomyelitits, ARF, involvement of kidneys, liver, pancreas, neurologic, and psychiatric changes. All viseral manifestations repsond to corticosteroid therapy. Lab Findings Nonspecific findings Elevated ESR Elevated CRP Peripheral neutrophilia with 70% band forms Decreased hemoglobin Slight increase in alk phos, AST, GGT +ANCA rarely Proposed Diagnostic Criteria Major Abrupt onset of typical cutaneous lesions Histopathology consistent with Sweet’s Minor Antecedent fever of infection Accompanying fever, arthralgias, conjunctivitis, or underlying malignancy Leukocytosis Good response to steroids but no response to antibiotics * Two major and two minor criteria are needed for diagnosis. Adapted from Su, WP, Liu, HN, Cutis 1986; 37:167. Treatment All treatment based on uncontrolled nonrandomized case series Prednisone is standard treatment Other options include NSAIDS Dapsone Potassium Iodide Colchicine Doxycycline Clofazzimine Our Patient’s Course Last seen in derm clinic 8-07 Took 8 week course of dapsone, skin lesions resolved completely Now on a prolonged taper of dapsone per derm clinic No associated condition yet diagnosed Search PubMed Sweet’s Syndrome Case Reports Reviews Differential Diagnosis Drug Therapy