Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
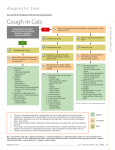
Differential Diagnosis And Treatment In Adults MÜNEVVER ERDİNÇ Department of Chest Diseases Ege University Faculty of Medicine Acute Cough lasting less than 3 weeks Subacute Cough lasting 3 to 8 weeks Chronic Cough Lasting more than 8 weeks Morice AH.Eur Respir J 2004 :24:481-492 Fontana GA.Thorax 2003;58:1092-1095 Irwin RS.NEJM 343(23): 1715-1721,2000 Irwin RS. Chest 1998; 114(suppl1) :133S-181S Differantial Diagnosis of Chronic Cough in Adults • PNDS – Allergic rhinitis – Chronic sinusitis • GERD • Cough variant asthma • ACEI induced cough • Pertusis • Neurogenic – Traumatic – Postinfectious cough • Phychogenic cough • Chronic aspiration • Zenker diverticulosis • • • • • • • • • • Foreign body Chronic bronchitis Bronchiectasis Lung cancer Subglottic stenosis Tracheomalasie Tracheoesophageal fistul Tuerculosis Sarcoidosis Congestive heart failure Simpson CB. Otolaryngology–Head Neck Surg 2006; 134: 693-700 In prospective studies in adults, chronic cough is most commonly due to 6 disorders : Upper Airway Cough Syndrome (UACS) Asthma GERD Chronic Bronchitis Bronchiectasis Non-asthmatic Eosinophilic Bronchitis Guidelines Writing Committee. Chest 2006; 129 (Suppl. 1): 1S-292S New Considerations Eosinophilic bronchitis Atopic cough Non acid(volume)/ weakly acid reflux Idiopathic (unexplained) öksürük Diagnosis and Management of Cough ACCP Evidence-Based CPG 2006 Postnasal drip syndrome (PNDS) renamed upper airway cough syndrome (UACS) Upper airway afferents may reflexly enhance coughing Nonasthmatic eosinophilic bronchitis recognized as a common cause of chronic cough Idiopathic cough renamed unexplained cough The term acid reflux disease, unless it can be definitively shown to apply, replaced by reflux disease Update of current diagnostic and therapeutic approaches Common diseases, Uncommon diseases New algorithms for the management of cough in adults and children An empiric integrative approach is recommended Guidelines Writing Committee. Chest 2006; 129 (Suppl. 1): 1S-292S Plevkova, et al. Respir Physiol Neurobiol 2004; 142: 225-235 PNDS ASTHMA 12 16 6 13 12 4 GERD 10 1. Gastroesophageal reflux disease (21-41%) 2. Cough variant asthma (24-59%) 3. Postnasal drip syndrome (41-58%) Chest 1999;116:279-284 Percentage of Cases Presenting 1,2,3 and 4 Causative factors Percentage of Cases Presenting 1,2,3, and 4 Causative Factors 8,9% 16,7% 38,5% 1 38,5% 2 3 4 1 2 3 4 35,9% Chest 1999;116:279-281 Asthma and/or GERD, PNDS responsible for 93.6% of the cases of chronic cough İmmunocompetent patients Not exposed to enviromental irritants Chest radiograph is normal Not taking an ACE inhibitor Not a current smoker Harding SM .Chest 2003;123:659-660 Diagnosis (%) Percentage Percentageof of Diagnoses Changing Trends in Diagnosis GERD REFLUX ASTHMA ASTHMA RHINITIS RHINITIS 90 80 70 60 50 40 30 20 10 0 1998 1999 2000 2001 2002 2003 GERD ? Heartburn (pyrosis) and regurgitation At least weekly symptoms extraesophageal reflux symptoms and/or esophageal mucosal damage / Functional defect in LES syphincter Delayed gastric emptying Decreased saliva Impaired esophageal clearance Hiatal hernia İncreased intra-abdominal pressure Katzka & DiMarino 1995 FLR Signs •Edema and hyperemia of larynx •Vocal cord erythema, polyps, granulomas, ulcers •Hyperemia and lymphoid hyperplasia of posterior pharynx •Interarytenoid changes •Subglottic stenosis GERD-related cough incidence 5 - 55% ARRD 1981;123:413-417 Arch Intern Med 1996;156:997 Chest 1993;104:1511-1517 El Hennawi, 2004 OHNS May be the sole presenting symptom(1/3) Association between cough and reflux is important Esophageal-tracheal-bronchial reflex Microaspiration Nonacidic factors? Esophageal dismotility? Thorax 2003:58;1092-1095) (Chest 1997; 111: 1389-1402) Irwin RS. Chest 2006;129:80S-94S Esophagus Tracheobronchial Tree REFLUX Microaspiration Esophageal Vagal Afferents Airway Vagal Afferents CNS Airway Vagal Efferents Airway . Mediator Release . Inflammation . Edema . Mucus . Smooth Muscle Bronchial Hyperreactivity Stein MR.Am J Med 2003 Chest 1997;111: 1389-1402 Oesophagus Stomach Pharyngeal pHmetry Not GERD Clinical GERD symptoms ? Nonacid, weakly acid reflux? + Increase dose PPI + alginate İmproved Consider Simultaneously dual probes 24 hours pHmonitoring and intraesophageal impedance Not improved Continue pHmetry under treatment Irwin RS.AJRCCM 165:1469-74,2002 McGarvey LPA.Thorax 59:342-346,2004 Multichannel intraluminal impedance-pH catheter 6 impedance channels 17 cm 15 cm 9 cm + 7 cm 1 pH electrode 5 cm 3 cm Adult Standard Model ZAN-S61C01E pH - 5 cm Non acid reflux On going reflux of ‘non-acid’ material may be responsible for continuing symptoms while on acid-suppressing medications Therapy in Esophageal-pulmonary reflux Conservative and lifestyle measures Ampirical therapy: Acid suppression Proton pump inhibitors PPI x 2 / 3 months Therapy failure 24 hour intraesophageal pHmetry ( pharyngeal pHmetry ) GERD (+) High dose PPI + H2 blocker agent Surgery(Fundoplication) Pulmonary and Crit Care Update 1994; Vol 9 Morice AH. ERJ 2004;24:481-492 Cumulative Response to GERD Therapy Weeks of antireflux therapy Patients responded No No (%) 2 16 (41) 4 38 (86) 6 42 (95) 8 43 (99) 12 weeks 44 (100) Poe RH.Chest 2003;123:679-684 Preop pH <4: %23.6 De Meester: 85 Postop pH <4: %2.4 De Meester: 9.9 Clinical Profile That Chronic Cough İs Likely Due To ‘Silent GERD’ 1. Chronic cough for at least 2 months 2. Immunocompetent patients 3. Chest radiograph is normal 4. Not exposed to enviromental irritants nor a present smoker 5. Not taking an ACE inhibitor 6. Symptomatic asthma has been ruled out 7. Rhinosinus diseases has been ruled out: 8. ‘Silent sinusitis’ has been ruled out 9. Nonasthmatic eosinophilic bronchitis has been ruled out: BPT is negative Cough has not improved with asthma therapy First generation H1 antagonists has been used Eo 3% in induced sputum Cough has not improved with steroids Irwin RS. Chest 2006;129:80S-94S İrwin RS. AJRCCM Vol 165; 1469-1474, 2002 Postnasal Drip Syndrome (PNDS) • Prevalence : 8 – 87% • Pathogenesis : The sensation of drainage of secretions from the nose or paranasal sinuses into the pharynx • Clinical Presentation: Dripping sensation Tickle in the throat Nasal congestion Mucus in oropharynx Cobblestone appearence of oropharynx ACCP consensus. CHEST 1998; 114: 133-181 ERS Task Force. ERS Journal ; 24: 553-566 Pathogenic Triad in Chronic Cough. CHEST 1999; 116: 279-284 Evaluation of chronic cough. UPTODATE 2005 In patient with chronic cough that is related to upper airway abnormalities Upper Airway Cough Syndrome Chest 2006;129:63S-71S UACS Treatment Antihistamines / decongestant combinations - “Older” sedating antihistamines more effective - Treatment effect should be observed in 1 week Additional / Alternative treatments : Ipratropium nasal spray : 2-7 days Nasal steroids (such as BDP, FP,BUD) : 2-3 days - 2 week 3 months prescribed NO YES Bronchial hyperreactivity Asthmatic Coughs Eosinophilic Eronchitis Cough Variant Asthma NO Asthma YES Airway obstruction Cough Variant Asthma Prevalence : 24 – 59% Clinical Diagnosis Gold standard History - Episodic symptoms, Family history Reversibility testing PEF monitoring Bronchoprovocation test Differential Diagnosis: Decreased of cough with classical asthma therapy ACCP consensus. CHEST 1998; 114: 133-181 ERS Task Force. ERS Journal ; 24: 553-566 The Journal of Respiratory Disease; 25; 310-315 THORAX 59; 342-346 Eosinophilic Bronchitis • • • • • • Isolated chronic cough, productive of sputum Normal lung function without variable airflow limitation Airway hyperresponsiveness absent Eosinophilia in sputum and BAL Cough reflex to capsaicin increased Normal daily variability in peak expiratory flow (<20%) Middle age patients Smoking is unusual, occupational ? Prevalence of atopy similar population Good respond to inhaled steroids Gibson et al. Lancet 1989 Chest 2006;129:116S-121S Eosinophilic Bronchitis A Worldwide Disease 13% UK 91patients, 19992 15% Korea 14% USA 92 patients, 20023 37patients 20031 33% Turkey 36 patients, 20036 20% China 10% Australia 86 patients 20035 30 patients, 20004 1)Kim et al AJRCCM 2003; 2) Brightling et al AJRCCM 1999;160:406-10, 3) Joo Korean JIM 2002;17:31-7, 4) Carney et al AJRCCM 1997; 156:211-6, 5) Ma et al Zhongua 2003;26:362-5, 6) Ayik, Erdinc et al Respir Med 2003;97:695-701 Causes of chronic cough Primary cause of cough No. of patients (%)* Eosinophilic bronchitis 12 (33.3%) Postnasal drip syndrome 8 (22.2%) Gastroesophageal reflux 8 (22.2%) Idiopathic chronic cough 8 (22.2%) Postinfectious cough 2 (5.6%) Cough-variant asthma 1 (2.8%) Ayık SÖ, Başoğlu ÖK, Erdinç M. Respir Med Vol. 97 (2003) 695-701 Causes of Isolated Chronic Cough Primary cause of chronic cough Patients (%) Rhinitis/PND 24 Asthma Post-viral 17.6 13.2 Eosinophilic bronchitis 13.2 GERD 7.7 Unexplained (Idiopathic) COPD Bronchiectasis 6.6 6.6 5.5 ACE inhibitor-induced cough 4.4 Lung cancer 2.2 Cryptogenic fibrosing alveolitis 1.1 Brightling CE et al. AJRCCM 1999 Asthmatic Cough Airway obstruction Reversibility PEF değişkenliği Yes Asthma İnhaled steroid β2-agonist No Bronchial provocation test Eosinophilic Bronchitis İnhaled steroid Negative Positive PEF monitoring Induced sputum (3% eosinophilia Increased NO all of them Cough Variant Asthma İnhaled steroid β2-agonist Chronic Unexplained (Idiopathic) Cough • Prevalence: 0-50% • More agressive diagnosis and treatments UACS, GERD and postinfectious cough leads to lower incidence ‘unexplained’. • Airway inflammation Mast cell, histamin, cysteinil LTs, PD2, PE2 Irwin RS,et al. Chest 2006;130:362-370 Chronic Unexplained (Idiopathic) Cough Potential Reasons Important missed history (smoking,ACEI,enviromental,drugs,allergy) Failure to do correct diagnostic tests Failure to use ‘empiric’ treatment Failure to use effective therapy Unknown disease process « Truly idiopathic cough is rare and misdiagnosis very common, especially if cough is provoked by sites outside the airways » Eur Respir J 24: 481-492 2004 Idiopathic cough %? Studies in the 1980’s % patients 40 30 Irwin 1981 20 Poe 1982 Poe 1989 10 0 Asthma GERD PNAS Idiopathic Idiopathic cough %? 1990-1995 % patients 50 40 Irwin 1990 30 Hoffstein 1994 20 O Connel 1994 Smyrinos 1995 10 0 Asthma PNAS Idiopathic cough %? 1996-1999 % patients 60 50 Mello 1996 40 Marchesani 1998 30 Mc Garvey 1998 20 Brightling 1999 Palombani 1999 Simpson 1999 10 0 ASTHMA OESOPH NOSE IDIO Idiopathic cough %? 2000 50 % patients 40 Birring 2003 30 Hague 2005 20 Kastelik 2005 Matsumoto 2007 10 0 ASTHMA NOSE Chronic Idiopathic Cough Haque et al Chest 2005;127:1710-1713 Chronic Idiopathic Cough Predominantly female and associated with BAL lymphocytosis Raising the possibility of a link between autoimmune diseases Chronic Idiopathic Cough (n=22) Control (n=65) p Autoimmune disease 13/22 (59%) 8/65 (12%) p<0.001* Positive autoantibody 6/15 (40%) 3/24 (13%) p<0.05 *OR: 8.8 Surinder S. Et al. Respir Med 98:242-246;2004 Chronic Idiopathic Cough Inflammation Birring et al AJRCM 2004 Chronic Idiopathic Cough + BAL lymphocytosis • • • • • • • • • • Sarcoidosis Hypersensitivity pneumonitis Rheumatoid Arthritis Sjögren’s syndrome Lung tx Inflammatory bowel disease Hypothyroidism Autoimmune disorders (SLE, RA) Pernisious anemia DM Thorax 2003;58:1066-1070 Chronic Idiopathic Cough It is not correct to state that “a typical lymphocytic airways inflammation is seen in idiopathic cough” because lymphocytic or lymphoplasmacytic inflammation a non-specific finding related to trauma of coughing Irwin RS,et al. Chest 2006;130:362-370 Psychogenic Cough • Cough is often triggered by a common cold • Usually dissapears during sleep • Like a dog barking • The diagnosis of psychogenic cough is one of exclusion, after ruling out an organic or functional cause of cough. • Specific or empiric treatment • Antitussives are usually ineffective. Respirology 2006;Suppl 4 ;S160-S174 Irwin RS et al. Chest 1998, 114:2 suppl ERS Task Force: Eur Respir J 2004, 24:481-492 Postinfectious Cough • Prevalence: 11-25 % • History: After a respiratory tract infection • Diagnosis: Spasmodic cough Normal chest radiograph, with/without ronchii Respiratory viruses, m.pneumoniae, c.pneumoniae, B.pertussis Serum acute IgA antibody ELISA Rarely lymphocytosis Airway inflammation +/- Airway hyperresponsivenes Irwin RS et al. Chest 1998, 114:2 suppl ACCP consensus. CHEST 1998; 114: 133-181 ERS Task Force. ERS Journal ; 24: 553-566 Postinfectious Cough – Oral and/or inhaled steroid (2-3 weeks) – Antibiyotic : Macrolides (Chlamydia, mycoplasma) TMP/SMX : Pertusis (3-6 weeks) – Ipatropium bromid decrease efferent limb of the cough reflex decrease stimulation of cough receptors – Antitussive therapy Irwin RS et al. Chest 1998,114:2 suppl Miyashita N. J Med Microbiol 2003, 52:3,265-269 ACEI Induced Chronic Cough • Frequency: 0.2-33% • Predominantly female • Not dose related • Appears within hours, weeks, months • Pathogenesis: Neurokinin, Substance P, Prostoglandins, stimulates afferent C-fibers in the airway increased cough reflex sensitivity • Prefer Angiotensin II receptör antagonists Treatment NONSPECIFIC Antitussive SPECIFIC Protussive Codein Hypertonic saline Dextromethorphan Erdostein Difenhidramin Amilorid Pseudoephedrine N asetilsistein Dekstrobromfeniramin Terbutalin Ipatropium Bromide Physiotherapy Naproksen Postural drainage Causative treatment Irwin RS et al. Chest 1998, 114:2 Future Therapies – Capsaicin type I Vanilloid receptor antagonists – Selective opioid receptor agonists – Opioid-like receptor agonists – Tachykinin receptor antagonists – Endogenous cannabinoids – 5-HT receptor agonists – Large-conductance calcium-activated potassium channel openers Dicpinigaitis PV.Chest 2006 ;129:284S-286S Chronic Cough Algoritm For the Management of Adults Chronic cough History,Examination, Chest X-Ray, PFT Abnormal Sputum, bronchoscopy,CT, Cardiac tests Normal Smoking, ACEI , Irritants ? Specific yes Stop 4 weeks diagnosis - treatment Chronic Cough Algoritm For the Management of Adults Chronic cough History,Examination, Chest X-Ray, PFT Abnormal Specific diagnosis - Treatment Normal No Smoking, ACEI, Irritants ? Yes UACS,GERD, Asthma, NAEB ? Sputum, bronchoscopy,CT, Cardiac tests Stop 4 weeks Yes Cough? No İmproved? Chronic Cough Algoritm Chronic cough History,Examination, Chest X-Ray, PFT Specific diagnosis - treatment Normal No Smoking, ACEI ?, Irritants? Therapy Yes Cough? Yes Stop 4 weeks UACS,GERD, Asthma, NAEB Empiric/ Specific Abnormal Sputum, Bronchoscopy,CT, Cardiac tests Yok Improved Yes Cough? No Chronic Cough Algoritm Chronic cough History,Examination, Chest X-Ray, PFT Abnormal Normal No Sputum, Bronchoscopy,CT, Cardiac tests Specific diagnosis - treatment Smoking, ACEI ?, Irritants? Yes Cough? Yes UACS,GERD, Asthma, NAEB Empiric Therapy No response Stop 4 weeks No Improved ENT, Sinus CT BPT,PEF monit., NO Esophageal tests Specific Diagnosis - Treatment UACS,GERD, Asthma, NAEB Empiric or Specific Diagnosis and Treatment Improved No Cough ? Yes Post infectious? Yes Consider uncommon causes Sputum, HRCT, Bronchoscopy Specific diagnosis - Treatment No Yes Cough ? Physcogenic cough? UACS,GERD, Asthma, NAEB Empiric or Specific Diagnosis and Treatment Improved No Cough ? Yes Post infectious? Yes Consider uncommon causes Sputum, HRCT, Bronchoscopy Specific diagnosis - Treatment No Yes Cough ? Improved Specific diagnosis - Treatment No Chronic idiopathic cough Physcogenic cough? THANK YOU…