Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
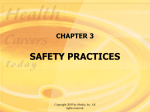
Chapter 14 Bronchiectasis C A B E D Figure 14–1. Bronchiectasis. A, Varicose bronchiectasis. B, Cylindrical bronchiectasis. C, Saccular bronchiectasis. Also illustrated are excessive bronchial secretions (D) and atelectasis (E), which are both common anatomic alterations of the lungs in this disease. Slide 1 Copyright © 2006 by Mosby, Inc. Three Forms of Bronchiectasis Slide 2 Varicose bronchiectasis Cylindrical bronchiectasis Saccular bronchiectasis Copyright © 2006 by Mosby, Inc. Anatomic Alterations of the Lungs Slide 3 Chronic dilation and distortion of bronchial airways Excessive production of often foul-smelling sputum Smooth muscle constriction of bronchial airways Hyperinflation of alveoli (air-trapping) Atelectasis, consolidation, and parenchymal fibrosis Hemorrhage secondary to bronchial arterial erosion Copyright © 2006 by Mosby, Inc. Etiology Slide 4 Acquired bronchiectasis Recurrent pulmonary infection Bronchial obstruction Congenital bronchiectasis Kartagener’s syndrome Hypogammaglobulinemia Cystic fibrosis Copyright © 2006 by Mosby, Inc. Overview of the Cardiopulmonary Clinical Manifestations Associated with BRONCHIECTASIS The following clinical manifestations result from the pathophysiologic mechanisms caused (or activated) by Atelectasis (see Figure 9-12), Consolidation (see Figure 9-8), Bronchospasm (see Figure 9-10), and Excessive Bronchial Secretions (see Figure 9-11)—the major anatomic alterations of the lungs associated with bronchiectasis (see Figure 14-1). Slide 5 Copyright © 2006 by Mosby, Inc. Figure 9-7. Atelectasis clinical scenario. Slide 6 Copyright © 2006 by Mosby, Inc. Figure 9-8. Alveolar consolidation clinical scenario. Slide 7 Copyright © 2006 by Mosby, Inc. Figure 9-9. Increased alveolar-capillary membrane thickness clinical scenario. Slide 8 Copyright © 2006 by Mosby, Inc. Figure 9-10. Bronchospasm clinical scenario (e.g., asthma). Slide 9 Copyright © 2006 by Mosby, Inc. Figure 9-11. Excessive bronchial secretions clinical scenario. Slide 10 Copyright © 2006 by Mosby, Inc. Clinical Data Obtained at the Patient’s Bedside Vital signs Slide 11 Increased respiratory rate Increased heart rate, cardiac output, blood pressure Copyright © 2006 by Mosby, Inc. Clinical Data Obtained at the Patient’s Bedside Slide 12 Use of accessory muscles of inspiration Use of accessory muscles of expiration Pursed-lip breathing Increased anteroposterior chest diameter (barrel chest) Cyanosis Digital clubbing Copyright © 2006 by Mosby, Inc. Figure 2-36. The way a patient may appear when using the pectoralis major muscles for inspiration. Slide 13 Copyright © 2006 by Mosby, Inc. Figure 2-41. A, Schematic illustration of alveolar compression of weakened bronchiolar airways during normal expiration in patients with chronic obstructive pulmonary disease (e.g., emphysema). B, Effects of pursed-lip breathing. The weakened bronchiolar airways are kept open by the effects of positive pressure created by pursed lips during expiration. Slide 14 Copyright © 2006 by Mosby, Inc. Digital Clubbing Figure 2-46. Digital clubbing. Slide 15 Copyright © 2006 by Mosby, Inc. Clinical Data Obtained at the Patient’s Bedside Slide 16 Peripheral edema and venous distention Distended neck veins Pitting edema Enlarged and tender liver Copyright © 2006 by Mosby, Inc. Distended Neck Veins Figure 2-48. Distended neck veins (arrows). Slide 17 Copyright © 2006 by Mosby, Inc. Figure 2-47. Pitting edema. From Bloom A, Ireland J: Color atlas of diabetes, ed 2, London, 1992, Mosby-Wolfe. Slide 18 Copyright © 2006 by Mosby, Inc. Cough, sputum production, and hemoptysis Slide 19 A chronic cough with production of large quantities of foul-smelling sputum is a hallmark of bronchiectasis Copyright © 2006 by Mosby, Inc. Clinical Data Obtained at the Patient’s Bedside Chest assessment findings (primarily obstructive) Slide 20 Decreased tactile and vocal fremitus Hyperresonant percussion note Diminished breath sounds Rhonchi and Wheezing Copyright © 2006 by Mosby, Inc. Clinical Data Obtained at the Patient’s Bedside Chest assessment findings (primarily restrictive) Slide 21 Increased tactile and vocal fremitus Bronchial breath sounds Crackles Whispered pectoriloquy Dull percussion note Copyright © 2006 by Mosby, Inc. Figure 2-12. Percussion becomes more hyperresonant with alveolar hyperinflation. Slide 22 Copyright © 2006 by Mosby, Inc. Slide 23 Figure 2-17. As air trapping and alveolar hyperinflation develop in obstructive lung diseases, breath sounds progressively diminish. Copyright © 2006 by Mosby, Inc. Clinical Data Obtained from Laboratory Tests and Special Procedures Slide 24 Copyright © 2006 by Mosby, Inc. Pulmonary Function Study: Expiratory Maneuver Findings Primarily Obstructive Slide 25 FVC FEVT FEF25%-75% FEF200-1200 PEFR MVV FEF50% FEV1% Copyright © 2006 by Mosby, Inc. Pulmonary Function Study: Lung Volume and Capacity Findings Primarily Obstructive VT N or VC Slide 26 RV FRC N or ERV N or RV/TLC ratio IC N or TLC Copyright © 2006 by Mosby, Inc. Pulmonary Function Study: Expiratory Maneuver Findings Primarily Restrictive FVC FEVT N or FEF25%-75% N or FEF200-1200 N PEFR MVV FEF50% FEV1% N Slide 27 N or N N or Copyright © 2006 by Mosby, Inc. Pulmonary Function Study: Lung Volume and Capacity Findings Primarily Restrictive VT Slide 28 RV FRC TLC N or VC IC ERV RV/TLC ratio N Copyright © 2006 by Mosby, Inc. Arterial Blood Gases Mild to Moderate Bronchiectasis pH Slide 29 Acute alveolar hyperventilation with hypoxemia PaCO2 HCO3 (Slightly) PaO2 Copyright © 2006 by Mosby, Inc. Time and Progression of Disease Disease Onset Alveolar Hyperventilation 100 90 PaO2 or PaCO2 80 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors 70 60 PaO2 50 40 30 20 10 0 Figure 4-2. PaO2 and PaC02 trends during acute alveolar hyperventilation. Slide 30 Copyright © 2006 by Mosby, Inc. Arterial Blood Gases Severe Bronchiectasis Chronic ventilatory failure with hypoxemia pH Normal Slide 31 PaCO2 HCO3PaO2 (Significantly) Copyright © 2006 by Mosby, Inc. Time and Progression of Disease Disease Onset Alveolar Hyperventilation Chronic Ventilatory Failure 100 90 Pa02 or PaC02 80 70 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors Point at which disease becomes severe and patient begins to become fatigued 60 50 40 30 20 10 0 Figure 4-7. PaO2 and PaCO2 trends during acute or chronic ventilatory failure. Slide 32 Copyright © 2006 by Mosby, Inc. Acute Ventilatory Changes on Chronic Ventilatory Failure Slide 33 Acute alveolar hyperventilation on chronic ventilatory failure Acute ventilatory failure on chronic ventilatory failure Copyright © 2006 by Mosby, Inc. Oxygenation Indices QS/QT DO2 VO2 Normal O2ER Slide 34 C(a-v)O2 Normal SvO2 Copyright © 2006 by Mosby, Inc. Hemodynamic Indices (Severe Chronic Bronchiectasis) Slide 35 CVP RAP PA PCWP Normal CO SV SVI CI Normal Normal Normal Normal RVSWI LVSWI PVR SVR Normal Normal Copyright © 2006 by Mosby, Inc. Abnormal Laboratory Tests and Procedures Slide 36 Hematology (Increased hematocrit and hemoglobin) Sputum examination Streptococcus pneumoniae Haemophilus influenzae Pseudomonas aeruginosa Anaerobic organisms Copyright © 2006 by Mosby, Inc. Radiologic Findings Slide 37 Chest radiograph Translucent (dark) lung fields Depressed or flattened diaphragm Long and narrow heart Enlarged heart Bronchogram CT scan Copyright © 2006 by Mosby, Inc. Figure 14-2. Cylindrical bronchiectasis. Left posterior oblique projection of a left bronchogram showing cylindrical bronchiectasis affecting the whole of the lower lobe except for the superior segment. Few side branches fill. Basal airways are crowded together, indicating volume loss of the lower lobe, a common finding in bronchiectasis. (From Armstrong P et al: Imaging of diseases of the chest, ed 2, St. Louis, 1995, Mosby.) Slide 38 Copyright © 2006 by Mosby, Inc. Figure 14-3. Saccular bronchiectasis. Right lateral bronchogram showing saccular bronchiectasis affecting mainly the lower lobe and posterior segment of the upper lobe. (From Armstrong P et al: Imaging of diseases of the chest, ed 2, St. Louis, 1995, Mosby.) Slide 39 Copyright © 2006 by Mosby, Inc. Figure 14-4. Varicose bronchiectasis. Left posterior oblique projection of left bronchogram in a patient with the ciliary dyskinesia syndrome. All basal bronchi are affected by varicose bronchiectasis. (From Armstrong P et al: Imaging of diseases of the chest, ed 2, St. Louis, 1995, Mosby.) Slide 40 Copyright © 2006 by Mosby, Inc. Figure 14-5. Bronchiectasis. High-resolution thin-section (1.5-mm) computed tomographic (HRCT) scan showing numerous oval and rounded ring opacities in the left lower lobe. The right lung appears normal. The fact that the airways tend to be arranged in a linear fashion and have walls of more than hairline thickness helps distinguish these bronchiectatic airways from cysts or bullae. (From Armstrong P, Wilson AG, Dee P: Imaging of diseases of the chest, St. Louis, 1990, Mosby.) Slide 41 Copyright © 2006 by Mosby, Inc. General Management of Bronchiectasis General treatment includes: Slide 42 Controlling pulmonary infections Controlling airway secretions Preventing complications Copyright © 2006 by Mosby, Inc. General Management of Bronchiectasis Respiratory care treatment protocols Slide 43 Oxygen therapy protocol Bronchopulmonary hygiene therapy protocol Hyperinflation therapy protocol Aerosolized medication protocol Mechanical ventilation protocol Copyright © 2006 by Mosby, Inc. General Management of Bronchiectasis Other medications commonly prescribed by the physician Slide 44 Xanthines Expectorants Antibiotics Copyright © 2006 by Mosby, Inc. Classroom Discussion Case Study: Bronchiectasis Slide 45 Copyright © 2006 by Mosby, Inc.