Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
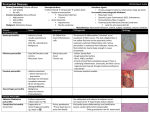
A Case of Two Chest Pains July 12th :57 y/o woman presenting to urgent care with c/o chest pain and dysnea - face flushed, anxious, appearing in distress with sudden c/o of dizziness and SOB, no N/V/diaphoresis Chest pain gradual worsening since last night – central cp with dysnpea, thought it was heartburn – had started tapering her dose of prednisone being treated for pericarditis VS: 112/47 HRR 106 RR 28 O2 sat 98% RA afebrile Initial interventions: 100% O2 sat w/ 3/l ,ECG NSR, troponin 0.00, IV access – toradol 30 mg Medications: Prednisone 25 mg – only one tapered dose of 20 mg, last hs took 25 mg; Nexium 40 mg od Allergies: NKA PMH: recent episode pericarditis – being followed by CR Internal Medicine: Echo July 7th = borderline LVH, mild LV/RV septal wall dyssychrony, EF 70%, L atrium borderline dilated, mild mitral valve sclerosis & calcification w/ small pericardial effusion, no cardiac tamponade CT chest July 7th = decreased effusion, thickening of pericardium query constrictive pericardium Social hx: recent loss of husband d/t massive MI at home; has custody of her granddaughter, and parent living with her P/E: Resp,CVS unremarkable, no rub Labs ordered this visit: Cr, K+, ESR, Random Glucose Consult with GP colleague: pericarditis Monitored for few hours to ensure pain and dyspnea settled Continue with 25 mg dose of prednisone Had follow up appointment with Internal Medicine in CR Encouraged to follow up with regular office appointment RTC urgent if symptoms worsening Seen in urgent care again July 19th – more dramatic presentation – acute onset of central, anterior chest pain, continuous, sharp, rates 10/10 radiating to back, should, neck with abd cramping – walked in with assistance, unsteady, flused, tachypneic Current meds Prednisone 25 mg, Nexium 40 mg, Tramadol O2, IV Toradol, ECG unchanged Internal Medicine consult 66 y/o man walked in to urgent care July 13th with c/o chest pain x 2 days describes as more discomfort central radiating to R shoulder and scapula – hx of pericariditis post CABG Dec 2010 pain prior has been on L side only Reports sharp pain with deep breath but no SOB, nausea, vomiting, diaphoresis, anxiety Recently ++fatigued, napping ++ during day Waking at night with worsening shoulder pain Has taken 6 tablets of ibuprofen in last 24 hours with little improvement Wife concerned it is his heart, encouraged him to be assessed Medications: Omeprazole 20 mg od, Metoprolol 25 mg bid, ASA 81 mg od, Pravastatin 80 mg od, Metformin 500 mg bid, Fenofibrate 145 mg od Allergies: iodine Previous labs normal eGFR 62 A1c 6% PMH: GERD, Dyslipidemia, DM Type 2, Quad bypass post MI Dec 2010, pericariditis Jan 2011, R rotator cuff tear (inferior labral tear) June 2011 P/E: ◦ Respiratory unremarkable ◦ CVS: S1 & S2 slurred no elevated JVP, VS: 117/77 HRR 81 RR 16 02 sat 99% RA afebrile ◦ MSK: limited ROM R shoulder d/t pain ECG: NSR query 1 degree AV block & septal changes, Troponin 0.00, Na 144, K+ 3.3 Cl 110 Glucose 4.5 Creat 70 Urea 3.6 Hgb 122 IV access: Toradol 30 mg IV Discharged with follow up with Internal Medicine Angina Pectoris Aortic Dissection Aortic Stenosis Coronary Artery Vasospasm Esophageal Rupture Esophageal Spasm Esophagitis Gastritis, Acute Gastroesophageal Reflux Disease Myocardial Infarction Myocardial Ischemia Peptic Ulcer Disease Pulmonary Embolism Fatigue Fever Pain worse when lying down Palpitations Dyspnea Clinical Pearls: ◦ Likely pericariditis if pain improved with NSAIDS ◦ Likely pericariditis if pain improved with sitting up and leaning forward Common disease, frequently subclinical= inflammation of the pericaridium (fibrous sac surrounding the heart) Recurrent pericarditis is most commonly observed in the cases of acute nonspecific pericarditis. The recurrence rate appears to be in the range of 15% to 32% after an initial attack. Causes: ◦ ◦ ◦ ◦ ◦ ◦ Idiopathic Infectious: viral (CMV, HIV, Herpes), bacterial, fungal Systemic disease Dressler’s: post MI Trauma Neoplasm Pericarditis can be classified according to the composition of the inflammatory exudate or in other words the composition of the fluid that accumulates around the heart.[1] Types include: serous purulent fibrinous caseous hemorrhagic Post infarction Depending on the time of presentation and duration, pericarditis is divided into "acute“ (more common) and "chronic" forms. Acute pericarditis can occur as a complication of infections, immunologic conditions, or MI Chronic or constrictive pericarditis is a less common Clinical classification of acute vs. chronic: ◦ Acute (<6 weeks) ◦ Subacute (6 weeks to 6 months) ◦ Chronic (>6 months Chest pain characteristic of pericarditis: Substernal or left precordial pleuritic Radiation to trapezius ridge Relieved by sitting up/bending forward Worsened by recumbent position or deep breath May resemble angina/MI but differs in that pain changes with body positions ◦ Other symptoms may be dry cough, fever, fatigue, anxiety ◦ ◦ ◦ ◦ ◦ Due to similarity to myocardial infarction pain, pericarditis can be misdiagnosed as an acute MI solely based on the clinical data therefore extreme suspicion on the part of the diagnostician is required Characteristic/Parameter Pericarditis Myocardial infarction Pain description Sharp, pleuritic, retro-sternal (under the sternum) or left precordial (left chest) pain Crushing, pressure-like, heavy pain. Described as "elephant on the chest." Radiation Pain radiates to the trapezius ridge (to the lowest portion of the Pain radiates to the jaw, or the scapula on the back) or no left or arm, or does not radiate. radiation. Exertion Does not change the pain Can increase the pain Position Pain is worse supine or upon inspiration (breathing in) Not positional Sudden pain, that lasts for hours or sometimes days before a patient comes to the ER Sudden or chronically worsening pain that can come and go in paroxysm or it can last for hours before the patient decides to come to the ER Onset/duration The classic sign of pericarditis is a friction rub auscultated at the left sternal border Other signs include: ◦ ◦ ◦ ◦ positional chest pain Diaphoresis pulsus paradoxus Beck’s triad: which describes three medical signs associated with acute cardiac tamponade, a medical emergency due to fluid accumulation around the heart impairing the heart’s ability to pump blood observed as: Low arterial blood pressure Jugular venous distension Distant and muffled heart sounds (narrowing of pulse pressure may also be observed) ASA/NSAIDS for viral/idiopathic causes Pericardiocentesis for effusion/cardiac tamponade Antibiotics for bacterial infections Steroids in acute pericariditis but may increase risk for recurrence constrictive pericarditis is a late sequela of an inflammatory condition of the pericaridum. The inflammatory condition is usually an infection that involves the pericardium, but it may be after a MI or after heart surgey http://en.wikipedia.org/wiki/Pericarditis http://www.medicinenet.com/pericarditis/article.htm http://www.stjosham.on.ca/media/PatientED/PT/Pericarditis-trh.pdf http://emedicine.medscape.com/article/156951-differential http://www.drugs.com/cg/chronic-pericarditis.html