Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
R. Arbeau
S. Anderson
October 21/ 2010
Case 1
ID: 3 y/o F
CC: Ingestion
HPI: Was at grandmothers house.
Grandmother was gardening and thinks
patient ingested something
Pmhx: Healthy
Rx: Nil
All: NKDA
Case 1 cont....
O/E
BP: 98/64
HR: 106
RR: 22
02: 100% on R/A
T: 37.1
Glucose: 4.5
Case 1 cont...
Exam:
GCS 15. Acting appropriately.
CV: N heart sounds
Resp: N
GI: N
CNS: N
Case 1 cont...
B/W
CBC, lytes, BUN, Cr N
Tox screen?
EKG
NSR
Case 2
ID: 17 month old
CC: ? Ingestion
HPI: Was at grandmothers house and
became fatigued. Taking lots of naps
since 15:00. Presented at 21:00
Pmhx: similar presentation 3 weeks ago
Rx: nil
All: NKDA
Case 2 cont....
O/E:
BP: 98/70
HR: 73
RR: 22
02: 100% on R/A
T: 37.4
Glucose: 5.1
Case 2 cont...
O/E:
Fatigued but easily rousable
CV: heart sounds normal
Resp: N
GI: N
CNS: No focal abnormalities
Case 2 cont...
B/W
CBC, lytes, BUN, Cr N
EKG
Sinus bradycardia
No QTC/QRS changes
Approach to Toxicology
ABC’s
IV
O2
Monitor
Approach Cont...
History
Collateral history VERY important
○ DPV
○ Paramedic reports
○ Witnesses
Physical
Track marks
Pill fragments
Look in pockets
Approach cont....
Supportive measures
Antidotes
Call Poison Control
What is a poison?
Kitchen/Laundry Area
Bathroom
Garage/Basement/Storage
Ammonia
Air Fresheners
Antifreeze*
Bleach
After-Shave Lotions
Insect Killers*
Carpet/Upholstery cleaners
Colognes/Perfumes
Fertilizers
Dishwasher Detergents
False Fingernail Removers*
Gasoline
Disinfectants
Hair Remover
Glues
Drain Cleaners*
Hair Styling Products Lotions/Creams/Oils
Kerosene
Fabric Softeners
Floor Cleaners
Furniture Polishes
Insect Killers*
Hand Sanitizer*
Makeup
Medications*
Mothballs
Lighter Fluids
Lime*
Lye*
Paints
Laundry Detergents
Mouthwash*
Paint Thinners
Metal Cleaners
Nail-Polish Removers
Pool Supplies
Oven Cleaners*
Rust Removers
Scouring Powders
Rubing Alcohol*
Shampoos
Shaving Creams
Rodent Killers
Turpentines
Weed Killers*
Spot Removers
Soaps/Deodorants
Windshield Wiper Fluids*
Spray Starches
Toilet Bowel Cleaners*
Ingestions
The dose is dependent upon
* The environmental concentration
* The properties of the toxin
* The frequency of exposure
* The length of exposure
* The exposure pathway
Toxicological Principles
Decrease absorption
Enhance elimination
Antidotes
Considerations
Change from normal state
could be on the molecular, cellular, organ, or
organism level--the symptoms
Local vs. Systemic
Reversible vs. Irreversible
Immediate vs. Delayed
Further Consideration
Routes and Sites of Exposure
Ingestion (Gastrointestinal Tract)
Inhalation (Lungs)
Dermal/Topical (Skin)
Injection
○ intravenous, intramuscular, intraperitoneal
Why is pediatrics different?
Higher mg/kg dosing based on
bodyweight
Exploratory behaviour
Everything goes into their mouths
Pediatric Toxicology
One pill killers
TCA’s
Antimalarials
Typical antipsychotics
Antidysrythmics
Ca2+ channel blockers
Beta blockers
Opiates (especially long acting)
Sulfonyureas (ie./ glyburide)
Theophylline
Lomotil (immodium)
Clonidine
One sip killers
Ethylene glycol
Methanol
Camphor
Anything containing methylsalicylate
Oil of wintergreen (100% methylsalicylate)
Ben gay
○ 1 ml of 98% methylsalicylate contains 1.4 g of
salicylate
○ One teaspoon (5ml is potentially fatal in 2 year
old)
Bradycardia in pediatric tox
Calcium channel blockers
Beta blockers
Digoxin
Cholinergic compounds (Increased
vagal tone)
Opiates (related to sedative effect)
Clonidine
Includes visine (eye drops) and nasal spray
(afferin)
Back to cases
Case 1:
3 y/o asymptomatic
Took one of grandmothers 100 mg atenolol
Cases
Case 2:
17 month old
Bradycardic
Fatigued
Took 0.1 mg of grandmothers clonidine
Beta blockers
Uses: HTN, dysrhythmias, migraines
etc...
Preparations: Oral immediate and
sustained release, IV, opthalmic
Selective (B1 – heart, eye, kidney) or
non-selective (B1 and B2
{smooth/skeletal muscle, liver, heart})
Selectivity is lost in overdose situations
Beta blockers cont...
Pharmacokinetics
May be hepatic (propanolol) or renal
elimination (atenolol, nadalol)
Onset is variable and may be delayed if
extended release formula
Beta Blockers cont...
Clinical Manifestations
Safer ingestion in younger people (those not
dependant on adrenergic tone)
Hypotension, bradycardia, CHF
Conduction disturbances (SA and AV nodal
blockade, QRS prolongation and QTC
prolongation-sotalol)
Respiratory depression
Delirium, coma or seizures (often in context of
hypotension)
More worrisome if underlying disease or coingestions
Beta Blockers cont...
Hypoglycemia may occur
Sympathetic stimulation is blocked
Gluconeogenesis is impaired so glucose
may be low
Bronchospasm
Underlying lung disease
Hyperkalemia may occur
Cause K+ efflux as beta agonists cause K+
influx
Beta Blocker Management
ABC/IV/O2/Monitor
Activated charcoal
0.5-1 g/kg
Most effective if given within one hour of
ingestion (no evidence)
Multiple doses have been recommended but
no specific evidence
Beta Blocker Management cont...
Glucagon
Inotropic and chronotropic effects
Counteracts any hypoglycemia that may
occur
5 to 10 mg IV bolus
Infusion may be needed
Atropine
Symptomatic bradycardia
0.5 mg for adults
0.02 mg/kg for children (minimum 0.1 mg)
Beta Blocker management cont….
Calcium
Pressors
Pacing
Beta Blocker Management cont...
If asymptomatic for 6 hours after an oral
overdose of normal release preparations
patients may be cleared medically
Sustained release preparations should
be admitted to a monitored bed, but are
unlikely to develop toxicity if
asymptomatic for 24 hours (ie./
carvedilol, sotalol)
Any hypotension, dysrhythmias should
be admitted to ICU/CCU bed
Calcium Channel Blockers
Pathophysiology:
Inhibit L-type Ca2+ channels
○ Decreases calcium influx into myocardial and
smooth muscle cells
○ Myocardium: Decreased contractility and
conduction
○ Peripheral: Relaxation and vasodilation of
vasculature
CCB’s pathophysiology cont..
Different affinities
○ Verapamil: greatest effects at SA and AV
nodes
○ Nifedipine: Greater effects peripherally than
on myocardium
○ Diltiazem: Moderate affinity for both
myocardial and peripheral cells
Ca2+ channel blockers cont...
Clinical Manifestations
Hypotension
Bradycardia
AV conduction delays and complete heart block
Cardiogenic shock
Hyperglycemia
○ L-type calcium channels are blocked in pancreatic
islet cells leading to decreased insulin release
CNS
○ Related to hypoperfusion
○ Noted to not have as much CNS effects as other
bradycardic medications (unsure of mechanism)
Ca2+ channel blockers cont...
Management
ABC/IV/O2/Monitor
Activated charcoal
○ 0.5-1 g/kg
○ Most effective if given within one hour of
ingestion
○ Multiple doses have been recommended
especially for extended release preparations
Ca2+ channel blockers cont...
Atropine
Symptomatic bradycardia
○ May not work well b/c AV nodal blocking effects
Calcium
Increases extracellular calcium creating a
concentration gradient promoting influx of Ca2+
into cells
Contraindicated with digoxin co-ingestion
Dosing 1g CaCl- or Ca gluconate
○ Initially 1-2 ampules
○ CaCl- provides three times as much calcium
(more sclerosis of vessels – better suited for
central venous administration)
Ca2+ channel blockers cont...
Glucagon
Activates adenyl cyclase through glucagon
receptor
Unlikely to be helpful but consider with
refractory hypotension
Pressors
NE has theoretical advantage
○ B1 adrenergic activity reverses myocardial
depressant effects
○ Alpha1 effects increase peripheral vascular
effects
Ca2+ channel blockers cont...
Insulin/glucose
Insulin may increase cardiac inotropy and
chronotropy
○ Has pressor effects that increases BP and HR
Pacing
CCB management
NEJM, Vol 344, No. 22, May, 2001
Case report of calcium channel blocker
OD’s being treated with insulin infusion
L-type channels are blocked (including
islet cells) resulting in hypoinsulinemia
In an unstressed state myocytes oxidize
FFA’s for energy, but in a stressed state
the hypoinsulinemia may prevent
glucose uptake by myocytes causing a
loss of inotropy, PVR and shock
CCB management
NEJM, Vol 344, No. 22, May, 2001
These patients were started on insulin
infusions which improved inotropy and
peripheral vascular resistance
Also thought to improve acidosis by
improving uptake of carbohydrates by
myocytes and smooth muscle cells
Ca2+ channel blockers cont...
Disposition
If asympomatic for 6 hours then may be
medically cleared
Any hypotension or dysrythmias should be
admitted
Digoxin
Cardioactive steroid
Uses: CHF, controlling ventricular
response in a-fib/a-flutter
Mechanism of action
Increases vagal tone (bradycardia and
impaired AV node conduction)
Inhibits sodium potassium exchange pump
Digoxin
Naturally occurring sources
Foxglove
Lily of the valley
Bufo toads
Oleander/yellow oleander
Dogbane
Digoxin
The Na/K+ exchange is blocked, thereby
decreasing Na+/Ca2+ exchange
In OD there is ++ intracellular Ca2+
Increases intracellular resting membrane
potential and increases dysrhythmias
Digoxin
Clinical manifestations
GI: nausea, vomiting usually first symptom
CNS: lethargy, confusion and weakness.
Halos, yellow vision in chronic overdose
situations
Metabolic: Hyperkalemia is a marker for
severe poisoning in acute overdose this is
due to blockage of Na/K ATPase, release of
K+ from tissues and inhibition of K+ uptake
into skeletal muscle
Digoxin
Cardiac manifestations
Increased automaticity with a high degree
AV block
Any dysrhythmia is possible except a rapidly
conducted supraventricular rhythm with a
rapid ventricular rate (unless patient has a
congenital accessory pathway)
Most common disturbance is PVC’s
Bidirectional V-tach is rare, but
pathognomonic
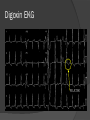
Digoxin EKG
Digoxin – Bidirectional V-tach
Digoxin
Treatment
Supportive
Charcoal
Atropine if indicated
Avoid internal electrical pacing
○ May trigger fatal dysrhythmia
Potassium/Magnesium if low
○ Magnesium contraindicated in bradycardia/AV
block
Digoxin
Definitive Treatment:
Digibind
○ Digoxin specific antibody fragments
○ Binds digoxin in serum, diffuses into interstitial
sites and creates a concentration gradient to
help digoxin dissociate from the heart
Digoxin: Digibind
Indications: Adults
Ventricular
dysrhythmia
Hemodynamically
significant
bradydysrhythmias not
responsive to atropine
Serum potassium >
5.0
Rapidly progressive
rhythm disturbances
and rising potassium
Co-ingestion of other
cardiotoxic drugs
Ingestion of plant
known to contain
cardiac glycosides
Acute ingestion of
greater than 10 mg
Indications: Children
Ingestion of greater than
0.1-0.3 mg/kg plus
rapidly progressive
symptoms or potentially
life-threatening
dysrhythmias or
conduction blocks
Co-ingestions of other
cardiotoxic drugs
Ingestion of plant known
to contain cardiac
glycosides
Digoxin
Digibind dosing
-If dose ingested known
{amount ingested (mg) * 0.8}/ 0.5 (amount
digoxin bound/vial)
-If serum concentration known
{serum concentration * weight in kg} / 100
-Empiric dosing with unknown concentration
10 vials (adult or child)
Digoxin
Treatment
Amiodarone if ventricular dysrhythmias
ACLS management
○ Electricity may worsen rhythm, but is
obviously treatment of choice in arrest
situation
○ Digibind should also be considered if not
given already
Digoxin
Disposition:
All patients who are symptomatic require at
least 12 hours of monitoring
If digibind is required then an ICU/CCU
admission is required
Clonidine
Central alpha agonist
○ Decreases NE release in brain, which
decreases sympathetic outflow causing
decreased HR, BP and cardiac output
Peripheral alpha agonist
○ In overdose
○ Post-synaptic alpha2 adrenergic agonist on
peripheral vessels. This increases NE release
causing peripheral vasoconstriction which
may cause early transient hypertension
Clonidine
Clinical Manifestations
CV: early transient hypertension followed by
hypotension and bradycardia from central
effects
CNS: Lethargy, pinpoint pupils
Respiratory: Hypoventilation, hypoxia,
periodic apnea, Cheyne Stokes respiration
Clonidine
Treatment
ABC/IV/O2/Monitor
Supportive
Charcoal
Naloxone: may reverse some or all of the
sedation associated (mechanism unclear). May
need large doses (ie./ 200 mg in 24 hours)
For hypotension:
○ IV fluids initially
○ Atropine
○ Consider pressors in refractory hypotension
Clonidine
Admission if any symptoms for
monitoring
Monitored for 6-8 hours if asymptomatic
Cholinergic Syndrome
Bradycardia may caused by action on
muscarinic receptors
Should be easily recognized and
differentiated from other exposures
Bradycardia Comparison
Drug
Temp
BP
Pupil
s
CNS
K+
Skin
Bowe Urine
l
Glu. EKG
CCB
N/E
Dec
N/E
+/-
+/-
N/E
N/E
N/E
Inc
Brady
AV blocks
Bblock
N/E
Dec
N/E
Dec
Inc
N/E
N/E
N/E
Dec
Brady, AV
blocks
Dig
N/E
+/-
Halo
Dec
vision,
yellow
haze
Acute
Inc.
N/E
N/E
N/E
N/E
PVC’s,
Scooped
ST’s, bi
directional
VT
Chron
ic
Dec
Cholin N/E
ergic
+/-
miosis Dec
+/-
Wet
Inc
Urinat N/E
ion
Brady
Clonid N/E
ine
Dec
pinpoi Dec
nt
+/-
N/E
N/E
N/E
Brady
N/E
Back to cases
Case 1:
3y/o F
Took grandmothers atenolol
Poison control contacted
Given charcoal
Remained asymptomatic
Transferred to Peds ER for observation
Discharged home after 6 hours of
observation
Cases
Case 2:
17 month old
Ingested 0.1 mg clonidine
Fatigued, bradycardia
Given charcoal
Narcan was advised, but not given
Atropine was given with minimal effect
Admitted to PCCU and monitored for 36 hours
HR increased with no further intervention
required
References
Rosens
Boyer & Shannon. Treatment of Calcium channel blocker
intoxication with insulin infusion. NEJM. Vol. 344, No. 22,
2001
New York City Poison Control Handbook
Questions?