Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
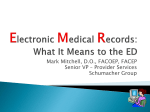
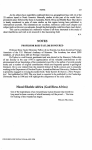
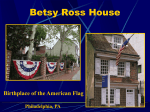
The Management of ED TIA Patients: Michael A. Ross MD FACEP Associate Professor Emergency Medicine Department of Emergency Medicine William Beaumont Hospital Wayne State University School of Medicine Michael Ross, MD, FACEP Case presentation • A 58 year old female presents to the emergency department after developing dysarthria, diploplia, numbness, and pronounced weakness of the right face and hand that lasted roughly 12 minutes. The patient feels completely normal and only came in at her families insistence. – Review of systems - mild headache with event. No palpitations, chest pain, or SOB. – Past medical history - Positive for hypertension and hyperlipidemia. No prior stroke or TIA. – Family history positive for premature coronary disease. – Meds - Beta-blocker for HTN. Not on aspirin. – Social - She does not smoke. Michael Ross, MD, FACEP Case presentation • Phyisical Exam: On examination the patient was normotensive, and comfortable. • HEENT exam showed no facial or oral asymmetry or numbness. No scalp tenderness. • CHEST exam showed no murmurs and a regular rhythm, • ABDOMINAL and EXTREMITY exam was normal, • NEUROLOGICAL exam showed normal mentation, CN IIXII normal as tested, motor / sensory exam normal, symmetrical normal reflexes, and normal cerebellar exam. Michael Ross, MD, FACEP Case presentation • ED course: – ECG showed a normal sinus rhythm with mild LVH. – Non-contrast head CT scan was normal. – Blood-work (CBC with differential, electrolytes, BUN/Cr, and glucose) was normal. ESR was normal. – Monitor showed no dysrhythmias – Normal subsequent neurological symptoms. – The patient feels fine and is wondering if she can go home. What do you think? Michael Ross, MD, FACEP Background • 300,000 TIAs occur annually - Johnstons’ data • Within 90 days: • 10.5% will suffer a stroke _ 21% will be fatal _ 64% will be disabling _ Half of these will occur within 1 - 2 days of ED visit • 2.6% will die • 2.6% will suffer adverse cardiovascular events • 12.7% will have additional TIAs Michael Ross, MD, FACEP Stroke Risk After TIA Year Johnston, et al (Kaiser ED)2000 Eliasew, et al (NASCET) 2004 Lovett, et al (Oxfordshire) 2004 Gladstone, et al (Toronto) 2004 Daffertshofer, et al (Grmy) 2004 Hill, et al (Alberta) 2004 Lisabeth, et al (Texas) 2004 Kleindorfer, et al (Cinc) 2005 Whitehead, et al (Scotland)2005 Correia, et al (Portugal) 2006 Tsivgoulis, et al (Greece) 2006 AVERAGE N 1707 603 209 371 1150 2285 612 927 205 141 226 Stroke Risk 10.5% /90d 20.1% /90d 12% /30d 5% /30d 13% /180d 9.5% /90d 4.0% /90d 14.6% /90d 7% /30d 13% /7d 9.7% /30d ~12% stroke risk in 90 days after TIA 5% in first 2 days Michael Ross, MD, FACEP Stroke Risk After Stroke IST CAST TOAST NASCET 3.3 %/ 3m 1.6%/ 3m 5.7%/ 3m 2.3%/3m AVERAGE ~4% stroke risk in 90 days after stroke Michael Ross, MD, FACEP Pathophysiology • Short-term risk of stroke: – After TIA (11%) > after stroke (4%) • Possible explanation – Tissue still at risk: unstable situation • More thrombo-embolic events Johnston, NEJM 2002; 347:1687 Michael Ross, MD, FACEP Possible Explanation: Instability Michael Ross, MD, FACEP Possible Explanation: Instability Michael Ross, MD, FACEP Outside the “head”: Cardio-embolic sources Michael Ross, MD, FACEP Background • Stroke is preceded by TIA in 15% of pts • Stroke is the THIRD leading cause of death – National cost of stroke = $51 billion annually! – Many consider stroke to be worse than death. Michael Ross, MD, FACEP TIA STROKE Michael Ross, MD, FACEP Topics to be covered 1. Appropriate history, physical, and labs 2. ECG, monitor, HCT 3. Carotid dopplers - why, when, how? 4. Further clinical testing 5. Therapy – starting with aspirin Michael Ross, MD, FACEP TIA Definition • Traditional – Neurological deficit lasting less than 24 hours due to focal ischemia in the brain or retina. • Newly Proposed – – – – A brief episode of neurologic dysfunction caused by focal brain or retinal ischemia, with clinical symptoms typically lasting less than 1hr, and without evidence of acute infarction”. • If TIA symptoms last >1hr, then >85% have a stroke – NINDs tPA study data - Albers et al. Michael Ross, MD, FACEP 1. History and physical: The History • Duration - <10min, 10-60min, >60 min • Evidence to suggest non-vascular cause? – Focal vs. non-focal symptoms – Abrupt vs. gradual symptom onset • Vascular risk factors? – DM, prior “CVA-TIA-MI-PVD” • Symptoms to suggest potential causes? – Neck pain - dissection – Palpitations - atrial fibrillation Michael Ross, MD, FACEP Evaluation: Physical examination • Neurologic deficits? • Carotid bruits (note limitations)? • Cardiac abnormalities? – Arrhythmia – Murmur – Signs of heart failure • Symptoms reproducible with provocative maneuvers? – Cervical stretch test – Carpal tunnel positioning tests Michael Ross, MD, FACEP Neurological Exam • Six major areas – MS, CN II-IX, Motor, Sensory, Reflex, Coordination • NIH stroke score – Structured neurological exam – Validated tool for detection of significant deficits – Value as an educational tool – Thrombolytic screening tool – Google - “NIHSS training”: http://asa.trainingcampus.net/uas/modules/trees/windex.aspx – Google - “FERNE” website: http://www.ferne.org/ Michael Ross, MD, FACEP Evaluation: Laboratory testing • Complete blood count – anemia, polycythemia, thrombocytosis/thrombocytopenia • Chemistry panel – hypoglycemia, diabetes, renal failure • Sedimentation rate – temporal arteritis, endocarditis • EKG – prior MI, atrial fibrillation Michael Ross, MD, FACEP Unstable plaque with intense staining for PAPP-A within spindle shaped smooth muscle cells and in extracellular matrix of eroded plaque Stable plaque with absence of PAPP-A staining Unstable plaque ; Lp-PLA2 Candidate Blood Markers??? Unstable Plaque: Lp-PLA2, PAPP-A, MMP-9, CRP, S-TF Coagulation Activation: D-dimer, F 1.2, TAT Cardioembolism: BNP (CHF), D-dimer Michael Ross, MD, FACEP TIA: Differential Diagnosis “Mimics” • • • • • Epilepsy Complicated migraine Subdural hematoma Mass lesions, AVMs Arterial dissection • Cervical disc disease • Carpal tunnel syndrome • Metabolic derangement (ex, hypoglycemia) • Inner ear disease/BPV • Transient global amnesia • Cranial arteritis Oxfordshire Community Stroke Project found that 62% of patients referred by GP with a diagnosis of TIA were found to have some other explanation for symptoms (Dennis M, Stroke 1989) Michael Ross, MD, FACEP Is a “TIA” a TIA? • Little agreement, even among neurologists (kappa 0.25-0.65) • Generally, neurologists are not the ones making the diagnosis – May even be less reproducibility • Risk factors for stroke may identify true TIAs Johnston et al, Neurology 2003; 60:280 Michael Ross, MD, FACEP Utility of the H/P? • TIA risk stratification – Johnston criteria – Rothwell criteria - “ABCD” – Combination of the above = “ABCD2” Michael Ross, MD, FACEP TIA risk stratification - California Model Johnston et al. Short-term prognosis after emergency department diagnosis of TIA. JAMA. 2000;284:2901-6. Independent risk factors for stroke: • Age > 60yr (OR = 1.8) • Diabetes (OR = 2.0) • TIA > 10 min. (OR = 2.3) • Weakness with TIA (OR = 1.9) • Speech impairment (OR = 1.5) Risk factors were additive Michael Ross, MD, FACEP Our patient’s Johnston score? Independent risk factors for stroke: • Age > 60yr 0 • Diabetes 0 • TIA > 10 min. 1 • Weakness with TIA 1 • Speech impairment 1 stroke risk score of 3: ~5% at one week ~8% at 3 months Michael Ross, MD, FACEP TIA risk stratification - British model? Rothwell,et al. Lancet 2005; 366: 29–36 • A = Age >60 years • B = BP: SBP >140 or DBP >90 • C = Clinical: – Unilateral weakness – Speech disturbance • D = Duration – >60 min – 10 – 59 min – <10 min = 1pt = 1pt = 2pt = 1pt = 2pt = 1pt = 0pt Michael Ross, MD, FACEP Michael Ross, MD, FACEP Our patients ABCD score? • A = Age >60 years =0 • B = BP: SBP >140 or DBP >90 =0 • C = Clinical: – Unilateral weakness = 2pt – Speech disturbance = 1pt • D = Duration – >60 min =0 – 10 – 59 min = 1pt – <10 min =0 • TOTAL SCORE = 4 (5% risk of stroke at one week) Michael Ross, MD, FACEP ABCD2 Score Michael Ross, MD, FACEP ABCD2 Score Score points for each of the following: – Age >60 (1) – Blood pressure >140/90 on initial evaluation (1) – Clinical: • Focal weakness (2) • Speech impairment without weakness (1) – Duration • >60 min (2) • 10-59 min (1) – Diabetes (1) Final Score 0-7 Michael Ross, MD, FACEP ABCD2 Score Validation: Meta-analysis Variable Age >60 years Diabetes mellitus SBP >140 mmHg or DBP >90 mmHg Duration 10-59 min vs. <10 min Duration >60 min vs. <10 min. Speech impairment without focal weakness Focal weakness No (%) 2-Day Risk 7-Day Risk 90-Day Risk Odds Ratio (95% CI) Odds Ratio (95% CI) Odds Ratio (95% CI) 3690 (76.7) 1.4 (1.0 -2.1) 1.4 (1.0 -2.0) 1.5 (1.2 -2.0) 797 (16.6) 1.6 (1.1 -2.2) 1.4 (1.1 -1.9) 1.7 (1.3 -2.1) 3420 (71.2) 2.1 (1.4 -3.1) 1.9 (1.4 -2.6) 1.6 (1.2 -2.0) 993 (20.7) 2.0 (1.0 -3.7) 1.9 (1.1 -3.3) 1.7 (1.1 -2.5) 2973 (61.9) 2.3 (1.3 -4.0) 2.6 (1.6 -4.3) 2.1 (1.5 -3.0) 899 (18.7) 1.4 (0.8 -2.3) 1.5 (1.0 -2.4) 1.7 (1.2 -2.3) 1979 (41.2) 2.9 (2.0 -4.3) 3.5 (2.5 -4.8) 3.2 (2.5 -4.1) *All listed independent predictors were included in logistic regression analysis. Michael Ross, MD, FACEP ABCD2 Score and Stroke Risks 25% Stroke Risk 20% 2-Day Risk 15% 7-Day Risk 30-Day Risk 10% 90-Day Risk 5% 0% 0 1 2 3 4 5 6 7 ABCD2 Score Michael Ross, MD, FACEP Prognosis Conclusions • The ABCD2 Score stratifies short-term risk of stroke after TIA – 2-day risks • Low Risk (34%): • Moderate Risk (45%): • Very High Risk (21%): Score 0-3 1% Score 4-5 4% Score 6-7 8% • “This rule is ready for clinical use” – C. Johnston Michael Ross, MD, FACEP What is our patients’ ABCD2 score? – Age >60 – Blood pressure >140/90 (initial) (1) – Clinical: • Focal weakness (2) • Speech impairment without weakness (1) – Duration • >60 min (2) • 10-59 min (1) – Diabetes (1) =0 =0 =2 =0 =0 =1 =0 • Total = 3 – Stroke at 2 days = 1% – Stroke at 7 days = 2% (?!) Michael Ross, MD, FACEP Limitations of Prediction Rules • Discriminatory value sub-optimal – What about the patient with 90% carotid stenosis and a low score??? • Generalizability seems poor (though exact reasons for this unclear) • Are these rules really just selecting patients with “real” TIAs? Michael Ross, MD, FACEP 2. HCT, ECG • HCT - tumor, SDH, NPH, etc – Minor stroke and TIA associated with a 10% incidence of stroke on MRI. Michael Ross, MD, FACEP Infarction in TIA • Approximately 50% of those with TIA have DWI changes on MRI Kidwell et al Stroke 1999 Michael Ross, MD, FACEP When is a “TIA” a TIA? • What about when a clinically silent acute infarct is present? – New infarct on CT as a predictor of stroke: • 38% with new infarct had a stroke within 90 days vs. 10% without (p=0.008). • OR 4.1 after adjustment for clinical factors. – Recently, new infarct on MRI also shown to be a predictor. • 5-fold increase in risk with new lesion on baseline MRI • Also, greater risk of in-hospital stroke in a second cohort. VC Douglas et al, Stroke 2003; 34:2894 SB Coutts et al, Neurology 2005; 65:513 H Ay et al, Ann Neurol 2005; 57:679 Michael Ross, MD, FACEP Recovery Stroke Neurologic Deficit Stroke? TIA Time Michael Ross, MD, FACEP 90-day risk of stroke in patients with a small stroke vs TIA? Lancet Neurol 2006; 5: 323–31 Michael Ross, MD, FACEP Reversible ischemia Infarction Minor stroke DWI+ TIA TIA Reversible ischemic neurologic deficit (RIND) Stroke Cerebral infarction with transient signs Michael Ross, MD, FACEP 2. HCT, ECG • ECG – ATRIAL FIBRILLATION!!! – Stroke risk – cardio-embolic risk • 4.6% at 1 month • 11.9% at 3 months – 61% reduction in annual risk of stroke (both ischemic or hemorrhagic) with coumadin Michael Ross, MD, FACEP 3. Carotid Dopplers Stroke risk depends on where the disease is: 7day 90day CE = Cardio-Embolic: 2.5% 12% LAA = Large arteries 4.0% 19% Und = Undetermined 2.3% 9% SVS = Small Vessels 0% 3% Michael Ross, MD, FACEP 3. Carotid dopplers The BIG question - WHEN??? • Carotid surgery if >70% stenosis lesions is “time sensitive”. • Stroke risk reduction if done within: – 0-2 weeks • 75% stenosis = 30.2% – 2-4 weeks • 75% stenosis = 17.6% – 4-12 weeks • 75% stenosis = 11.4% – +12 weeks • 75% stenosis = 8.9% • Similar for 50-70% lesions Michael Ross, MD, FACEP Outpatient carotid dopplers? Office management of TIA??? Goldstein et al. New transient ischemic attack and stroke: outpatient management by primary care physicians. Arch Intern Med. 2000;160:2941-6. • Design: – Retrospective study of 95 TIA and 81 stroke patients seen in office • Diagnostic testing within 30 days: – 23% had head CT done – 40% had carotid dopplers done – 18% had ECG done – 19% had echo done – 31% had no other evaluation Michael Ross, MD, FACEP 4. Further Clinical testing? • Serial neurological exams? – 10.5% stroke within 3 months • Half within 2 days • Most within 1 day • Monitoring for AF? • 2-D echo? Michael Ross, MD, FACEP 4. Further clinical testing 1 Strokes Probability of Survival .9 .8 Adverse Events .7 .6 0 7 30 60 90 1480 1293 1451 1248 Days after TIA No. of Patients At Risk For: St roke Adverse Events 1001 1001 1577 1462 1527 1361 Johnston et al, JAMA 284:2901 5. Medical management Antiplatelet Therapy • Useful in non-cardioembolic causes –Aspirin 50-325 mg/day –Clopidogrel or ticlopidine –Aspirin plus dipyridamole •Latter two if ASA intolerant or if TIA while on ASA • Routine anticoagulation not recommended Michael Ross, MD, FACEP 5. Medical management Risk Factor Management • • • • • • • HTN: BP below 140/90 DM: fasting glucose < 126 mg/dl Hyperlipidemia: LDL < 100 mg/dl Stop smoking! Exercise 30-60 min, 3x/week Avoid excessive alcohol use Weight loss: < 120% of ideal weight Michael Ross, MD, FACEP Hospital Admission for TIA • Medical management to minimize risk of recurrent ischemia • Expedite evaluation and treatment of specific mechanisms – CEA for carotid stenosis, anticoagulation for atrial fibrillation • Observation for further events, with potential expedited thrombolysis • Avoid the lawyers Michael Ross, MD, FACEP Michael Ross, MD, FACEP Management of TIA: • Areas of Certainty: – Need for ED visit, ECG, labs, Head CT • Areas of less certainty – The timing of the carotid dopplers • Areas of Uncertainty - Johnston SC. N Engl J Med. 2002;347:1687-92. – “The benefit of hospitalization is unknown. . . Observation units within the ED. . . may provide a more cost-effective option.” Michael Ross, MD, FACEP An Emergency Department Diagnostic Protocol For Patients With Transient Ischemic Attack: A Randomized Controlled Trial To determine if emergency department TIA patients managed using an accelerated diagnostic protocol (ADP) in an observation unit (EDOU) will experience: shorter length of stays lower costs comparable clinical outcomes . . . relative to traditional inpatient admission. Michael Ross, MD, FACEP Patient population: • Presented to the ED with symptoms of TIA • ED evaluation: – History and physical – ECG, monitor, HCT – Appropriate labs – Diagnosis of TIA established • Decision to admit or observe • SCREENING AND RANDOMIZATION Michael Ross, MD, FACEP Methods: ADP Exclusion criteria • • • • • • • • • • • Persistent acute neurological deficits Crescendo TIAs Positive HCT Known embolic source (including a. fib) Known carotid stenosis (>50%) Non-focal symptoms Hypertensive encephalopathy / emergency Prior stroke with large remaining deficit Severe dementia or nursing home patient Social issues making ED discharge / follow up unlikely History of IV drug use Michael Ross, MD, FACEP Methods: ADP Interventions • Four components: – Serial neuro exams • Unit staff, physician, and a neurology consult – Cardiac monitoring – Carotid dopplers – 2-D echo • BOTH study groups had orders for the same four components Michael Ross, MD, FACEP Methods: ADP Disposition criteria • Home – No recurrent deficits, negative workup – Appropriate antiplatelet therapy and follow-up • Inpatient admission from EDOU – Recurrent symptoms or neuro deficit – Surgical carotid stenosis (ie >50%) – Embolic source requiring treatment – Unable to safely discharge patient Michael Ross, MD, FACEP Results Michael Ross, MD, FACEP Results: Patient Characteristics Mean Age (sd) Male n (%) TIA Stroke Risk Factors - mean (sd) * Median (IQR) Initial ED Length of Stay * Johnston Inpatient Total n=74 67.7yr (15.4) 34 (46%) 2.7 (1.4) 6.2 hrs (5.0-6.2) TIA-ADP Total n=75 68.4yr (15.3) 31 (41%) 2.4 (1.1) 5.7 hrs (4.5-5.5) - JAMA. 2000;284:2901-6. Michael Ross, MD, FACEP Results: Performance of clinical testing Inpatient (n=74) TIA-ADP (n=75) 67 (90.5%) 25.2 hr (17.3 – 37.1) 73 (97.3%) 13.0 hr (8.4 – 18.0) 54 (73%) 43.0 hr (23.8 – 63.8) 73 (97.3%) 19.1 hr (16.7 – 22.5) Carotid imaging Number completed (n, %) Time to completion Echocardiography Number completed (n, %) Time to completion Michael Ross, MD, FACEP Results: Length of Stay Inpatient ADP Median = 61.2 hr = 25.6 hr Difference = 29.8 hr (Hodges-Lehmann) (p<0.001) ADP sub-groups: ADP - home = 24.2 hr ADP - admit = 100.5 hr Results: 90-Day Clinical Outcomes 90 Day Outcomes Related return visits Clinical Outcomes Index visit CVA Subsequent CVA (90 day) Total 90 day CVA Related Major event or MACE Inpatient Total n=74 9 (12%) TIA-ADP Total n=75 9 (12%) 5 2 7 (9%) 4 7 3 10 (13%) 4 Michael Ross, MD, FACEP Results: 90 - day Costs Inpatient ADP Median = $1548 = $890 Difference = $540 (Hodges-Lehmann) (p<0.001) ADP sub-groups: ADP - home = $844 ADP - admit = $2,737 Study conclusion: Compared to inpatient admission, the ED TIA diagnostic protocol was: • More efficient • Less costly • With comparable clinical outcomes Michael Ross, MD, FACEP Implications • National feasibility of ADP: – 18% of EDs have an EDOU – 220 JCAHO stroke centers • National health care costs – Potential savings if 18% used ADP: • $29.1 million dollars – Medicare observation APC • Impact of shorter LOS – Patients – satisfaction, missed Dx . . . – Hospitals – bed availability Michael Ross, MD, FACEP CLINICAL CASE - OUTCOME • The patient was started on aspirin and admitted to the ED observation unit. • While in the unit she had a 2-D echo with bubble contrast, that was normal. She had no arrhythmia detected on cardiac monitoring and no subsequent neurological deficits. • However, carotid dopplers were abnormal. She showed 30-50% stenosis of the right internal carotid artery, and a severe flow limiting >70% stenosis of the left carotid artery at the origin of the internal carotid artery. • She was admitted to the hospital for endarterectomy. Five days following ED arrival, and following inpatient pre-operative clearance, she underwent successful endarterectomy. • On one month follow-up she was asymptomatic and her carotids were doing well. Michael Ross, MD, FACEP Who do you send home from the ED??? • C. Johnston: – “TIA risk score does not identify a “zero” risk group” – But it is a good start. . . • Possibly: – Negative ED work-up (ECG, exam, CT), low TIA score, negative carotid dopplers within 6 months, safe home support for return in next 48 hours if needed? • Appropriate medications. Michael Ross, MD, FACEP Who do you send home from the ED??? • Ron Krome: – “It doesn’t matter what you do, as long as you are right” • If you are not sure, better play it safe. . . – Admit or observe Michael Ross, MD, FACEP Conclusions • TIAs are ominous – Justifies acute interventions, including hospitalization – Opportunity to prevent injury but trials are needed • Recovery rather than complete resolution is likely the important distinguishing characteristic and may identify an unstable pathophysiology • “TIAs” are heterogeneous – Management should be individualized – Prognostic scores may help • Secondary prevention is critical Michael Ross, MD, FACEP