Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
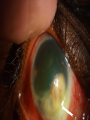
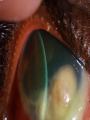
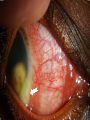
Case presentation By :Saad Aldahmash,MD History A 24 years old Saudi young man came to KKESH E.R on January 2008 ( 3 months) wih Hx of : *redness on –off OD for 1 year . *gradual decrease in VA OD over the last 1 year. *Past ocular Hx was unremarkable. *Past medical and surgical Hx was unremarkable. Family , social History *His youngest brother died at age of two years because of chronic cough . * He is living in Riyadh in a small house acomodating 12 persons. He was Examined at that time at KKESH E.R : *VA … OD 20/70 OS 20/20 *IOP… OD 18 mmHg. OS 16 mmHg. *SLE …OD: mutton fat KPs , +3 cells , vitritis . OS :quiet eye . B-scan done , showed :only vitreous haze in OD. He was diagnosed at that time as a case of : *unilateral Granulomatous panuveitis OD. *They started to investigate him. *The patient lost his follow up , didn’t show . The patient came again to the E.R at KKESH last week with a Hx : *Increased Pain ,redness and marked reduction of VA in OD. *the patient give a Hx of recent weight loss. Examination : VA … OD HM OS 20/20 IOP… OD 56 mmHg . OS 18 mmHg . SLE … OD: corneal edema,scleritis with scleral melting,mutton fat KPs ,shallow A/C, +4 cells, 360 post. Synechiae , limbal lesion, no view to post. Pole. SLE… OS : unremarkable. B-scan OD : significant vitreous haze . UBM : showed ciliary body lesion extending from 3 o’clock to 8 o’oclock position , 360 synaechial angle . *PPD test ( 5 iu): 10 mm enduration. *ESR : 67 mm/hr. *CRP : Positive . *ACE : normal value. *HIV, TPHA,RPR : Negative. *Iron deficiency anaemia . *CBC: wbc 13.6 Hb 9.7 mg/dl. *High serum urea and creatinine , low K. *CT chest: multiple foci of inactive (most likely)TB granulomas. • The Diagnosis : *Tuberculous panuveitis. *Ciliary body , limbus, scleral Tuberculous granuloma . * Secondary angle closure glaucoma . Ocular Tuberculosis review *Actually ,TB can affect any structure of the eye and adnexia . *Ocular structures are highly vascularized , high affinity for TB bacilli. *Diagnosis of ocular TB is very challenging. * Most of the times no associated concurrent active systemic disease. Review of the litreature *conjunctival granuloma. *chronic conjunctivitis. *Periorbital osteomyelitis. *orbital granuloma with enophthalmos. *Orbital Psudotumor like picture. *Endogenous endophthalmitis. *panophthalmitis. *orbital abscess. *Preseptal cellulitis . *Retinoblastoma like picture. *Dacryoadenitit. *Dacryocystitis. *NLD obstruction due to nasal granuloma. *Primary lid tuberculoma. *Myositis. *Phlectenulosis. *Scleritis. *keratitis , PUK. *spontaneous globe perforation. *Anterior uveitis ( granulomaous , non granulomatous ). *Angle , ciliary body granuloma. *Vitritis. *papillitis. *Optic disc tubercle. *Primary vascular occlusion without vasculitis. *vasculitis. *multifocal choroiditis,chorioretinitis,retinitis. *Choroidal tuberculoma without choroiditis ( similar to metastatic choroidal lesions). WHO *Because of the increase of HIV No of patients. *emergence of multidrug resistant strains. *poor countries where TB is endemic(or epidemic). *easy migration between countries . *late diagnosis (presentation) because of the masking effect of some antibiotics . *All previous factors led to an increase in the TB incidence all over the world. *TB nowadays, not as before in India ,Africa ,Indonesia….. It is becoming not uncommon infection in the US, Europe , also. TB in KSA *There were some reports from madina area of multidrug resistant Mycobacteria tuberculosis. *Early diagnosis is very important to decrease the morbidity, mortality, avoid high bacterial load of mycobacterium tuberculosis which make eradication more difficult. Conclusion *TB can mimic many ocular ,adnexal pathologies. * TB must be in the differential diagnosis of any inflammations ,tumors and vascular disorders affecting the globe and it’s adnexa. Thank you