Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Xenoestrogen wikipedia , lookup
Breast development wikipedia , lookup
Mammary gland wikipedia , lookup
Neuroendocrine tumor wikipedia , lookup
Human chorionic gonadotropin wikipedia , lookup
History of catecholamine research wikipedia , lookup
Hyperthyroidism wikipedia , lookup
Bioidentical hormone replacement therapy wikipedia , lookup
Triclocarban wikipedia , lookup
Hyperandrogenism wikipedia , lookup
Adrenal gland wikipedia , lookup
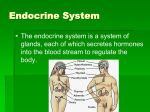
LAB BASICS Endocrinology July 30 2008 Objectives for this topic •To review how the laboratory can be used in the assessment of a patient with endocrine abnormalities. •To review some the basic chemical structures of major hormones. •To review some principles of immunoassay methods used in hormone measurements. •To review what is available from the laboratory at LHSC and to understand some of the limitations of laboratory analyses. CHEMICAL MESSENGERS Neurotransmitters Chemicals used to relay, amplify and modulate electrical signals between a neuron and another cell. Synthesized endogenously i.e. within the presynaptic neuron Hormones Chemical messengers from one organ (or group of cells) to another. Cytokines Peptides used as messengers between cells and for controlling the inner environment at the cellular level. Cytokines • Cytokines that mediate natural immunity Type 1 IFN TNF IL-1, IL-6 Chemokines Cytokines that regulate Lymphocyte activation, growth and differentiation IL-2, IL-4, TGFß Cytokines that regulate Immune-mediated Inflammation IFNγ , Lymphotoxin, IL-5, IL-10, IL-12 Migration inhibition factor (MIF) Cytokines that stimulate Hematopoiesis C-Kit Ligand IL-3. IL-7 GM-CSF, M-CSF, G-CSF, other CSF’s (colony stimulating factors) Eythropoietin Neurotransmitters Transmitter Molecule Derived From Site of Synthesis Acetylcholine Choline CNS, parasympathetic nerves Serotonin 5-Hydroxytryptamine (5-HT) Tryptophan CNS, chromaffin cells of the gut, enteric cells GABA Glutamate CNS Glutamate CNS Aspartate CNS Glycine spinal cord Histamine Histidine hypothalamus EPINEPHRINE Tyrosine adrenal medulla, some CNS cells NOREPINEPHRINE Tyrosine CNS, sympathetic nerves DOPAMINE Tyrosine CNS Adenosine ATP CNS, peripheral nerves ATP NITRIC OXIDE, NO sympathetic, sensory and enteric nerves Arginine CNS, gastrointestinal tract The sites of the principal endocrine glands Principal endocrine glands of the human body, their secretion, function and type Transport of Hormones Peptide/Protein Hormones -hydrophilic, dissolve in water Steroid & Thyroid Hormones - require carrier proteins • • • • CBG - cortisol, TBG - thyroid hormones, SHBG - sex hormones Some are highly specific binding proteins Albumin - low affinity, high capacity carrier Equilibrium between bound and free forms of the hormone, only the free form can bind to receptors • The physiological state corresponds to the concentration of free hormone Control of Endocrine System Simple - self limiting signal, effect is self limited May or may not have ‘threshold’ to limit noise Negative Feedback - signal induces response, response inhibits production of signal Positive Feedback - response feeds back to induce more signal. Amplification continues until system can no longer respond, or until signal removed Inhibitory Control - release of hormone control by an inhibitor. Remove inhibitor to allow release Endocrine Rhythms – daily, monthly, seasonal rhythms, external cues can modify rhythms Disorders of the Endocrine System Oversecretion, – loss of feedback control – exogenous secretion (another, usually uncontrolled, source - “ectopic”) Undersecretion – loss of stimulation – organ failure Disordered metabolic pathway – reduced end product, increased intermediates (may have endocrine activity), blocked from end product May affect growth, development, metabolism, behaviour ECTOPIC HORMONES • These are hormones or hormone-like products, produced by tumors located outside of the gland that normally produces them. Biochemical structure of hormones • • Steroid Hormones Lipid soluble – Diffuse directly into cells – Are derived from cholesterol – EXAMPLE - CORTISOL • Non-steroid hormones – – – – – – Water soluble Receptors on the cell surface Amines (Example catecholamines) Peptides (eg. ACTH, ADH, Oxytocin) Proteins (eg. GH, Insulin, Prolactin Glycoproteins (eg. FSH, LH, TSH) NOTE: Peptide hormones can exist in different molecular forms. Not all forms are biologically active MEASUREMENT OF HORMONE CONCENTRATIONS Bioassays Measure biological response of hormone in vivo system, tissue culture or whole animal Time consuming, technically demanding, poor accuracy and precision Chemical Reactions Obsolete Examples are PBI for thyroxine, fluorometric assays for serum cortisol, urinary ketosteroids and ketogenic steroids, Pisano reaction for VMA, HIAA and others Measures concentration or amount excreted, not activity MEASUREMENT OF HORMONE CONCENTRATIONS Chromatography Works well for small molecules, especially those from the adrenal medulla, example VMA, catecholamines HPLC introduced in 1976 for clinical applications LC/MS/MS becoming method of choice for small analytes Immunoassays Poly or monoclonal. High throughput, accuracy and precision. Measures concentration not activity. Many hormones are measured by Immunoassay Works best for larger molecules, especially proteins. Specificity an issue when differentiating a hormone from an inactive metabolite. COMPETITIVE IMMUNOASSAY Most hormones are measured by immunoassay • Basic Components of immunoassay – The analyte to be measured. – One or more antibodies or binding agent specific to the analyte to be measured. – A label (detection system). COMPETITIVE IMMUNOASSAY • The tracer molecule is attached to the antigen. • After an incubation period where equilibrium is obtained, an agent is added to separate the bound from the free analyte. • A pellet may be obtained by centrifugation that contains only the bound fraction, the free fraction is discarded. • Because of the competition, the amount of tracer in the pellet is inversely proportional to the amount of analyte in the sample. The higher the concentration in the sample the less of the tracer will be able to bind to the binding agent. COMPETITIVE IMMUNOASSAY • Competitive radio immunoassay – standard curve. Estriol in first trimester uE3 calibration Second Trimester 120000 120000 100000 100000 80000 Counts 80000 60000 60000 40000 40000 20000 20000 0 0.00 10.00 20.00 30.00 40.00 50.00 60.00 0 0.00 1.00 2.00 3.00 4.00 5.00 Estriol Values 2nd trimester assay AutoDelfia • Ideal RIA curve non-ideal RIA curve • The label in the bound fraction is inversely proportional to the concentration of analyte. 6.00 COMPETITIVE IMMUNOASSAY • Binding agents in a competitive immunoassay may be: – Second antibody (e.g. mouse anti-rabbit) – Charcoal – Biotin – Coated tube technology – Antibodies attached to magnetic beads – Poly ethylene glycol (PEG) protein precipitation Non-competitive Immunoassays • For competitive immunoassay the antibody concentration is LIMITED. • For non-competitive immunoassays the antibody is in EXCESS. This means that all the analyte will be bound to the antibody. Label is usually on a second antibody. The label in the bound fraction is directly proportional to the concentration of the analyte to be measured. NON-COMPETITIVE IMMUNOASSAYS • ALL OF THE ANALYTE BINDS TO AN UNLIMITED CONCENTRATION OF LABELLED ANTIBODY. • THE BOUND FRACTION IS DIRECTLY PROPORTIONAL TO THE CONCENTRATION OF THE ANALYTE Non-competitive immunoassay Non-competitive immunoassay HCG assay by two site Fluoroimmunometric assay 5000000 Counts 4000000 3000000 2000000 1000000 0 0.00 5.00 10.00 HCG KIU/L 15.00 NON-COMPETITIVE IMMUNOASSAY(SANDWICH TYPE) No competition step in the procedure Uses larger amounts of Ab All the analyte will be bound to the antibody (solid phase Ab). 2nd Ab (tracer) binds to distinct epitope on analyte The label in the bound fraction (signal) is directly proportional to the concentration of the analyte to be measured. Better suited to monoclonal Ab Can be easily automated on large chemistry platforms Includes ELISA type assays Immunoassay labels • Radioisotopes, such as I125, Co60, P32, H3 etc. • Fluorophor labels such as Eu (europium chelates). • Enzymes such as ALP, firefly luciferase, G6PDH that can generate a colored complex if incubated with the correct substrate following the separation step. • Cofactors such as ATP, FAD. • Free Radicals such as Nitroxide • Inhibitors such as methotrexate • Metals such as gold sol, selenium, silver sol. • Particles such as bacteriophages, erythrocytes, latex beads. • Polynucleotides such as DNA • Enzyme substrates such is Galactosyl-umbelliferone Endocrine Laboratory LLSG • Hypothalamus – Secretes small labile peptides that cannot be measured in peripheral blood. – Cortrasyn, TRH, GnRH, GHRH are given to a patient to measure pituitary response. (CIU consult) – Note that many anti-psychotic drugs block dopamine (aka PIF) secretion and lead to an increase in serum prolactin levels. Psychiatrists often measure prolactin level as “Therapeutic Drug Monitoring”. Endocrine Laboratory LLSG • Anterior Pituitary – – – – – – – TSH, measured daily on the Siemens Centaur LH, Siemens Centaur FSH, Siemens Centaur GH, Immulite 2000 (Siemens) ACTH, IRMA method from DiaSorin. Prolactin, Siemens Centaur HCG in post menopausal women (Core Lab) The Siemens Centaur Analyzer Endocrine Laboratory LLSG • Posterior Pituitary – Vasopressin (ADH) is measured by the Buhlmann RIA double-antibody method. Method involves an extraction and two 24 hour incubation stages. Test performed about every two weeks with a reference range of 0.8 to 3.5 pmol/L. – Oxytocin: not available and limited clinical utility Endocrine Laboratory LLSG • Thyroid Gland - Cortex – – – – – – – – Total T4 (obsolete) Free T4 (Centaur Analyzer) Total T3 (?) Free T3 (Centaur Analyzer) T3 uptake (obsolete) PBI (obsolete) Reverse T3 TBII, LATS Endocrine Laboratory LLSG • Thyroid Gland Cortical region – Thyroglobulin (IRMA isotope kit from Kronus) • Thyroid Gland medulla – Calcitonin (Immulite) • Thyroid Antibodies – Anti-thyroglobulin (Anti-TG Abs – Immulite) – Anti-thyroid peroxidase (Anti-TPO Abs - Immulite) • Parathyroid Glands – PTH (Immulite) Immulite 2000 analyzer Endocrine Laboratory LLSG • Adrenal Gland - Cortex Cortisol - plasma am Cortisol - plasma pm Urinary free cortisol – below 380 nmol/d Urinary cortisol – below 789 nmol/d • Urinary 17-OH corticosteroids by the Porter Silber method (phenylhydrazine) or 17-Ketogenic steroids by the Zimmerman reaction, now obsolete. Aldosterone, DHEAS (on Immulite 2000) • Urinary 17-Ketosteroids by the Zimmerman (M-dinitrobenzene) reaction, now obsolete. 17 Hydroxy progesterone (RIA) Endocrine Laboratory LLSG • Adrenal Gland - Medulla – Urine VMA total 24 hour or VMA per mmol/creat – Urine HVA total 24 hour or HVA per mmol/creat – Urinary and Plasma Catecholamines by HPLC – Dopamine – Norepinephrine – Epinephrine – Urine and Plasma Serotonin and Histamine by ELISA – Urine Metanephrine by HPLC – Plasma Metanephrine ???? (LC/MS/MS) Endocrine Laboratory LLSG • Stomach, Liver and GI – Gastrin by RIA – I125 label is on the gastrin molecule – Secretin not measured – Ghrelin methods available for research – stimulates GH secretion from the AP – Insulin Like Growth Factor 1 or IGF-1. Measured on the Immulite analyzer. – HIAA by HPLC for diagnosis of Carcinoid – Chromogranin A by ELISA Endocrine Laboratory LLSG • Pancreas - Glucose in the Core laboratory - Insulin by immunoassay on the Immulite analyzer - C-peptide on the Immulite analyzer to determine endogenous insulin secretion. - Glucogon – not available - Somatostatin (also from hypothalamus) – not available Endocrine Laboratory LLSG • Ovary and Placenta - HCG to Dx pregnancy and HCG for MSS Estradiol on the Siemens Centaur Progesterone on the Siemens Centaur Androstenedione on the Siemens Immulite - Inhibin A Inhibin B Total inhibins PAPP-A Estriol - Urinary 2/16 αEstrogen Metabolite Ratio ?? Endocrine Laboratory LLSG • Testes - Total Testosterone on the Siemens Centaur Free Testosterone by equilibrium Dialysis Free Testosterone by analog method Bioavailable Testosterone by calculation using Total testosterone and SHBG. - 5α-dihydrotestosterone (from testosterone) - ELISA Endocrine Laboratory LLSG • Kidney – Renin by RIA • Peripheral specimen may be supine or standing • Renal vein sampling – need to work with CIU and DI to get appropriate specimens – EPO on the Immulite (cannot differentiate normal from recombant forms) – 1, 25 dihydroxy Vitamin D from 25 hydroxy Vitamin D Endocrine Laboratory LLSG • SKIN – 25 hydroxy Vitamin D under the influence of sunlight. Laboratory assay has to be able to quantitate equally both D2 and D3 forms. Endocrine Laboratory LLSG