Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
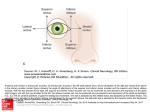
Identify the elements of the bony orbit on a skull or x-ray. Indicate the structures lying superior, inferior, medial and lateral to the eyeball and the position of the eyeball relative to the bony orbit. Horizontal CT Orbit lies: • Lateral to nasal cavity and paranasal sinuses •Medial to infratemporal fossa Coronal CT Orbit lies: • Inferior to cranial cavity •Above maxillary sinus Eyeball is oriented anteroposteriorly but orbits are angled outward Trace the flow of blood into and out of the orbit and orbital structures. Supratrochlear a. Supra-orbital a. Lacrimal gland Sup. Ophthalmic v. Inf. Ophthalmic v. Ant. ethmoidal a. Cavernous sinus Post. ethmoidal a. Lacrimal a. Facial v. Ophthalmic a. Internal carotid a. Retromandibular v. Pterygoid plexus Identify the extra-ocular muscles. Side view Levator palpebrae Superior oblique Optic nerve Superior rectus Lateral rectus (cut) Inferior oblique Inferior rectus Medial rectus SO LP LP SR LP SO MR IO SR SR SO LR MR IR IO LR LR MR IR IR Frontal views IO Indicate the nerve supply to each. Supratrochlear n. Supra-orbital n. Lacrimal n. Infratrochlear n. Ethmoidal nn. Lacrimal n. Frontal n. Short ciliary nn. V1 VI Long ciliary nn. Nasociliary n. V2 II Ciliary ganglion V3 V II III Frontal n. (cut) III IV VI V IV VI Sensory nerves are branches of the ophthalmic division of the trigeminal- V 1 Motor nerves are branches of cranial nerves III, IV, and VI Contrast the common clinical test for extra-ocular muscle function with the action of the individual muscles. SO LP Actions of individual extraocular muscles: •Lateral & medial rectus pull eyeball medial & laterally, respectively SR LR MR IR •Because of different axis of orbit & eyeball, superior & inferior rectus muscles pull the eyeball medially as well as elevate and depress it IO •Because of their oblique course, the superior & inferior oblique pull the eyeball laterally as well as down and up •Pure elevation is produced by the superior rectus & inferior oblique acting together •Pure depression is produced by IR & SO Contrast the common clinical test for extra-ocular muscle function with the action of the individual muscles. Clinical tests: •The best method to test eye motion is ask the patient to follow your finger drawing a large H pattern in the air a few feet from their face. The two legs of the H will isolate and test the motion of the superior/inferior rectus pair and inferior/superior oblique pair. The center part of the H will test the medial and lateral muscles. •Obliques are unique and involve adduction of globe prior to elevation and depression Predict the functional deficit resulting from damage to each nerve. This patient has a damaged right trochlear nerve (IV). The right superior oblique muscle is paralyzed. Note that movements to the right are not affected, but movements down and, especially, down and to the left result in asymmetrical eye movements. The right eye is not able to move down and in. There is a very cool web site that allows you to simulate the eye motions expected from lesions to different cranial nerves and different eye muscles. Check it out at http://cim.ucdavis.edu/Eyes/Version1/eyesim.htm Follow the course of autonomic nervous supply to the orbital structures, indicating the pre- and post-ganglionic sources of innervation. To Eyeball: •Preganglionic parasympathetic axons from EdingerWestphal nucleus travel in CN III to ciliary ganglion •After synapsing in ciliary ganglion, postganglionic axons travel to constrictor of the pupil and ciliary body via short ciliary nerves •Preganglionic sympathetic axons from T1-T2 enter sympathetic chain and ascend to the superior cervical ganglion (SCG) •After synapsing in the SCG, postganglionic axons join the plexus on the internal carotid artery and enter the orbit via its ophthalmic branch •In the orbit, these axons travel with the nasociliary nerve. Some pass through the ciliary ganglion and enter the eyeball via short ciliary nerves. Others enter via long ciliary nerves. These innervate the dilator of the pupil. •Other sympathetic postganglionic axons contribute to the innervation of the levator palpebrae muscle Follow the course of autonomic nervous supply to the orbital structures, indicating the pre- and post-ganglionic sources of innervation. Innervation of the lacrimal gland: •Arises from facial nerve •Takes pathway involving several nerves Greater petrosal n. N. of pterygoid canal formed from: •parasympathetic preganglionic axons in greater petrosal n. that will synapse in pterygopalatine ganglion •Sympathetic postganglionic axons from SCG cells that will pass through ganglion Facial n. Lacrimal n. (V1) Deep petrosal n. V2 N. of pterygoid canal Pterygopalatine ganglion Pterygopalatine ganglion