Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
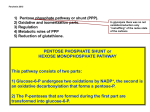
RBC ENZYMOPATHIES SHEJAL PATEL DO RBC ENZYMOPATHIES • Abnormalities of RBC enzymes cause Hereditary Nonspherocytic Hemolytic Anemia(HNSHA) • As RBCs mature they lose their nucleus, mitochondria and other organelles which causes them to not be able to carry out oxidative phosphorylation and protein synthesis. RBC ENZYMOPATHIES • RBCs must sustain active metabolism to transport and deliver oxygen to tissue and maintain flexibility and integrity of red cell membrane. • This is achieved by metabolic pathways: anaerobic glycolysis, hexose monophosphate shunt, glutathione metabolism, and nucleotide salvage pathway. How many RBC enzymopathy disorders are there? CASE 1 46 yo male comes in for evaluation of fatigue, lethargy, dyspnea, and yellowing of the eyes for one week. He recently was treated for MRSA skin infection on his forearm with a 14 day course of bactrim. He finished his last antibiotic today and his infection has resolved. On exam, VS stable except for heart rate of 112, scleral icterus. Labs: wbc 8.9, hgb 9.6, MCV 104, plts 259, retic 6.4%. What is his likely diagnosis and what other labs would you want? CASE 1 • Additional labs: T. Bili 6.2, D. Bili 1.2 , LDH 250, Haptoglobin <8, DAT negative. • You get a peripheral smear… DOES THIS HELP MAKE A DIAGNOSIS? G6PD DEFICIENCY • Most common enzymatic disorder in RBCs, affects 400 million people in the world. • It is X-linked. • Glucose-6-Phosphate dehydrogenase is an enzyme that protects red blood cells from oxidative damage. When there is oxidative damage to hemoglobin this leads to precipitation of hemoglobin which morphologically is Heinz bodies on peripheral smear. G6PD deficiency is worldwide, what are the more common places? Does it’s distribution correlate with another disease prevalence? G6PD DEFICIENCY • Highest prevalence rates in Tropical Africa, Middle East, Tropical and subtropical Asia, Mediterranean, and Papua New Guinea. • In the United States, black males are primarily affected. • Internationally, prevalence of G6PD deficiency correlates with distribution of malaria. G6PD deficiency patients may have protection against malaria. The possible mechanism of malarial protection may be increased phagocytosis of G6PD deficient erythrocytes containing the early ring stage parasites. How do you make the diagnosis for g6pd deficiency? Are false negatives possible? DIAGNOSIS OF G6PD DEFICIENCY • Enzymatic activity of G6PD • Timing of testing of enzyme level is very important to help prevent false negative results. During acute hemolysis and shortly after hemolysis, can have false negative results because young erythrocytes which predominate during this time will have higher enzymatic activity. Reticulocytes have 5 x higher G6PD enzyme activity than the oldest RBC. • Can also get molecular or genetic testing. Van den Broek et al. G6pD deficiency: not exclusively in males. Clinical Case Reports. 2016 p1-3 What triggers are there for acute hemolysis in G6PD deficiency patients and how do you treat? TRIGGERS FOR ACUTE HEMOLYSIS • Exposure to oxidants: • drugs (http: //www.g6pd.org/en/G6PDDeficiency/ SafeUnsafe/DaEvitare ISS-it) • infections • fava beans. G6PD DEFICIENCY TREATMENT • Avoid triggers, ie meds known to cause hemolysis or fava beans • Stop offending agent. Acute hemolysis is usually short lived about a week, likely because the older rbcs(with lower enzymatic activity) are already eliminated. • Supportive are via blood transfusion if symptomatic anemia. • Folic acid supplementation in those with chronic hemolysis. CASE 2 A nine year old caucasian female is referred to you for evaluation of anemia found on a routine physical examination. She is active and the fastest person on her soccer team. Your exam reveals mild icterus, a palpable spleen 2 cm below the left costal margin, and the following laboratory studies: hemoglobin 8.8 ; reticulocyte count 8% ; MCV 96. On peripheral blood smear you note polychromasia, with several echinocytes and an occasional spherocyte. There is no family history of blood dyscrasia. The most likely diagnosis is: A. Congenital spherocytosis from a spontaneous mutation B. 5’ nucleotidase deficiency C. B12 deficiency D. Hereditary elliptocytosis E. Pyruvate kinase deficiency PYRUVATE KINASE DEFICIENCY • The most common glycolytic defect that causes congenital non-spherocytic hemolytic anemia. • Pyruvate kinase converts phosphoenolpyruvate to pyruvate, making 50% of the red cell total ATP. Red cell lifespan is dependent on ATP produced. Therefore, PKD leads to less ATP and shortened red cell lifespan. • The younger rbcs are more vulnerable to destruction because they are more dependent on glycolysis and ATP. PYRUVATE KINASE DEFICIENCY • Severity of hemolytic anemia is variable in PKD patients. • Autosomal recessive • Distributed worldwide however more common in northern European and Chinese. In the US, common in Pennsylvania Amish. • Controversial whether it protects against malaria. How do you diagnose PK deficiency? How do you treat pkd patients? Any different treatment in newborns versus adults? PKD TREATMENT IN INFANTS • Severe hyperbilirubinemia is common. Newborns often require phototherapy and or exchange transfusions. There are rare cases of fulminant hepatic failure from PKD. • Chronic rbc transfusions may be necessary although can improve with age. PKD TREATMENT IN NON INFANTS • Supportive care via rbc transfusions. Folic acid for chronic hemolysis. • Splenectomy is an option for transfusion dependent patients and in those who do not tolerate anemia. Splenectomy can raise hgb by 1-3 gm. Postsplenectomy expect also rise in reticulocytes because reticulocytes are preferentially sequestered in the spleen • Some cases of PKD pts who had a BMT and were cured of PKD. CASE 3 12 yo male presented with mild jaundice and mild pallor. He has no history of blood transfusions or medications. On exam, normal growth and development except for hepatosplenomegaly. On labs, wbc 4, hgb 10, platelets 250, reticulocyte count 7%, serum bilirubin 4(mostly indirect bilirubin). What other labs do you want? CASE 3 • LDH elevated, haptoglobin low, DAT negative. • Osmotic fragility neg • Hb electrophoresis normal • G6PD enzyme level was normal • Serum and urine lead levels normal What is your differential with the peripheral blood smear? PYRIMIDINE 5’ NUCLEOTIDASE DEFICIENCY • The third most common enzymatic deficiency causing hemolysis. • Autosomal recessive • Pyrimidine 5’ nucleotidase participates in RNA degradation in reticulocytes. • In Pyrimidine 5’ nucleotidase deficiency there is accumulation of pyrimidines in red cells and causes toxicity and hemolysis. PYRIMIDINE 5’ NUCLEOTIDASE DEFICIENCY DIAGNOSIS • Seeing basophilic stippling can be suggestive but not diagnostic • For diagnosis need to show reduced P5’N-1 activity in red blood cells and high concentrations of pyrimidine nucleotides. PYRIMIDINE 5’ NUCLEOTIDASE DEFICIENCY TREATMENT • No specific treatment, supportive care • Rare cases of transfusion dependence • Transfusions may increase during times of infections or pregnancy • Splenectomy is controversial, in some has helped anemia and some not • Should monitor iron status and screen for hemochromatosis GOING BACK TO CASE 3 • What if the patient had a history of eating paint which had lead in it and his serum lead levels were elevated? • Would pyrimidine 5’ nucleotidase be low? LEAD POSIONING • Lead can induce pyrimidine 5’ nucleotidase deficiency. • Would expect hemolytic anemia and basophilic stippling on peripheral smear • This is very treatable with chelator and stopping lead exposure. CASE 4 78 yo man with history of diabetes admitted for aortic valve replacement, the week prior had a carotid endarterectomy. CMP, cbc and coags all within normal limits. When the carotid endarterectomy was performed patient got a cervical plexus block with lidocaine and ropivacaine. Patient noted to have low oxygenation and looked cyanotic so patient converted to general anesthesia. SpO2 remained low at 90%. ABG showed normal PaO2 and SaO2. Cyanosis had resolved and 8 hours after completion of surgery patient was extubated. Patient discharged 24 hours later, his last recorded SpO2 was 92% on RA. During aortic valve replacement patient noted to have cyanotic lips and SpO2 was 92% on RA. TEE didn’t show a right to left shunt. The patient’s SpO2 didn’t increase regardless of what was done to mechanical ventilator. Blood in the systemic flow line remained brown and dark in the cardiopulmonary bypass. CASE 4 ABG showed a pH 7.4, SaO2 99%, PaO2: 309, hgb 10.5, carboxyhemoglobin: 0.1%, metHb : 23.2%. No specific treatment was given(since no clinical cyanosis) and surgery was continued. Methb was 17% at end of surgery. Postoperative period several ABG measurements showed metHb around 20%. Patient denied taking any oxidizing substance that could cause methemoglobinemia. Hematology Oncology consults is called because of suspicion of congenital methemoglobinemia. What workup should be done? CASE 4 • Hemoglobin electrophoresis to identify hemoglobin M, some difficult cases may need to do DNA sequencing. Hgb M can cause congenital cyanosis. • DNA sequencing was done to look for mutations in the gene encoding for NADH cytochrome b5 reductase which showed a mutation. Patient was diagnosed with type 1 congenital methemoglobinemia . CYTOCHROME B5R DEFICIENCY • The most common cause of congenital methemoglobinemia. • Autosomal recessive • NADH cytochrome b5 reductase reduces methemolgobin back to hemoglobin. Normal metHb is maintained under 2%. • There are two types: • Type I-only red blood cells are affected • Type II- affects all cell types CYTOCHROME B5R DEFICIENCY • Type I• Endemic in some populations of Athabascan Indians, Navajo Indians, Yakutsk natives of Siberia • metHb levels are 10-35% generally and they appear cyanotic but are usually asymptomatic even with levels up to 40% • Life expectancy is normal • Some will have polycythemia • With oxidant stress, those affected can have acute symptomatic methemoglobinemia. CYTOCHROME B5R DEFICIENCY • Type II • Sxs: cyanosis, mental retardation, severe developmental delay • Life expectancy is shortened due to neurological complications How do most with cytochrome B5R deficiency not have any symptoms? CYTOCHROME B5R DEFICIENCY • Patients can tolerate up Methgb levels as high as 40% because of physiological adaptations… • Polycythemia • Changes in concentration of 2, 3- DPG and ph • Synthesis of globin chains • However can decompensate when exposed to oxidizing agents What are the clinical manifestations of methemoglobinema? CYTOCHROME B5R DEFICIENCY DIAGNOSIS • Measurement of activity of NADH cytochrome b5 reductase or investigations for known mutations by molecular biology. CYTOCHROME B5R DEFICIENCY TREATMENT • Avoid oxidant drugs • Can use methylene blue &/or ascorbic acid for cyanosis. In type II patients this treatment will not do anything for neurologic abnormalities. • Methylene blue is converted to leucomethylene blue, which results in a nonenzymatic reduction of methemoglobin. Ascorbic acid directly reduces methehemoglobin, but it works slowly. • Alternative therapy: hyperbaric oxygen and exchange transfusions BACK TO CASE 4 • Likely the lidocaine being an oxidant agent likely increased methemoglobinemia in this patient with congenital metHb enzyme deficiency. REFERENCES • Prchal et al. Red Cell Enzymes. Hematology 2005 p19-23. • Koralkova et al. Rare hereditary red blood cell enzymopathies associated with hemolytic anemia-pathophysiology, clinical aspects and laboratory diagnosis. Int Lab Hem. 2014, 36: 388-397. • Corrons. Red blood cell enzyme defect. Ch 17. 2009. • Uptodate.com • Grace et al. Erythrocyte pyruvate kinase deficiency: 2015 status report. AJH 90:825-830 REFERENCES • Zanella et al. Hereditary pyrimidine 5’ nucleotidase deficiency: from genetics to clinical manifestations. BJH, 2006: 133, 113123 • Aparna et al. Congenital Non-spherocytic hemolytic anemia (CNSHA) due to pyrimidine 5’ nucleotidase deficiency. Indian Pediatrics. 2006: vol 43:p184-185. • Rees et al. Pyrmidine 5’ Nucleotidase deficiency. BJH, 2003:120 p375-383. • Da-Silva et al. Congenital Methemoglobinemia: A rare cause of cyanosis in the newborn-a case report. Pediatrics 2003: vol 112: e158-e161 • Champigneulle et al. Late diagnosis of congenital methemoglobinemia in an Elderly patient during cardiac surgery. Journal of Cardiothoracic and Vascular Anesthesia, 2014: vol 28, no 3: p730-732. • NASCIMENTO, tatiana souza do; PEREIRA, rodrigo otávio lami; MELLO, humberto luiz dias de and COSTA, josé. Metemoglobinemia: do diagnóstico ao tratamento. Rev. Bras. Anestesiol. [Online]. 2008, vol.58, n.6, pp.651-664