Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
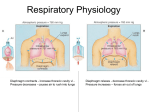
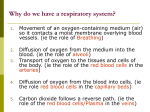
Respiratory Physiology Diaphragm contracts - increase thoracic cavity vl Pressure decreases - causes air to rush into lungs Diaphragm relaxes - decrease thoracic cavity vl Pressure increases – forces air out of lungs Inspiration Expiration Pulmonary volumes • Values determined by using a spirometer – Tidal volume – amount of air inhaled or exhaled with each breath under resting conditions – Inspiratory reserve volume – amount of air that can be inhaled during forced breathing in addition to resting tidal volume – Expiratory reserve volume – amount of air that can be exhaled during forced breathing in addition to tidal volume – Residual volume – Amount of air remaining in the lungs after a forced exhalation. Pulmonary volumes • Values determined by adding two or more of the respiratory volumes -Vital capacity – maximum amount of air that can be expired after taking the deepest breath possible (VC = TV + IRV + ERV) -Inspiratory capacity – maximum volume of air that can be inhaled following exhalation of resting tidal volume (IC = TV + IRV) -Functional residual capacity – volume of air remaining in the lungs following exhalation of resting volume (FRC = ERV + RV) -Total lung capacity – total volume of air that the lungs can hold (TLC = VC + RV) • Dead space – Anatomical dead space –areas of the conducting zone that contains air that never contributes to the gas exchange in the alveoli – Alveolar dead space – alveoli that or collapsed or obstructed and are not able to participate in gas exchange Spirogram Spirometer Partial Pressure of Atmosphere Barometer Pulmonary Gas Exchange Blood enters pulmonary capillary O2 diffuses into blood CO2 diffuses out of blood •Hemoglobin •Quaternary protein •Fe centered heme groups •O2 binds to heme group •CO2 binds to amine groups Carbon dioxide - transported from the body cells back to the lungs as: 1 - bicarbonate (HCO3) - 70% formed when CO2 (released by cells making ATP) combines with H2O (due to the enzyme in red blood cells called carbonic anhydrase) as shown in the diagram below 2 - carbaminohemoglobin - 20% formed when CO2 combines with hemoglobin (hemoglobin molecules that have given up their oxygen); contains plasma proteins 3 - dissolved in the plasma - 10% Systemic Gas Exchange Regulation of Breathing • Your respiratory rate changes. – Active - your respiratory rate goes up – Less active, or sleeping - the rate goes down. • Even though the respiratory muscles are voluntary, you can't consciously control them when you're sleeping. So, how is respiratory rate altered & how is respiration controlled when you're not consciously thinking about respiration? – The rhythmicity center of the medulla: • controls automatic breathing • consists of interacting neurons that fire either during inspiration (I neurons) or expiration (E neurons) – I neurons - stimulate neurons that innervate respiratory muscles (to bring about inspiration) – E neurons - inhibit I neurons (to 'shut down' the I neurons & bring about expiration) • Apneustic center (located in the pons) - stimulate I neurons to promote inspiration • Pneumotaxic center (located in the pons) - inhibits apneustic center & inhibits inspiration Patterns of Breathing • Apnea – temporary cessation of breathing (one or more skipped breaths) • Dyspnea – labored, gasping breathing; shortness of breath • Eupnea – Normal, relaxed, quiet breathing • Hyperpnea – increased rate and depth of breathing in response to exercise, pain, or other conditions • Hyperventilation – increased pulmonary ventilation in excess of metabolic demand • Hypoventilation – reduced pulmonary ventilation • Orthopnea – Dyspnea that occurs when a person is lying down • Respiratory arrest – permanent cessation of breathing Clinical Disorders and Diseases of the Respiratory System • Hypoxia – deficiency of oxygen in a tissue or the inability to use oxygen • Epitsaxis – nosebleed • Oxygen toxicity – excess oxygen, causing the build up of peroxides and free radicals • Chronic obstructive pulmonary diseases (COPD) – long-term obstruction of airflow and a substantial reduction in pulmonary ventilation • Chronic bronchitis – cilia are immobilized and reduced in number; goblet cells increase their production of mucus → mucus clogs the airways and breeds infection • Emphysema – alveolar walls break down and the surface area of the lungs is reduced • Asthma – allergens trigger the release of histamine and other inflammatory chemicals that cause intense bronchoconstriction. In asthma, periodic constriction of the bronchi and bronchioles makes it more difficult to breathe in and, especially, out. Attacks of asthma can be triggered by airborne irritants such as chemical fumes and cigarette smoke airborne particles to which the patient is allergic. • Lung cancer –most common cancer and most common cause of cancer deaths in U.S. males. There are several forms of lung cancer, but the most common (and most rapidly increasing) types are those involving the epithelial cells lining the bronchi and bronchioles. Ordinarily, the lining of these airways consists of two layers of cells. Chronic exposure to irritants causes the number of layers to increase. The ciliated and mucus-secreting cells disappear and are replaced by a disorganized mass of cells with abnormal nuclei. If the process continues, the growing mass penetrates the underlying basement membrane. Malignant cells can break away and be carried in lymph and blood to other parts of the body where they may lodge and continue to proliferate. It is this metastasis of the primary tumor that eventually kills the patient. Clinical Disorders and Diseases of the Respiratory System • Acute rhinitis – the common cold • Laryngitis – inflammation of the vocal folds • Pharyngitis – inflammation of the pharynx (sore throat) • Pneumonia – lower respiratory infection of the alveoli that causes fluid build up in the lungs. It can be caused by many kinds of both bacteria (Streptococcus pneumoniae) and viruses. Tissue fluids accumulate in the alveoli reducing the surface area exposed to air. If enough alveoli are affected, the patient may need supplemental oxygen. • Pleuritis - Inflammation of the pleura, producing more than the normal amount of fluid, causing a pleural effusion. The pain fibers of the lung are located in the pleura. When this tissue becomes inflamed, it results in a sharp pain in the chest that is worse with breathing in. Other symptoms of pleurisy can include cough, chest tenderness, and shortness of breath. • Sleep apnea – Cessation of breathing for 10 seconds or longer during sleep • Tuberculosis – pulmonary infection with Mycobacterium tuberculosis; reduces lung compliance • Cystic fibrosis - caused by inheriting two defective CFTR genes, a transmembrane protein needed for the transport of Cl− ions out of the epithelial cells of the lung thus enabling water to follow by osmosis. Diminished CFTR function reduces the water content of the fluid in the lungs making it more viscous and difficult for the ciliated cells to move it up out of the lungs. The accumulation of mucus plugs the airways interfering with breathing and causing a persistent cough. Cystic fibrosis is the most common inherited disease in the U.S. white population. Chronic Bronchitis Asthma Bronchi narrow due to swollen tissue and excessive mucus production Edema of mucusa, excessive mucosa production, muscle spasms obstruct airways Emphysema Alveolar walls torn and can’t repair,\alveoli fuse into large air spaces