Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Climate change adaptation wikipedia , lookup
Scientific opinion on climate change wikipedia , lookup
Surveys of scientists' views on climate change wikipedia , lookup
Politics of global warming wikipedia , lookup
Effects of global warming on human health wikipedia , lookup
Public opinion on global warming wikipedia , lookup
Climate change and poverty wikipedia , lookup
Years of Living Dangerously wikipedia , lookup
IPCC Fourth Assessment Report wikipedia , lookup
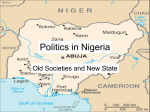
Africa Case Study Dele Ogunseitan School of Social Ecology University of California, Irvine May 20th 2004 Advanced Institute of Vulnerability to Global Environmental Change International Institute for Applied Systems Analysis, Austria Outline (1) Institutional Issues: Framing and prioritizing vulnerability assessments in Africa. (2) Thinking outside the dominant framework: Global environmental change and the African burden of disease. (3) Proposed solutions to global environmental change will have impacts too: No-cost adaptation and the clean development mechanism in Africa. (4) Break (5) Group discussion/summary Panarchy and Vulnerability “Panarchy focuses on ecological and social systems that change abruptly. It is the process by which ecosystems and societies grow, adapt, transform, and, in the end, collapse.” - C.S. “Buzz” Holling (2004) Vulnerability is inevitable? Epidemics Extinctions Forest fires Earthquakes War » Holling, C. S. 2004. From complex regions to complex worlds. Ecology and Society 9(1): 11. [online] URL: http://www.ecologyandsociety.org/vol9/iss1/art11 » Gunderson, L. H., and C. S. Holling. 2002. Panarchy: understanding transformations in human and natural systems. Island Press, Washington D.C., USA. Several external factors contribute simultaneously to vulnerability e.g. “abrupt” climate change; emerging pathogens; global trade; how do we prioritize assessments? Vt = ∑(Vi)*∑ (Ve) Internal vulnerability Perpetual Panarchy in Africa Normative Issues When resources are limited, choices are typically made to focus on pre-existing stressors rather than on emerging threats, but innovative frameworks address both challenges through “nocost” adaptation strategies. In many African countries, the reconciliation of national development plans with international priority to mitigate global environmental change (e.g. climate change, ozone depletion, biodiversity loss) remains an intractable policy controversy. Its resolution requires conviction of vulnerability to new conditions that will exacerbate preexisting environmental stresses on society and public welfare. Emergence of Regional Frames of Vulnerability The Perspective of Developing Countries: The New Delhi Conference in 1989 (The equity argument). African Perspectives: Nairobi Conference in 2-4 May 1990; Sponsored by the Woods Hole Research Center at the UNEP headquarters. The Cost of Gaining International Financial Support: Framing, funding, and the question of intellectual hegemony. Prioritizing GHG Inventories, Mitigation, and Vulnerability (Sensitivity + Capacity for Adaptation). The benefits of national GHG inventories and mitigation are shared globally. Whereas the burden of adaptation to the impacts are expected to be borne nationally. Policy Recommendations from the 1990 Gathering of “African Perspectives” Focus on deforestation, carbon sinks, and food security Futuristic scenarios Enhancing research and training Strengthening the technological base Promoting public awareness and participation Reforming the institutional environment Vigilance of industrialized country actions Promotion of private sector initiatives Adjusting UN agency framework e.g. CoP to UNFCCC; Ramsar e.g. Country Study Programs; IPCC e.g. Burden of disease estimates International Conventions; Country representatives Negotiation of Alternative International Frameworks At the same scale National Environmental And Health Policy Local knowledge systems Framing environmental issues across different scales International Support for Vulnerability Assessments in Africa _____________________________________________________________________________________________ ,,,, US CSP GEF Netherlands CSP German GTZ WHO Mauritius U.S.-sponsored Country Study Programs on climate change inventories, mitigation, and vulnerability assessments African Participation in the USCSP: Assessments of Vulnerability and Adaptation by Sector Country Botswana Cote d'Ivoire Egypt Ethiopia The Gambia Kenya Malawi Mauritius Mozambique a Nigeria South Africa Tanzania Uganda Zambia Zimbabwe Coastal Resource *# *# * * * * Agric. *# * * * * * * * * * * Grassland And Livestock Water Resource Forests Fishery * * * * * *# * * * * * * * * * * * * * * * * * * Wildlife Human Health * * * * * * * * * * * * * * * * *Vulnerability assessment #Adaptation assessment (Note: decoupled from vulnerability) Some assessments are jointly funded by the GEF * * * * * * Agenda setting: Institutional structure, state of the science, and advocacy Q: When USCSP started supporting national assessments in 1992-94, health was not included in the first round of vulnerability assessments -until much later in 1996-98 with the second round of assessments and national action plans. What caused the delay? A: “We were limited mainly by the development of the science. We did not have good information or training to provide, but after we got into the program, some countries began to agitate for the inclusion of health. At about the same time, some influential scientists were beginning to produce empirical work on health impacts of climate change, and as a result of the combination of the request from participating countries and the availability of scientific expertise, we decided to include health.” I would say that, except in the health area, which really did in fact come up from a number of different countries, nothing else came completely out of the blue, because we had a big net for the issues. - Jack Fitzgerald, Acting Director, USCSP (2000). Health as a focal point for assessments of vulnerability • Health is a common concern for African countries, and the ultimate impact of climate on crop production and water resources is population health. • Development of “Early warning systems” for local environmental changes that currently accounts for most impact on human health and social welfare. • Possibility of circumventing health-damaging pathways to industrial development. • *Pre-epidemiologic transition. Therefore, burden of disease is attributable to environmental factors that are sensitive to climate change. – *WMO-day 1999: Weather, Climate, and Health 1963 1973 25,000 km2 95% reduction Lake Chad 1,250 km2 1997 1987 The Lake Chad Basin Commission has mandate over 967,000 km2 watershed. Five member states own it and contribute it's budgets. The mandates of regional organizations enable them to undertake active multipurpose infrastructural projects that could generate funds to finance of regional basin organizations. Population migration, resource conflict, and vulnerability to AIDS in Lake Chad Basin Countries Estimates of the number of persons living with the HIV, June 2000* Adults and Children Cameroon Adults Rates among adults Women (1549) Children (0-14) 540,000 520,000 7.73% 290,000 22,000 64,000 61,000 1.35% 34,000 33,000 2,700,000 2,600,000 5.06% 1,400,000 120,000 C.A.R. 240,000 230,000 13.84% 130,000 8900 Chad 449,254 88,000 2.69% 49,000 4000 Total 3 993 250 3 499 000 6.13% (average rate) 1 903 000 187 900 Niger Nigeria *Source : UNAIDS High expectations for new cross-scale institutional arrangement The Ramsar Convention on Wetlands Memorandum of Cooperation between Ramsar and the Lake Chad Basin Commission (established in 1964) The signing ceremony, Valencia, Spain, 23 November 2002: Delmar Blasco and Muhammad Sani Adamu Naivasha Lake Basin Today at 1880 m above sea level (1886 m in 1926), it is the highest of the Rift Valley freshwater lakes, and second largest at 100 km2, but only 5 m deep; and no outlet! >400 species of birds 1980 Human population 20,000 Fish harvest 68 tonnes Ramsar Convention Designation in 1996 2000 Human population 250,000 Fish harvest 14 tonnes Sewage, pesticides, and Fertilizer loading. Optimization of institutional collaborations • Negotiation of constraints on agenda setting and funding mechanisms to re-establish ownership of assessments and responsibility for intervention schemes). • Technical capacity development, including qualitative and quantitative analyses. • Re-configuration of science-policy interfaces within countries. Published On-line http://www.globalforumhealth.org/forum_6/sessions/ Every year more than US $70 billion is spent on health research and development by the public and private sectors. An estimated 10% of this is used for research into 90% of the world's health problems. This is what is called "the 10/90 gap". Research Approach • It is generally assumed that potentially controllable environmental risk factors, as opposed to life style preferences, contribute most to the burden of disease in developing countries. • Quantitative assessments of the health impacts of environmental remediation are not commonly performed because of methodological difficulties and the paucity of data that could usefully correlate investment in infrastructures for environmental protection to prevent adverse health outcomes. – These limitations have incapacitated attempts to prioritize risk factors in the interface between the environment and human health sectors. Objectives • The main objective of this research was to use composite indicators of disease burden as tools for prioritizing solvable environmental problems that influence sub-regional burden of disease. • To test the sensitivity of the composite indicators to various scenarios of global environmental change as a way to monitor population vulnerability. Global Burden of Disease Assessment Seven Regions WHO/WB/HSPH Estimating local burden of diseases • A composite measure of the combined impact of death and disability in a population is used to estimate disease burden. The Disability-Adjusted Life Years (DALY) model: • DALYi[0,0] = YLLi + YLDi • Where DALYi[0,0] = Undiscounted, unweighted for disease i • YLLi = Years of Life Lost due to disease i • YLDi = Years of Life lived with Disability due to disease i Communicable diseases Non-communicable diseases Injury-related Future projections of disease burden ln M = C + b1lnY + b2lnHC + b3T Where: M = projected mortality level C = constant term Y = GDP per capita HC = Human capital (including population growth) T = Time Estimating risks attributable to environmental factors Attributable Risk is assessed according to the following equation, using published data on relative risks for each cause of death and disability related to the exposure, levels of exposure (prevalence), and burden of disease due to each cause of death and disability in the population: AB = ∑ AFj Bj = ∑Pj (RRj – 1) ÷ ∑Pj (RRj – 1) + 1 • Where – – – – – AB = Attributable Burden for a risk factor AFj = Fraction of Burden from cause j Bj = population level burden of cause j P = Prevalence of exposure RRj = Relative Risk of disease or injury for cause j in exposed versus unexposed group. – n = Maximum exposure level Combining future projections with attributable risk can give an estimate of avoidable disease burden WHO, 2002 Models and Scenarios • In the first scenario, decadal evaluation of selected climate-driven epidemics were evaluated against projected scenarios of climate change predicted by the Intergovernmental Panel on Climate Change. • In the second scenario, co-benefits of climate change mitigation were explored using the burden of disease approach and the abatement of lead (Pb) exposure as the dependent variable. Rank order of population at risk for vector-borne diseases Millions Nigeria’s Demographic Characteristics* Characteristics 1999 Estimate Total Population 113,828,587 Total Population Growth Rate 2.92 % Urban Population (Fraction of Total Population) 41 % Urban Population Growth Rate 14% Life Expectancy at Birth Total Population = 54.06 Years Female = 54.06 Years Male = 52.55 Years Disability-Adjusted Healthy Life Expectancy (World Health Organization, Year 2000) Total Population = 38.3 Years Female = 38.4 Years Male = 38.1 Years Birth Rate 41.84 Births / 1,000 Population Total Fertility Rate (Average Number of Children per Mother) 6.02 Children Born Per Woman Death Rate 12.98 Deaths / 1,000 Population Infant Mortality 69.46 Deaths / 1,000 Live Births Maternal Mortality 1.0 % Fraction of Population Below Poverty Line 34.1 % Gender Ratio At Birth = 1.03 Male(s) / Female Ages 15-64 Years = 1.04 Male(s) / Female Age 65 and Older = 1.01 Male(s) / Female Total Population = 1.02 Male(s) / Female *Source: United Nations Development Program 1999. Socioeconomic indicators and health care status in Nigeria Indicator Public health expenditure (Proportion of GDP) Value* < 1% Private health expenditures (Proportion of GDP) 1% Urban dwellers access to improved water 80% Rural dwellers access to improved water 39% Urban dwellers access to improved sanitation 82% Rural dwellers access to improved sanitation 48% Population per doctor 5,208 (1993)** Population per hospital bed 599 (1990) Real GDP per capita 920 (1997) *Values are for 1995 unless otherwise stated. Source: UNDP, 1999. Cases of Notifiable Diseases in Nigeria 1990-1999. National Database Source: Federal Epidemiology Division, Federal Ministry of Health, Abuja, Nigeria Disease 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999* Cholera 4101 62418 8687 4160 3173 3364 59136 13411 9254 26358 CSM1 7804 6992 6418 4209 6119 7376 108546 39973 10793 1946 Diphtheria 1768 2849 2351 2042 1363 1556 2768 3285 6071 3769 G/Worm2 9050 5479 6749 5356 3388 1848 14388 10426 13419 9603 Hepatitis 5495 8897 8291 6312 4283 3599 5436 2664 8158 3264 Leprosy 20557 13641 14875 14706 10422 8105 7687 8524 10177 3704 Malaria 1116992 909656 1219348 981943 1175004 1133926 1149435 1148542 2122663 732170 Measles 115682 44026 85965 54734 108372 49880 102166 73735 164069 132856 Pertussis 42929 18685 22147 23800 34792 13639 26745 33729 49550 22162 Tuberculosis 20122 19626 14802 11601 15202 10040 121025 11388 19368 9329 Onchocerciasis 2002 758 2879 82634 6401 7272 5111 3125 2948 1024 Yellow fever 6035 2561 149 152 1167 0 0 0 5 0 1Cerebrospinal meningitis worm *January - August only 2Guinea Deaths from Notifiable Diseases in Nigeria 1990-1999 National Database Source: Federal Epidemiology Division, Federal Ministry of Health, Abuja, Nigeria Disease 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999* Cholera 61 7869 663 266 471 140 4546 851 277 2085 CSM1 784 695 563 472 437 1388 11231 965 797 165 Diphtheria 2 64 3 0 0 5 55 166 3 15 G/Worm2 7 23 0 0 0 0 0 0 1 38 Hepatitis 69 60 48 53 33 54 38 39 42 20 Leprosy 7 17 35 0 0 1 0 0 0 0 Malaria 2284 1947 1068 719 1686 3268 4773 4603 6197 1891 Measles 1399 388 1032 373 696 671 2031 1147 1804 2751 Pertussis 184 66 1 61 65 51 186 222 216 121 Tuberculosis 213 487 230 192 379 407 380 331 454 152 Onchocerciasis 1 4 0 0 25 1 90 85 2 0 Yellow fever 421 661 8 8 415 0 0 0 3 0 1Cerebrospinal meningitis worm *January - August only 2Guinea Regional Mortality by Gender in Study Population (1990 - 1999). DEATHS PER 1,000 2.5 2 MALES 1.5 FEMALES 1 0.5 0 1 2 3 4 5 6 YEARS 7 8 9 10 ADMISSIONS PER 1,000 Hospital Admissions by Gender in the Study Population (1990 - 1999). 35 30 25 MALES 20 FEMALES 15 10 5 0 1 2 3 4 5 6 YEARS 7 8 9 10 10- Measles 11-Malaria 3-Severe diarrhea 0.90 18 2 37-ALRI (child) 0.1 38-ALRI (adult) 1.31 4-TB Disease Incidence per 1000 1.2 2-Typhoid 4 1-Cholera 0.19 6-Diptheria 0.03 7-Pertussis 0.03 19-Yaws 8-Meningitis 0.22 22-Hepatitis 9-Polio 0.007 23-Trypanosomiasis 6 0.3 0.05 13-Leprosy 0.12 Tetanus neonate 15-Schistosomiasis 0.14 24a-Tetanus post neo 0.75 20-Onchoceriasis 0.30 25-Cancer (child) 0.03 18-Guinea Worm 0.08 26-Cancer (adult) 0.69 30-Hookworm 19 27-Diabetes Ascaris 10 28 Malnutrition 36-Common cold-16 14-Chickenpox 1000 22 0.02 0.1 31-Rheumatic HD 0.3 3.8 0.12 32-Hypertensive HD 12-STD 0.24 34-Congenital HD 1.6 2 29 Sickle Cell Disease AIDS 21-Trachoma 0.5 0.07 33-Other HD 35-Cerebrovascular 39-Peptic ulcer 40-Other GI disease 41-Hernia/Int Obst 0.37 2.3 4.27 2.8 4 42-Cirrhosis 0.09 43-Chronic Renal D 0.31 44-Pregnancy Compli 1.13 Prematurity 9.6 Birth Injuries 1.6 Umbilical Sepsis 0.22 Congen Malform. 0.96 Hemolytic Dis 0.14 Birth Pneumonia 0.46 50GYN Disease 1 46-Skin Infections 47-Mental Disorders Cataracts/Eye 2.7 4.06 0.4 49-Dental Diseases 0.28 51-ENT Diseases 0.56 Accidents/All Epilepsy 7.7 0.48 DALY (HeaLY) model scenarios Discount Rate 0.015 - 0.045 Intervention Coverage EPI 0.3 WATER 0.2 – 0.4 SANITATION 0.45 OPD 0.45 IPD 0.4 EDUCATION 0.1 MFU 0.9 FAMILY PLANNING 0.05 A.N.C. 0.2 VECTOR CONTROL 0.2 – 0.5 The local burden of disease: Top categories for Years of Health Lives Lost (1990-1999) Rank Disease YHLL per 1000 1 Hypertension 88.5 2 Birth Injuries 47.3 3 Premature Birth 47.2 4 Mental Disease 41.9 5 Accidents 40.3 6 Malaria 33.3 7 Diabetes 33.0 8 Cerebrovascular disease 30.6 9 Tuberculosis 24.9 10 Neonatal Tetanus 18.9 11 Typhoid 16.7 12 Cancers (adult onset) 14.9 13 Congenital Malformations 13.9 14 Hernias 13.5 15 Tetanus (Post neonatal) 11.2 22 HIV / AIDS 4.93 Sensitivity of disease burden to environmental change Epidemic potential for climate-sensitive Vector-borne diseases EP = reciprocal of host density threshold Critical density for vector-borne disease transmission Mc1 = c1 (- ln (p) ÷ (b)(c)(a2)(pn)) Where p = survival probability of mosquito a = frequency of blood feeding n = incubation period of the parasite vector b = efficiency of infection c1 = constant based on recovery rate and host susceptibility factors Reproductive rate of disease = R0 = (m)(a2)(b)(c)(pn) ÷ r (-ln (p)) When R0 > 1, disease will spread. n = Dm ÷ T – Tmin, m Dm = degree-days required for parasite development T = average ambient temperature Tmin = minimum temperature required for parasite development MIASMA Modeling framework for the health Impact ASsessment of Man-induced Atmospheric changes • MIASMA is an acronym devised to refer to several models dealing with health impacts of global atmospheric changes: the vector-borne diseases model. From Shakespeare to Defoe: malaria in England in the Little Ice Age. Paul Reiter Centers for Disease Control and Prevention, USA. [email protected] • Present global temperatures are in a warming phase that began 200 to 300 years ago. Some climate models suggest that human activities may have exacerbated this phase by raising the atmospheric concentration of carbon dioxide and other greenhouse gases. Discussions of the potential effects of the weather include predictions that malaria will emerge from the tropics and become established in Europe and North America. The complex ecology and transmission dynamics of the disease, as well as accounts of its early history, refute such predictions. Emerging scientific controversy over the linkage between climate and vector-borne diseases (e.g. Malaria) Vol. 6, No. 4, Jul–Aug 2000 To the Editor: I read with great interest the article "From Shakespeare to Defoe: Malaria in England in the Little Ice Age" (1). Unfortunately, the article is not as balanced as a presentation last year by Paul Reiter, which clearly illustrated that, although climate is important in the transmission of malaria, the influence of other factors (e.g., access to medical care and improved housing) is likely to be of more importance in Europe…. While Reiter's paper offers an interesting perspective on the history of malaria in Europe, it provides no illuminating information on the influence of climate change on human health. - Pim Martens (Maastricht University, Maastricht, The Netherlands) To the Editor: The two reports from the International Panel on Climate Change (IPCC) (1,2) cited in the letter by Pim Martens (3) are widely regarded as "the standard scientific reference for all concerned with climate change and its consequences," yet the contents of these reports are often misleading…….. Repeated claims that global warming may have already led to increases in these diseases in the tropics are equally indefensible….. - Paul Reiter (Centers for Disease Control and Prevention, USA) Climate change and malaria vulnerability in Nigeria Environmental Change and the African Burden of Disease Projection of Disease Burden in Sub-Sahara Africa as a Function of Global Climate Change 1990 D A LY s Disease Malaria Diarrhea Dengue Tropical C. Malnutrition Respiratory Eyes HIV a 2000 D A LY s 2010 D A LY s 2020 D A LY s % of T o ta l A fric a n B u rd e n A fr ic a ’s Share of G lo b a l B urden W ith in C a te g o r y (% ) % of T o ta l A fric a n B u rd e n A fr ic a ’s Share of G lo b a l B urden W ith in C a te g o r y (% ) % of T o ta l A fric a n B u rd e n A fr ic a ’s Share of G lo b a l B urden W ith in C a te g o r y (% ) % of T o ta l A fric a n B u rd e n A fr ic a ’s Share of G lo b a l B urden W ith in C a te g o r y (% ) 9 85 32 3 52 18 13 19 75 8 9 < 0 .1 1 3 3 1 6 91 41 5 58 24 13 19 51 6 7 < 0 .1 1 2 4 1 6 93 46 6 64 28 14 19 42 4 5 < 0 .1 0 .5 2 5 1 4 94 49 6 73 30 15 20 33 11 < 0 .1 2 3 3 1 3 “Less popular” health vulnerabilities to climate change Dry Climate, Human susceptibility and the Meningitis Belt *1.2 Million Cases/year *135,000 Fatalities *8-12 year cycles in hyper-endemic regions *Shorter and more irregular intervals since 1980s The incidence Cerebrospinal Meningitis in Nigeria (1990 -1999). The vector-borne disease shows environment-dependent fluctuation dynamics in Nigeria. The upsurge in cerebrospinal meningitis is linked to recent climatic events. 120000 100000 80000 60000 40000 20000 0 1990 1991 1992 1993 1994 1995 YEAR 1996 1997 1998 1999 2000 Desertification and Health Impacts of Sahara Dust International focus on the trans-Atlantic movement of Sahara dust, with impacts Including the introduction of food crop pathogens in the Americas, and ironfertilization of the oceans, leading to coral reef bleaching. Impact on respiratory health effects In Sub-Saharan Africa is understudied. Current hypothesis include the exacerbation of respiratory diseases, Meningitis burden, and blindness. Policies to Mitigate Climate Change Will Have Global Impacts What are the projected health effects in African countries? Alternative Framing of Health Vulnerability in IPCC Assessments: Switching to alternative fuels will also lower vulnerability to Pb poisoning • Current framing of health impacts of climate change emphasizes the spread of vectorborne diseases which may have little additional impact in African countries. • 22% of gasoline used globally contains Pb, mostly in developing countries. • OPEC countries generally oppose shifting from carbon fuels, but they all still use leaded gasoline. • Joint Implementation arrangements must consider the direct health benefits of assistance towards decarbonization. Natural gas flaring in Nigeria contributes ~20-30% of global sources of greenhouse gas emissions from this source, contributing to the causes of global warming. Nigeria subscribes to OPEC-block position on mitigation strategies (Kyoto Protocol) SHELL'S GAS FLARE AT ITS KOLO CREEK SITE, BAYELSA STATE IN NIGERIA'S NIGER DELTA This picture is typical of gas flares that litter the Niger Delta. Many of them have been burning for over thirty years and blur any distinction between night and day in their range of impact. Photo Taken By Israel Aloja of Enviromental Rights Action/Friends of the Earth Nigeria [ERA/FoEN] In 1994, UN Commission on Sustainable Development Recommended Global Phase-out of Leaded Gasoline. In 2004, Many countries, largely in Africa and the Middle East, have no urgent plans to eliminate lead from gasoline Lukman’s Statement to COP-6 …………….As it stands, the Kyoto Protocol, if fully implemented, would lead to a dramatic loss of revenue for oil-exporting countries, as a result of a heavy reduction in demand for petroleum. Independent studies estimate the loss at tens of billions of US dollars per year for OPEC's Members. This would strike at the very heart of these countries' economic and social infrastructures, causing a radical scaling down of development plans and entailing huge cutbacks in such vital services as education and health care. It would also affect the ability of these countries to invest in future production capacity…………. ……Finally it should not be forgotten that the established industrial nations bear the principal responsibility for the purported phenomenon of global warming, and not the developing countries. The onus, therefore, is upon the rich nations to minimize and finance the negative impact of their response measures on the poor countries of the south. Developing countries should not be roped into making commitments to emissions-reduction targets, which could have enormous cost implications for their fragile economies. Instead, every assistance should be given to them to develop their economies in an efficient, environmentally harmonious and sustainable manner. - Rilwanu Lukman, OPEC Secretary General to Cop 6, September 2000. Comparative costing of health impacts of Pb and economic disincentives • In Nigeria, Pb content of regular gasoline is 0.74 g/L. • Atmospheric Pb emission is estimated to be 2,800 metric tons/year. • Policy analysts at the Center for Energy and Development in Ife calculate that the country cannot presently afford the cost of switching to non-leaded gasoline. • But what is the public health cost of not switching? How many DALYs can be attributed to the burden of Pb in Nigeria? The costs and benefits of energy de-carbonization • Nigeria has proven reserves of 180 billion cubic feet of natural gas - the 9th largest location of this resource in the world. • Nigeria flares 75 per cent of the gas it produces and reinjects only 12 per cent to enhance oil recovery. • Approximately 2 billion standard cubic feet of gas is currently being flared in Nigeria - the highest in any member-nation of the Organization of Petroleum Exporting Countries (OPEC). • Consequently, Nigeria accounts for 20-30% of the total amount of gas flared globally. Internalized Costs of Pb-Poisoning • Ibitoye et al. [1998] estimated a cost of $30 - $50 per ton for reduction of carbon dioxide emissions in Nigeria, according to the models and goals endorsed by the United Nations Framework Convention on Climate Change. • A maximum reduction of 2 billion tons of carbon could be achieved within the next 40 years. Thus, the total cost of decarbonization is estimated to be $60 – 100 billion for the next generation of Nigerians. • Meanwhile, the next generation is undergoing exposure to Pb. Assuming that most of the current sources of carbon dioxide are also sources of toxic metals and other air pollutants, more than 70 million young children in Nigeria are burdened by diseases attributable to leaded fossil fuels. At what cost? > 30% of children (ages 1-6 yrs) in rural Otukpo region of Nigeria are lead-poisoned Smith & Ogunseitan, 2002 Gender N Mean [B-Pb] Range SD % > 10 ug/dL Female 138 8.9 (2.1,23.8) 4.2 32.5 Male 168 9.8 (2.2,31.8) 4.8 35.0 Total 306 9.4 (2.1,31.8) 4.2 34.3 Lead (Pb) dose in urban Nigerian children between the ages of 1 and 7 years 30 25 20 % 15 10 5 0 5 7 9 11 13 15 17 19 21 Blood lead concentration (mg/dL) Nriagu et al., 1997 Quantifying the burden attributable to the health impacts of Pb-exposure in Nigeria • • • • • • • • • • • Mild mental retardation Ischaemic heart disease Cerebrovascular disease Genitourinary disease Immune suppression Spontaneous abortion Congenital anomalies Hypertension Iron deficiency anemia Endocrine disorders Hypertensive disorders of pregnancy – Collectively, these conditions represent approximately 15% of the total disease burden in the SSA region (Murray & Lopez, 1996). Calculating attributable risks for Pb-exposure The attributable risk (AR) due to lead exposure for 10 Pb-linked Global Burden of Disease (GBD) disease categories: • Genito-urinary disease • Spontaneous abortion • Premature birth • Dental caries • Lung cancers • Nervous system cancers • Congenital anomalies • Hypertension • Cerebrovascular disease • Low birth weight AR was assessed according to the following equation, using published data on relative risks for each cause of death and disability related to the exposure, levels of exposure (prevalence), and burden of disease due to each cause of death and disability in the population: AB = SAFjBj • Where – – – – – AB = Attributable Burden for a risk factor AFj = Fraction of Burden from cause j Bj = population level burden of cause j P = Prevalence of exposure RRj = Relative Risk of disease or injury for cause j in exposed versus unexposed group. Shift to mild mental retardation due to Pb-induced loss of IQ points Percentage of subjects Normal curve of distribution of intelligence Shift to mild mental retardation due to loss of IQ points Mild mental retardation 50 70 72.6 80 90 100 IQ 73.5 Fewtrell et al., [2002] • Risk of lead exposure on mental retardation: AR = PR – Pbaseline + PMR Standard ÷ PMR Standard Where MR PR = Mental retardation = Region-specific prevalence of MR from known causes Pbaseline = Prevalence of MR from known, noncongenital causes in developed countries; PMR Standard = Prevalence of MR according to the standard distribution of IQ score AR = Adjustment ratio. Contribution of Lead to the Burden of Disease in the Study Population Odds Ratio for PbB (ug/dL) DALYs, 0-14 Pb-Disease Category male female total 5-8 9-15 Attributable Risk % for PbB (ug/dL) >16 5-8 9-15 >16 Attributable BoD to Pb (%) 5-8 9-15 >16 710 541 1251 0.9 5 1.9 3.8 1.7 33.5 21.9 22 419 274 0 1000 1000 1.8 3.6 5.4 21.4 59.3 30.6 214 593 306 2295 2295 4590 2.2 4.3 8.6 29.0 64.9 43.2 1330 2978 1982 6.8 9.6 Dental Caries 129 127 256 (AR) (AR) 6.8 9.6 13.5 17 25 35 Lung Cancers 1 0 1 0.9 1.8 3.6 3.5 30.9 20.6 0 0 0 270 210 480 2 5.5 11 25.4 71.6 50.0 122 344 240 2455 2628 5083 0.8 1.6 3.2 7.3 25.1 18.0 371 1278 917 66 69 135 0.8 1.5 3 7.3 21.9 16.7 10 30 23 313 298 611 2.2 4.5 6.8 29.0 66.2 36.7 177 405 224 9827 8873 18700 1.2 2.4 4.7 6.4 43.9 27.0 1191 8218 5050 16066 16041 32107 3453 14289 9050 2731 2727 5458 587 2429 1538 % SSA Burden of Disease Attributable to Pb 1.08 4.49 2.84 % SSA Burden of Disease Attributable to Pb, Ages 0-14 1.77 7.34 4.65 % Nigeria Burden of Disease Attributable to Pb 1.08 4.49 2.84 % Nigeria Burden of Disease, Attributable to Pb, Ages 0-14 1.77 7.34 4.65 Genito-Urinary Disease Abortion Prematurity Nervous System Cancers congenital anomalies Hypertension Cerebrovascular Disease Low Birth Weight Total SSA Total Nigeria 13.5 (AR) Contribution of Pb Exposure to Disease Burden (Disability-Adjusted Life Years) • Symptoms above 10 mg/dL (Pb) – Growth retardation, Hearing loss, IQ deficiency, Colic, Nephropathy, Encephalopathy, Hypertension, Decreased longevity. • Burden of Disease Categories – Hypertensive disorders, Iron-deficiency anemia, Unipolar major depression, Nephritis and Nephrosis, Osteoarthritis, Congenital anomalies, Perinatal conditions, Endocrine disorders, and Poisonings. • Sub-Saharan Africa (2000 Baseline Scenario) Total DALYs = 318,560 • DALYs sensitive to metal toxicity as a risk factor = 44,050 (~4.7%) – Compared to diarrhea (10%), or malaria (7%), this is a considerable burden. Framing priorities • The cost of energy decarbonization is cost-effective (approximately $10,000 per child) if the expenses are directly linked to the reduction in disease burden. This estimated cost is higher than preventive costs calculated for the toll of malaria on the national economy [Sachs, 2000], but the benefits of decarbonization and eliminating lead pollution are also distributed internationally. Summary (1) Institutional Issues: Framing and prioritizing vulnerability assessments in Africa. Who is going to use the results of the vulnerability assessment that you are conducting? (2) Thinking outside the dominant framework: Global environmental change and the African burden of disease. Health (morbidity + mortality) is the ultimate outcome of vulnerability assessments. Cumulative vulnerabilities (e.g. agricultural productivity, coastal resources, water resources, etc. may be estimated with a common conversion factor to a health index. Is this worth doing in your assessment? (3) Proposed solutions to global environmental change will have impacts too: Nocost adaptation and the clean development mechanism in Africa. Think ahead – what are the vulnerabilities to proposed mitigation strategies in your region? (4) Break (5) Group discussion/summary