Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Ebola virus disease wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Gastroenteritis wikipedia , lookup
Sarcocystis wikipedia , lookup
Henipavirus wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Orthohantavirus wikipedia , lookup
Trichinosis wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Onchocerciasis wikipedia , lookup
Hepatitis C wikipedia , lookup
West Nile fever wikipedia , lookup
Rocky Mountain spotted fever wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Neonatal infection wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Leishmaniasis wikipedia , lookup
Visceral leishmaniasis wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Oesophagostomum wikipedia , lookup
Schistosomiasis wikipedia , lookup
Marburg virus disease wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Hepatitis B wikipedia , lookup
Leptospirosis wikipedia , lookup
Lymphocytic choriomeningitis wikipedia , lookup
Candidiasis wikipedia , lookup
Herpes simplex research wikipedia , lookup
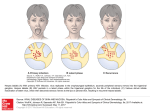
Oral Manifestations of Infectious Diseases in Children Reference: Pinkham, Chapter 4 Common Oral Conditions Acquired Developmental Congenital Acquired Oral Conditions Infections: Viral Bacterial Candida Autoimmune lesions Glossitis Discolored teeth INFECTIOUS DISEASES DIAGNOSTIC Obtain CRITERIA medical history Obtain dental history Conduct complete clinical examination Obtain necessary laboratory and radiographic studies. HERPETIC GINGIVOSTOMATITIS Causative Agent: Herpes Simplex Virus (HSV) Type I Clinical Evaluation: Viral infection S/S (malaise, fever..etc) Clinical: - Vesicle develop on the lips, tongue, gingival, palate - Vesicles rupture to form large painful ulcers - Gingiva: Edematous, bleeds easily HERPETIC GINGIVOSTOMATITIS Diagnosis: Age: Young patients History First exposure to HSV Viral culture, serum antibody Vesicle develop on the lips, tongue, gingival, palate HERPETIC GINGIVOSTOMATITIS Treatment: SELF-LIMITING (7-10 DAYS) Palliative mouthrinses. Orabase, or petroleum jelly, as a protective barrier Dehydration is a concern Patient is contagious Antibodies and steroids are contraindicated RECURRENT HERPES SIMPLEX (HERPES LABIALIS) Causative Agent: HSV – I (reactivation of the virus lying in the trigeminal ganglion). Clinical Presentation: - Hx of similar lesion - Small ulcers in the lip at: - mucocutaneous junction or - at the corner of the mouth, or - beneath the nose RECURRENT HERPES SIMPLEX (HERPES LABIALIS) Diagnosis: Subjective findings: - Itching before ulcer development. - Mild flu like symptoms. Objective findings: - Vesicles (2-4 mm), rupture and crust over 36-48 hrs. - Healing in 7-10 days. RECURRENT HERPES SIMPLEX (HERPES LABIALIS) Treatment: Self-limiting. Different Tx. modalities proposed: Lesion should be well lubricated Prophylactic or oral acyclovir: for suppression of herpes labialis: No evidence of effectiveness reduce the frequency – best success if lesion > 1/month. Healing without scar. HERPES ZOSTER (CHICKEN POX) Causative Agent: Varicilla-Zoster Virus (reactivation of the virus months or years after chicken pox can occur) Evaluation: Exposure to infected person More common in winter and spring time Most patients develop life-long immunity Children who are infected early in life or experience a particularly mild or sub-clinical case may become reinfected again. HERPES ZOSTER (CHICKEN POX) Diagnosis: Subjective: Fever, malaise, chills Objective: Vesicles starts on trunk, spread to extremities and face. Lesions crust and heal. Oral: Vesicles that rupture leaving small ulcers with red margins. These lesions are not very painful. HERPES ZOSTER (CHICKEN POX) Treatment: Self-limiting (7-10 days) - Contagious - Palliative treatment: - - Bed rest, antipyretics and analgesics. - Nails HERPENGINA Causative Agent: Coxsakie A Virus (types 2,3,4,5,6,8,10). Evaluation: Common in young children (< 4 yrs) Recent exposure to infected person (epidemic) More common during summer and fall. HERPENGINA Diagnosis: Subjective: Viral infection S/S (fever, malaise ..etc) Objective: Multiple vesicles on soft palate and tonsillar area. Vesicles ulcerate leaving gray area with erythematous base. Ulcers are painful. Lesions do not involve anterior 2/3 of the mouth. HERPENGINA Treatment: - Self-limiting: Acute symptoms persists for 3 days - Oral lesions heal in 7 to 10 days without scarring - Contagious ( isolation of the patient) - Palliative treatment: - Bed rest, antipyretics and analgesics Oral Fluid (dehydration) HAND, FOOT, AND MOUTH DISEASE Causative Agent Coxsakie A Virus (A-16) Tend to occur in epidemics Incubation period: Incidence: Symptoms: 2-6 days Children 1-10 years Low grade fever and malaise HAND, FOOT, AND MOUTH DISEASE Signs Maculopapular rash: 2-10 mm Appears on palms and soles and ventral surface of fingers and toes Become vesicular in 1-2 days Persists for 1-2 weeks Vesicles rupture and form painful aphthous like ulceration HAND, FOOT, AND MOUTH DISEASE Oral Manifestation: Multiple scattered superficial ulcers in the: tongue, buccal mucosa, less frequently in palate, gingiva, and lips HAND, FOOT, AND MOUTH DISEASE Healing: Oral lesions: Skin lesions: 5-10 days 1-2 weeks Treatment: Palliative treatment IMPETIGO Causative Agent: Two Types: Bullous caused by staphylococci Non-bullous caused by streptococci Evaluation: Gram stain good for bullous type only because non-bullous type can be secondarily infected by staphylococci. Throat and skin cultures for family members. IMPETIGO- Diagnosis Subjective: Hx of insect bites, exposure to infected person. Lesions are asymptomatic Objective: Non-Bullous: Thick, adherent-yellowish-brown crusted lesions (coalesce to form large lesion). Found in face and extremities. Bullous: Flaccid large bullae (anywhere), rupture in 2-3 days to form discrete round lesion (polycyclic area) IMPETIGO - Treatment Non-bullous: Minimal type: Moderate or excessive type: - Water soaks to remove crust - Topical antiseptic cleaner - Topical antibiotics 2-3/day - If no healing, systemic antibiotics. - Antibiotics: Penicillin G or erythromycine Bullous: Penicillinase-resistant penicillin (dicloxacillin) SCARLET FEVER Causative Agent: ß hemolytic streptococci Clinical Presentation: Incubation period: 3-5 days Symptoms: pharyngitis, headache, fever, nausea, vomiting, cervical lymphadenopathy Within 2-3 days: Skin rash develops as bright red papular skin rash SCARLET FEVER Oral Manifestation: Strawberry tongue (white coating with the papillae being erythematous and prominent) The coating is lost leaving an erythematous smooth surface. congestion of oral mucosa and palate A grayish-white exudates may cover the tonsils and facial pillars. Treatment: Penicillin for 10 days Mouthrinse (debridement of infected area) Paracetamol (Pain relief) CANDIDIASIS Causative Agent: Candida albicans Infection is established if normal oral normal flora is altered ( patient takes steroids, antibiotics for long time) Evaluation: It is important to identify the underlying cause CANDIDIASIS: Diagnosis: Subjective Sore throat Burning sensation Or Asymptomatic Objective Findings: Pseudomembranous form: Findings: Raised-white-curdy plaque Scaping leave a raw bleeding surface Erythrematous form: Red surface mostly on the tongue and palate Lesions may occur on any mucosal surface CANDIDIASIS Treatment: Mild: Topical antifungal agents (Nystatin) Moderate: Systemic antifungal agents (Ketoconazole) Severe: Systemic antifungal agents (Amphotericin B). INFECTIOUS DISEASES DIAGNOSTIC CRITERIA Obtain medical and dental history Conduct complete and thorough clinical examination Obtain necessary laboratory and radiographic studies. TYPES VIRAL BACTERIAL Fungal VIRAL INFECTIONS Primary herpes Recurrent herpes Herpes zoster (chicken pox) Cat Scratch Disease Herpangina Hand, foot, and mouth disease Rubeolla measels Rubella (German measles) Infectious mononucleosis PEDIATRIC HIV INFECTION Causative Agent Clinical Presentation PEDIATRIC HIV INFECTION Diagnosis: Treatment: