Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
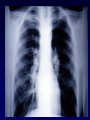
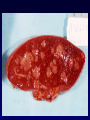
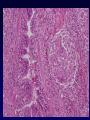
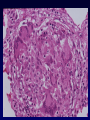
Pathogenesis of Granulomatous & Interstitial Airways Disease Granulomatous Disease Necrotizing vs Non-necrotizing • Most necrotizing granulomatous disease is infectious (TB!) • Responsible organism usually demonstrable in tissue • All specimens should be cultured • Non-infectious granulomatous inflammation – sarcoidosis, Wegener’s granulomatosis, Crohn’s, etc. Tuberculosis The mycobacteria that cause TB in man: • Mycobacterium tuberculosis – Lung is most common primary site – Droplet infection = inhalation of infective droplets coughed or sneezed by a patient with TB • Mycobacterium bovis – Drinking milk from infected cows – intestinal & tonsillar lesions • M. avium & M. intracellulare (MAC complex) – Opportunistic infection in IC • Mycobacteria: – Aerobic organisms – Difficult to stain • • • • waxy cell wall scanty in tissue slow growth in culture PCR – Difficult to kill (dormancy) • No toxins or histolytic enzymes • Inhibition of phagosome-lysosome fusion & killing by macrophages • Induce delayed hypersensitivity (type IV - T cell mediated) – Destructive effects Epidemiology • Developed countries: – Considerable fall in incidence and mortality in 20th century • A disease of the elderly: – Reactivation of quiescent infection acquired in youth • Recent resurgence: – AIDS, urban deprivation, immigrant & refugee populations • 1/3 world population infected (~1.7 billion) • 8 million new cases every year – 95% in developing countries • 3 million deaths every year – Largest cause of a death from a single pathogen • TB kills twice as many adults as AIDS, malaria and other parasitic diseases combined TB & HIV • Marked resurgence – Poorer communities, drug abuse • Multidrug resistant strains have emerged • 6 million people world-wide have dual infection, majority in sub-Saharan Africa • HIV infection – particularly aggressive TB – widespread, disseminated & poor host response • HIV infection promotes infection with opportunistic mycobacteria • Primary TB: – First time infection – Formerly found mainly in children, now encountered in adults • Secondary/Postprimary TB: – Adult type – Reactivation of a dormant primary lesion – Re-infection from re-inhalation Primary Tuberculosis • Transmitted through inhalation of infected droplets • Single tuberculous granuloma (tubercle): – within parenchyma (usually subpleural/periphery) = Ghon focus – also in hilar lymph nodes (common) = Ghon complex Ghon Complex - Sequence of Events • Inhaled bacilli ingested by alveolar macrophages • Macrophages with bacilli aggregate, forming microscopic nodules that deform architecture • Development of T-cell mediated immunity: CD4 (helper) & CD8 (cytotoxic) – CD4 – interferon – secretory changes in macrophages – epithelioid (activated) histiocytes – CD8 – kill macrophages – resulting in caseous necrosis • Fusion of macrophages to form Langerhan’s type giant cells • Mantle of B lymphocytes Primary TB Resolution vs. Progression • RESOLUTION: – Most common (if immunocompetent) – Development of a fibrous capsule - eventually calcified scar – Indefintely viable dormant bacteria • PROGRESSION: 1. Tuberculous bronchopneumonia – Erosion into bronchus - dissemination within bronchial tree (‘galloping consumption’) – Continuing casseation - cavitary fibrocasseous lesions Fibrocaseous 2. Pleural spread – effusion, TB empyema 3. Miliary TB (haematogenous dissemination) – – – – – Remainder of lung Cervical lymph nodes (scrofula) Meninges (tuberculous meningitis) Kidneys & adrenals Bones (tuberculous osteomyelitis) • veterbral TB = Pott’s disease – Fallopian tubes & epididymis Miliary Secondary TB 1. Reactivation of dormant lesion 2. Re-infection Associations - alcoholism, diabetes, silicosis & immunosuppression • Pulmonary – – Resolution or progression N.B. Extensive firosis in healing process: • • Pulmonary & pleural fibrosis Bronchiectasis TB in the elderly & immunocompromised • TB in the elderly: – • Disseminated miliary TB – (non-reactive TB) little granulomatous response, necrosis, DAD TB in AIDS: – – – Conventional morphology Granulomas poorly formed Opportunistic MAC from environment Necrotizing Granulomas - Other Infectious Causes • Bacteria: – Brucellosis • Fungi: – Histoplasma, Coccidioides, Cryptococcus & Blastomyces • Parasitic roundworm: – Dirofilaria Sarcoidosis • Systemic disease of unkown aetiology • Characterized by non-caseating granulomas in many tissues & organs – Lungs, lymph nodes, spleen, liver, bone marrow, skin, eye, salivary glands and less frequently – heart, kidneys, CNS, endocrine glands – pituitary Sarcoidosis • Occurs worldwide but geographical variation – more prevalent at higher latitudes – Ireland, Scandinavia & North America (African Americans) – 10 per 105 in UK • Females > Males, peak incidence 30 - 40 yrs • Exact aetiology & pathogenesis unclear • Several immunologic abnormlaities – Enhanced cellular hypersensitivity at involved sites – but depressed elsewhere • Anergy to common skin test antigens – Generally driven by CD4 T cells – Increased CD4 lymphocytes in the lung • Clinical: – Variable depending on organ(s) – Mild non-specific chest complaints, cough, dyspnoea – 1/3 – Erythema nodosum • Radiology: – Bilateral hilar lymphadenopathy Sarcodosis in the Lung • Non-caseating granulomas (classic) – Tight clusters of epithelioid histiocytes and occassional MNGCs – Tight rim of concentric fibroblasts , few lymphocytes (‘naked granulomas’) – Schaumann bodies • Laminated concretions (Ca2+ & protein) – Asteroid bodies • Stellate inclusions • Histological diagnosis of exclusion – DDx – infection, berylliosis, HP, IVDA, adjacent to tumour / lymphoma Sarcoidosis - Prognosis • Unpredictable clinical course – Progessive chronicity or alternating activity & remission • ~ 70% recover with steroid Rx • ~ 35% progress to interisital fibrosis & cor pulmonale Interstitial Lung Disease • Heterogeneous group of non-infectious, nonneoplastic disorders – Predominanly diffuse and usually chronic – Damage to the lung parenchyma (varying intersitial inflammation & fibrosis) • a.k.a alveolitis & pulmonary fibrosis • Restrictive lung disorders • Acute (e.g. DAD) vs. Chronic • NB - Clinical, Radiology & Pathology correlation! • Aetiology / associations: – idiopathic, collagen vascular disease, drugs & toxins, environmental Chronic ILD • FIBROSING: – – – – – – – – USUAL INTERSTITIAL PNEUMONIA (UIP/CFA/IPF) Non-specific interstitial pneumonia (NSIP) Cryptogenic organizing pneumonia (COP) Connective tissue disease Pneumoconiosis Drug rections Raditation pneumonitis Lymphocytic interstitial pneumonitis (LIP) • GRANULOMATOUS – Sarcoidosis – Hypersensitivity pneumonitis • SMOKING-RELATED: – Respiratory bronchiolitis (RB) – Desquamative* interstitial pneumonitis (DIP) Usual Interstitial Pneumonia • Progressive fibrosing disorder of unknown cause – ? Repeated acute lung injury (unknown agent) • Patchy lung involvement – worst at bases, subpleural & paraseptal distribution – Dense fibrosis – remodelling of lung architecture (‘honeycombing’) – Fibroblastic foci Usual Interstitial Pneumonia • Adults 30 to 60 yrs – Gradual onset of symptoms: dyspnea, non-prod cough • Median survival ~ 3 years – Respiratory and heart failure (cor pulmonale) – Require transplantation Pneumoconioses • Disorders caused by inhalation of inorganic elements, primarily mineral dusts. • Injury is determined by: – Length of exposure – Physicochemical characteristics – Host factors • Carbon dust - Coal worker’s pneumoconiosis: – Anthracosis – Simple coal worker’s pneumoconiosis – Progressive massive fibrosis • Silicosis – Silicotic nodules – TB risk • Asbestos – Asbestosis (pulmonary fibrosis) – Pleural disease (fibrous plaques, mesothelioma). Hypersensitivity Pneumonitis • Immune-mediated granulomatous inflammation caused by inhaling organic dusts – Mix type III (immune-complex deposition) & type IV (cellular mediated) hypersensitivity Farmer’s lung Thermophilic actinomycetes in hay Pigeon breeder’s Air-condition lung • Diffuse interstitial fibrosis (> upper lobes) – Progressive - honeycomb & respiratory failure Thermophilic bacteria