Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
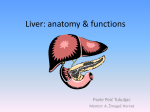
Gallstone disease. Cholecystitis, diagnosis and treatment Topicality • According to the 6th World Congress of Gastroenterology in the world is about 10% of the population suffer from gallstone (more common in developed countries, often in women, usually elderly) • Only in the U.S. per year performed more than 1 million cholecystectomy in Russia more than 200 thousand in Uzbekistan more than 5 thousand • The cost of treatment of cholelithiasis in France over 800 million euros a year. Historical information • Galen (Cl. Galenus) showed stones at autopsy. In 1341 Gentile da Foligno in Padua in embalming the corpse of a noble woman found in the neck of the gall bladder large green stone. In the second half of XV century, the famous Florentine physician Antonio Benevieni at autopsy woman who suffered long bouts of biliary colic, found in the gall bladder stone black size of a walnut. • Abu Ali ibn Sina - GSD called "disease-rich." • V. Coiter in 1573 French physician J. Fernel (1574) described the clinical presentation of gallstone disease and established its connection with jaundice. Chemical study of gallstones was first undertaken by S. Galeati (1746). • J. Thudichum, suggested that the rudiments of rock formed by the condensation cacocholia still in the intrahepatic bile ducts. Syntopy of the gallbladder 1 - Gall Bladder 2 – duodenum 3 - The right proportion of liver Gall bladder and biliary tract 1 - bottom of the gallbladder, 2 - body 3 - neck, 2 - area of union with the liver, 5 - right - and 6 left hepatic ducts, 7 - cystic duct 8 - common duct 9 - sphincter of Oddi, 10 - Vater papilla 11 - Flow-term pancreas cancer (Virsung). Topography structures enclosed in hepatoduodenal ligament. 1 — ductus hepaticus communis; 2 — ramus sinister a. hep. propriae 3 — ramus dexter a. hep. propriae; 4 — a. hepatica propria; 5 — a. gastrica dextra; 6 — a. hepatica communis; 7 — ventriculus; 8 — duodenum; 9 — a. gastroduodenalis; 10 — v. portae; 11 — ductus choledochus; 12 — ductus cysticus; 13 — vesica fellea. Physiology of the gallbladder • 1. During the day, the liver produces about a liter of bile. • 2. Sphincter of Oddi is reduced (7), the output of bile into the duodenum 12 (8) is terminated. • 3. Bile is continuously fed into the bile duct (3) • 4. Next comes the gallbladder (1) through the cystic duct (2) • 5. The wall of the bladder is very actively sucks the water from the bile Physiology of the gallbladder • When food enters from stomach to 12 duodenum, it begins to develop a hormone - cholecystokinin. • This hormone is a powerful stimulant to reduce gall bladder, and at the same time, this hormone relaxes the sphincter of Oddi. • The wall of the bladder is reduced simultaneously with the relaxation of the sphincter of Oddi and the concentrated bile from the gall bladder comes in 12 duodenal ulcer •The composition of bile •Bile - a yellow liquid. The basis of bile is water, which are major components of bile. • The composition of bile • Water • Bile acids (U-ny instvenny functional component of bile) • Lecithin (phospholipid) • Cholesterol (fat) • Bilirubin (the pigment that gives bile yellow) • Proteins (proteins) • Electrolytes (potassium ions, sodium, calcium, chlorine) Causes of Gallstones •Infectious inflammation of the biliary tract. •Metabolic disorders (increased cholesterol in the bile). •Stagnation of bile in the biliary ducts. Taurohol acid Cholesterol Bile acids Cholesterol gallstones Black pigment stones of the gallbladder Brown pigment gallbladder stone stages of gallstone disease • The first stage - the physical and chemical. (Nye litogen-bile). Clinical manifestations are absent. • The second stage - the latent asymptomatic carriers of the stone. The process of stone formation + + bile stasis inflammation. Clinical manifestations are absent, and the stones are discovered by accident. • The third stage - marked clinical manifestations. Acute inflammation in the gallbladder, choledocholithiasis, stenosis of the major duodenal papilla, acute cholangitis, acute pancreatitis Subjective manifestations of gallstone disease • • • • • • • Pain in right hypochondrium Nausea Bitterness in the mouth Heartburn Vomiting Relationship of pain with food intake Abdominal distention Localization of pain in Gallstone disease 5 «F» symptoms • • • • • FEMALE - female, female FORTY - forty FAT - thick, full FERTILE - fertile (multiparous) FAIR - blond, light (blonde) Methods of diagnosis of gallstone disease • • • • • • Duodenal intubation Ultrasonography Radiography (cholecysto-,holangiography) KT Laparoscopy Magnetic resonance imaging The normal ultrasound pattern of gallbladder 1. cavity of the gallbladder 2. wall of the gallbladder 3. cystic duct 4. liver tissue Gallstones Cholecystography 1. shadow of the gallbladder 2. Shadow of common bile duct 3. spine 4. ribs Cholecystography in the presence of two large stones in the gallbladder 1. gallbladder 2. stones 3. edge Disadvantages of the study - Harm to the body. - The need for training. - The contrast is not always accumulate in the biliary tract Vaeth, - Non-operation in the gallbladder, the contrast he does not fall Computed tomography retrograde pancreticocholangiography Antegrade cholangiography Percutaneous transhepaticcholecysto-, holangiography. diagnostic laparoscopy Complications of gallstone disease • • • • • • • • Acute cholecystitis Choledocholithiasis Obstructive jaundice Acute pancreatitis Cholangitis Bile peritonitis Hepatic failure Abscesses Surgeries for GSD • • • • • • Laparoscopic cholecystectomy Open cholecystectomy Holedoholitotomy Papillosfinkterotomy Cholecystitis and holangiostomy Holedohoduodenostomy Laparoscopic cholecystectomy Puncture of the gall bladder The intersection of the cystic duct Select items Isolation of arterial Clipping Cholecystectomy Open cholecystectomy Open cholecystectomy Cholecystectomy "from the neck" and "the bottom" Choledochoduodenostomy Yurash Flerken Finstrer Transduodenal papillosfincterotomy and plasty Transduodenal papillosfincterotomy and plasty Responsibility of PhGP: 1. To have knowledge of method diagnostics pathology of a bile duct and gallbladder. 2. Concepts classification of chelicistit’s. 3. Diagnostics of GSD and chronically calcules cholecistit’s. 4. Feature of differential diagnostics. 5. To send the patient to the surgical stationary. 6. Shepherd rehabilitation after surgical treatment.