Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Plasmodium falciparum wikipedia , lookup
Onchocerciasis wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Schistosoma mansoni wikipedia , lookup
Chagas disease wikipedia , lookup
Portable water purification wikipedia , lookup
Microbicides for sexually transmitted diseases wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
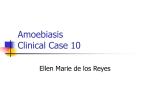
Visceral leishmaniasis wikipedia , lookup
Leptospirosis wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Hepatitis B wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Echinococcosis wikipedia , lookup
Trichinosis wikipedia , lookup
Hepatitis C wikipedia , lookup
Sarcocystis wikipedia , lookup
Gastroenteritis wikipedia , lookup
Schistosomiasis wikipedia , lookup
Cysticercosis wikipedia , lookup
Fasciolosis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Parasitology Faculty: AGUAZIM SAMUEL M.D. Lange chapter 51 1 Intestinal and Urogenital Protozoa 2 Parasites occur in two distinct forms: • Single-cell called protozoa • Multicellular metazoa called helminths or worms. 3 Protozoa can be subdivided into four groups: • • • • Sarcodina (amebas), Sporozoa (sporozoans), Mastigophora (flagellates), Ciliata (ciliates) 4 Metazoa are subdivided into two phyla: •Platyhelminthes (flatworms) •Nemathelminthes(roundworms, nematodes). •Platyhelminthes contains two medically important classes: •Cestoda (tapeworms) (swimming in a cespool of tapeworms) •Trematoda (flukes). (It is a fluke that you won a million dollars and you are trembling with 5 excitement) Intestinal Protozoa • Within the intestinal tract, three organisms: - The ameba (Entamoeba histolytica) - The flagellate (Giardia lamblia) - The sporozoan (Cryptosporidium parvum) 6 Urogenital Protozoa • In the urogenital tract, one organism: - The flagellate (Trichomonas vaginalis). 7 8 CASE • 33 year old man, presenting with right upper quadrant pain and fever of 4 days duration; slight yellowing of skin. • 1 week before, he had bloody stools, about 3 or 4 times per day, but it resolved 9 Case: 5 cm hypoechoic liver mass 10 CASE • Metronidazole • Significant improvement after 7 days • Repeat UTZ: smaller mass 11 CASE • Impression: Amebic liver abscess, secondary to Entamoeba histolytica 12 Intestinal Protozoa Entamoeba histolytica • Diseases:Amebic dysentery and liver abscess. 13 Entamoeba histolytica Characteristics: Intestinal protozoan. The life cycle consists of two stages: (1) Motile ameba (trophozoite) consists of one ingested red blood cell and one nucleus (2) Non-motile cysts with four nuclei with no internal fiber. 14 Trophozoite: one ingested red blood cell and one nucleus 15 Cysts: four nuclei with no internal fiber 16 Entamoeba histolytica trophozoites in section of intestine (H&E) 17 Entamoeba histolytica cyst and trophozoite, haematoxylin stained 18 Entamoeba histolytica • Life cycle: Humans ingest cysts, which form excystation in small intestine, which form trophozoites. Trophozoites pass to the colon and multiply. Cyst form in the colon. • Transmission and Epidemiology: Fecal-oral transmission of cysts via water, fresh fruit and vegetables. Human reservoir. Occurs worldwide, especially in tropics. • Also: ano-genital or oro-anal sexual contact • Pathogenesis: Trophozoites invade colon epithelium and produce “teardrop” ulcer. Can spread to liver and lungs and cause abscess. Excystation: the action of an encysted organism in escaping from its19 envelope Life cycle of Entamoeba histolytica 20 Histopathology of a typical flask-shaped ulcer of intestinal amebiasis. CDC 21 Amebic dysentery Acute amebiasis frequent dysenteric stools of pus and blood ; without feces systemic toxicity: fever, dehydration, electrolyte abnormalities Tenesmus , abdominal tenderness Chronic amebiasis recurrent episodes of dysentery intervening GIT disturbances, constipation Invasive disease: liver, lung and brain 22 23 24 AMEBOMA • proliferative granulomatous response at an ulcer site • infectious pseudotumor 25 Ameboma leading point of an intussusception or may cause intestinal obstruction 26 Amebic liver abscess • Most common extraintestinal form • metastasis from intestinal infection • Symptomatic intestinal infection need not be present • right upper quadrant pain • right shoulder pain • presses on the common bile duct : jaundice • Lung atelectasis, consolidation, pleural effusion 27 28 Gross pathology of liver containing amebic abscessGross. CDC 29 RUPTURED AMEBIC LIVER ABSCESS WITH “ANCHOVY PASTE” Gross pathology of amebic abscess of liver. Tube of "chocolate" pus from abscess. CDC 30 Amebiasis cutis 31 Brain abscess 32 Entamoeba histolytica Laboratory Diagnosis: 1. Trophozoites or cysts visible in stool. 2. Serologic testing (indirect hemagglutination test positive with invasive disease). Treatment: - Metronidazole plus iodoquinol. GET BAC on the Metro (Giardia, Entamoeba, Trichomonas, Bacterial vaginitis, amoebic infection, C. difficile) Prevention: 1- Proper disposal of human waste. 2- Water purification. 3- Hand washing. 33 Giardia lamblia Most prevalence enteric parasite in the us Leading in infectious agent in water borne outbreaking diarrhea Disease: Giardiasis, especially diarrhea -Characteristics: Intestinal protozoan. The life cycle consists of two stages: (1) Trophozoite, Pear-shaped with two nuclei and four pairs of flagella. (2) The oval cyst with four nuclei and several internal fibers34. 35 Trophozoite: Pear-shaped with two nuclei and four pairs of flagella Oval cyst: four nuclei and several internal fibers. 36 Giardiasis Early symptoms: flatulence abdominal distension nausea foul-smelling bulky, often watery, diarrhea explosive!!! chronic stage vitamin B12 malabsorption disaccharidase deficiency lactose intolerance 37 Diagnosis Definitve tests: Cysts in the stool Trophozoites in the duodenum (Enterotest®)- string test Endoscopy Treatment Metronidazole 4-6 hours Bile-stained 38 39 Giardia lamblia • Life cycle: Humans ingest cysts – form trophozoites in duodenum which encyst and are passed in feces. • Transmission and Epidemiology: Fecal-oral transmission of cysts. Human and animal reservoir. Occurs worldwide. • Pathogenesis: Trophozoites attach to wall with no invasion. They interfere with absorption of fat and protein. • Laboratory Diagnosis: Trophozoites or cysts visible in stool. String test used if necessary. • Treatment: Quinacrine, with Metronidazole as an acceptable alternative.. • Prevention: Water purification. Handwashing. 40 41 42 Cryptosporidium parvum • Disease: Cryptosporidiosis, especially diarrhea. • Characteristics: Intestinal protozoan. • Life cycle: Oocysts release sporozoites; they form trophozoites. After schizonts and merozoites form, microgametes and macrogametes are produced; they unite to form a zygote and then an oocyst. 43 44 45 Cryptosporidium parvum • Transmission and Epidemiology: Fecal-oral transmission of cysts from undercook meat and contaminated water. Human and animal reservoir. Occurs worldwide. • Pathogenesis: Trophozoites attach to wall of small intestine but do not invade. • Laboratory Diagnosis: (round) Oocysts visible in stool with acid-fast stain.*** • Treatment and Prevention : None. 46 47 CASE • 23 year old female, with pain during sexual contact, copious, malodorous vaginal discharge of 3 days duration. • Mild hypogastric pain, no vaginal bleeding • Regular periods • Multiple sexual partners, uses OCP 48 Case: Strawberry cervix, frothy discharge, 49 Case: vaginal smear 50 Case: vaginal smear • Impression: Trichomoniasis, secondary to Trichomonas vaginalis 51 Urogenital Protozoa Trichomonas vaginalis • Disease: Trichomoniasis. • Characteristics: Urogenital protozoan. Pear-shaped,with a central nucleus and four anterior flagella. It exists only as a trophozoites. No cysts or other forms. Mot : trophozoites, sexual, formites • Laboratory Diagnosis: motile Trophozoites visible in vaginal and prostate secretions. • Clinical Finding: A watery, foul-smelling, yellowgreenish vaginal discharge accompanied by itching 52 and burning occurs. 53 Trophozoites: pear-shaped, a central nucleus and four flagella. Trichomonas - Stained vaginal secretion 54 Trichomonas vaginalis Trichomoniasis 55 Trichomoniasis • Men: asymptomatic OR urethritis, prostatitis • Women: asymptomatic OR mild to severe vaginitis copious yellowish, frothy discharge strawberry cervix “colpitis macularis” 56 Trichomoniasis • Risk factors – Infection with other STDs, especially gonorrhea – Four or more lifetime sex partners – Sexual contact with an infected partner – Not using barrier contraception – Trading sex for money or drugs 57 T. vaginalis - Vaginal discharge 58 Trichomonas vaginalis • Treatment: Metronidazole for both sexual partners. • Prevention: Condoms limit transmission 59 60 Isospora belli ISOSPORIASIS Transient diarrhea in healthy pts and severe in IC Forms and transmission Fecal oral ingestion of oocysts. Pathogenesis: The oocysts excyst in the upper small intestine and invade the mucosa, causing destruction of the brush border. Dx: ACID FAST & ELLIPTICAL OOCYSTS RX: TMP-SMX OR PYRIMETHAMINE/SULFADIAZINE Note: causes malabsoption similar to giardia 61 CYCLOSPORA CAYETANENSIS • MILD WATERY DIARRHEA IN HEALTHY AND SEVERE IN IC • Member of coccida(subtype of sporozoa) • TRANSMISSION: fecal oral(via contaminated water) • Dx;spherical oocysts in modified acid fast stain of a stool sample • Rx:trimethoprim sulfamethoxazole. 62 MICROSPORIDIA • Characterized by obligate intracellular replication and spore formation • Persistent diarrhea in AIDS pts(Enterocytozoon bieneusi and Septata intestinalis) • Tx: fecal oral • Dx: spores in stool • Rx: albendazole • Others: no proven treatment 63 Balantidium coli • only ciliated protozoan that causes human disease, ie, diarrhea. • hosts: cows, pigs and horses farm work, rural dwellers. • MOT: ingestion of cysts • similar to entamebiasis (extraintestinal lesions do not occur) • liver, lung and brain abscesses are not seen. • Diagnosis is made by finding large ciliated trophozoites or large cysts with a characteristic V-shaped nucleus in the stool. • The treatment of choice is tetracycline. Prevention consists of avoiding contamination of food and water by 64 Simply keep a place within you where it is welcomed, and happiness will come and abide with you forever.!!!!!!!!!!!!! 65