Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
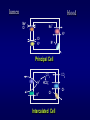
Potassium Balance and Potassium Imbalance Part Ⅰ Potassium Balance Ⅰ Content and Distribution of Potassium in the Body Ⅱ Intake and Excretion of Potassium Dietary K intake Serum [K+] round 4.5mmol/L 70~100mmol/day ECF 2% K+ ICF [K+] 160mmol/L Excretion 98% of the total body potassium Total body K content 31~57mmol/Kg body weight Skin trivial normally Colon 10% Kidneys > 80% More ingested, more excreted Less ingested, less excreted Not ingested, excretion goes on Content, distribution, intake and excretion of K Ⅲ Maintenance of Potassium Homeostasis —Distribution of K+ across the cell membrane and Regulation of renal K+ excretion Distribution of Potassium across the Cell Membrane The Na+/K+ATPase membrane pump and permeability of ion channels Influencing Factors 1.Hormones — insulin, glucagon, catecholamines, thyroid hormone 2.Serum K+ Na+/K+ATPase [K+] [K+]↑ Catecholamine 3.pH of ECF and plasma osmolality 4.Others — rate of cell breakdown, hypoxia, hypothermia, exercise Na+ Insulin K+ H+ Regulation of Renal Potassium Excretion Filtration, Cl- and secretion reabsorption of potassium Na+/K+ATPase( Mg2+ activated) The nephron and collecting tubule Na+/K+ATPase H+- K+ ATPase Regulation of Renal Potassium Excretion Filtration, reabsorption and secretion of potassium Secretion of potassium in the distal and collecting tubules principal cells, with Na+/K+ATPase membrane pump, for secretion of K+ lumen blood Na+ Cl- Na+ K+ ClK+ K+ Principal Cell CO2 H+ K+ CO2 HCO3Cl- Intercalated Cell Cl- Regulation of Renal Potassium Excretion Filtration, reabsorption and secretion of potassium Secretion of potassium in the distal and collecting tubules Reabsorption of K in the distal and collecting tubules, intercalated cells, with H+/K+-ATPase (proton pump) for reabsorption of K+ Regulation of Renal Potassium Excretion Filtration, reabsorption and secretion of potassium Secretion of potassium in the distal and collecting tubules Reabsorption of K in the distal and collecting tubules intercalated cells, with H+/K+-ATPase (proton pump) for reabsorption of K+ Factors influencing excretion of K+ by the distal and collecting tubules Factors Influencing Excretion of K+ by the Distal and Collecting Tubules — activates Na+/K+ATPase, increase membrane permeability to K [K+] in the ECF Flow rate of tubular fluid in the distal tubule pH of ECF —↓pH inhibits Na+/K+ATPase Aldosterone Factors Influencing Excretion of K+ by the Distal and Collecting Tubules lumen + Na+ Na+ Cl- + flow rate + ClK+ K+ + [K+ ]↑ K+ CO2 HCO3- + Ald K+ + ① ② ③ Principal Cell H+ blood Cl- Intercalated Cell CO2 Cl- [H+ ]↑ + Maintenance of Potassium Homeostasis Distribution of potassium across the cell membrane Regulation of renal potassium excretion Excretion of K by the Colon also controlled by aldosterone Function of Potassium in the Body The part K+ Ⅳ plays in metabolism Maintenance of the resting membrane potential of excitable cells in the Body Function of Potassium Maintenance and regulation of osmotic pressure and acid-base balance both in ICF and ECF Part Ⅱ Potassium Imbalance ---abnormal changes in [K+] in ECF Hypokalemia Serum [K+]<3.5mmol/L,may or may not be associated with K deficit Etiology and Pathogenesis Dietary intake Serum [K+] < 3.5mmol/L ECF 2% Excessive losses shifting ICF [K+] may or may not be decreased Total body K content — decreased (K deficit) or — normal G.I losses---diarrhea, vomiting Renal losses---diuretics, some diseases of the kidney Losses from the skin---profuse sweating, burns Crude cotton seed oil poisoning Etiology and Pathogenesis Ⅰ. Inadequate Intake anorexia, inability to eat, Ⅱ. Fasting, Excessive Losses prolonged IV alimentation without K 1.Gastrointestinal losses supplementation, alcoholism Vomiting →mainly increased excretion Diarrhea →extrusion of largerenal amount of + due to metabolic alkalosis caused by of K alkaline liquid stool with a high content loss of gastric acid,acidosis, contraction ECF of K→K depletion, ECFofvolume volume contraction →↑secretion of aldosterone Etiology and Pathogenesis Ⅰ. Inadequate Intake Ⅱ. Excessive Losses 1.Gastrointestinal losses 2.Excessive renal losses (1)Diuretics→increased flow rate and delivery of Na+,Cl- and water to the distal tubule → increased Na+-K+ exchange; volume contraction →increased aldosterone → renal K excretion↑ Regulation of Renal Potassium Excretion ClNa+/K+ATPase Na+/K+ATPase( Mg2+ activated) The nephron and collecting tubule H+- K+ ATPase Etiology and Pathogenesis Ⅰ. Inadequate Intake Ⅱ. Excessive Losses 1.Gastrointestinal losses 2.Excessive renal losses (1) Diuretics (2) Some diseases of the kidney Renal tubular acidosis Excessive Renal Losses (1) Diuretics (2) Some diseases of the kidney Renal tubular acidosis Diuretic recovery phase of acute renal failure (3) Antibiotics (4) Excess of adrenocortical hormones Aldosteronism, Cushing’s syndrome (5) Magnesium deficiency Regulation of Renal Potassium Excretion ClNa+/K+ATPase Na+/K+ATPase( Mg2+ activated) The nephron and collecting tubule H+- K+ ATPase Case Report A female patient, 42 years old, was admitted to the affiliated hospital of the Sichuan Med.College as an emergency case on April 4 1978, with a chief complaint of decreased food intake, nausea and frequent vomiting for 20 days. She had a history of diabetes mellitus for 3 years. Diagnosis: Diabetic ketoacidosis, which is a medical emergency. She was treated with insulin, with success. She was also found to have infection of the urinary tract as well as severe hypokalemia (the serum [K+] was around 2mmol/L). Therefore she was given large doses of gentamycin for 33 days. KCl was also administered, both by mouth and IV instillation, in large doses, for 41 days. However, hypokalemia persisted (2.55mmol/L). To the surprise of the doctor, the patient suddenly developed spastic rigidity of the limbs. It was until then, 41days after admission, the doctor examined the serum [Mg2+], it was very low:0.2mmol/L!(The normal range of serum [Mg2+] being 1.5~2.5mmol/L). IV MgSO4 was immediately given, and also for several days, with complete success! The doses of KCl was reduced, however, the serum [K+] rose to normal levels within 3 days! Serum [Mg2+] also turned normal. No adverse reactions.(《中华内科杂志》1980年1月) Questions:1. What is the cause or what are the causes of hypokalemia and hypomagnesemia in this patient? 2. Why did the doctor fail to diagnose hypomagnesemia earlier? Excessive Renal Losses (1) Diuretics (2) Some diseases of the kidney Renal tubular acidosis Diuretic recovery phase of acute renal failure (3) Antibiotics (4) Excess of adrenocortical hormones Aldosteronism, Cushing’s syndrome (5) Magnesium deficiency (6) Alkalosis Etiology and Pathogenesis Ⅰ.Inadequate Intake Ⅱ.Excessive Losses 1. Gastrointestinal losses 2. Excessive renal losses 3. Excessive losses from the skin Profuse sweatings, burns or scalds Etiology and Pathogenesis Ⅰ.Inadequate Intake Ⅱ.Excessive Losses Ⅲ.Shifting of K+ from the ECF to ICF 1.Overdose of insulin 2.-adrenergic agonist overdose K+ Na+/K+ATPase Na+ Albuterol Insulin K+ H+ Etiology and Pathogenesis Ⅰ.Inadequate Intake Ⅱ.Excessive Losses Ⅲ.Shifting of K+ from the ECF to ICF 1.Overdose of insulin 2.-adrenergic agonist overdose 3.Alkalosis 4.Barium poisoning 5.Familial hypokalemic periodic paralysis K+ Na+/K+ATPase Na+ Albuterol Insulin K+ H+ Etiology and Pathogenesis Ⅰ.Inadequate Intake Ⅱ.Excessive Losses Ⅲ.Shifting of K+ from the ECF to ICF Crude Cotton Seed Oil poisoning Effects on the Body — factors influencing the effects: the underlying diseases, the degree of hypokalemia and rapidity of its development, the ratio of [K+]i / [K+] e Effects on Neuromuscular Excitability Nernst equation Em= -60lg[K+]icf / [K+]ecf (mv) +35 Millivolts 0 -60 Threshold -90 Milliseconds The Resting Membrane Potential (RMP) and Action Potential (AP) of a skeletal muscle cell in the normal state Acute Hypokalemia [K+]i / [K+]e ↑ RMP more negative than normal hyperdepolarization block, excitability↓ muscle weakness, flaccid paralysis, smooth muscle symptoms mv 30 0 Action potential (AP) -30 -60 TMP -90 RMP -120 Normal Low [K+] High [K+] The effects of serum K+ concentration on cellular membrane excitability Chronic Hypokalemia ratio of [K+]i to [K+]e may be normal, RMP and excitability unchanged, interfering with cellular metabolism and vasodilation of muscles during exercise Effects on the Heart A Brief Review of the Bioelectric Phenomena of the Heart RMP and AP of a Ventricular Muscle Cell of the Heart a: effective refractory period; b: relative refractory period c: supranormal period The Membrane Potential of Atrial Muscle, and Purkinje’s Fiber 40 +20 Purkinje’s fiber Atrial muscle 1 1 2 2 0 -20 40 0 3 0 3 60 80 100 4 RMP 4 4 4 max.diast.potential 1.Effects on excitability RMP<-90mv, excitability Ca2+ inflow plateau, ERP shortened Phase 3, SNP prolonged AP prolonged normal low [K+]e a.mus. v.mus. Threshold potential repolarization normal prolonged Effects of low serum [K+] on the action potential of the myocardial cell 2. Effects on autorhythmicity K channel conductance of the cell membrane of the fast response autonomic cells acceleration of spontaneous diastolic depolarization, autorhythmicity The Membrane Potential of Purkinje’s Fiber 1 2 normal 0 4 max.diast.potential 3 hypokalemia 4 3. Effects on conductivity Amplitude and rapidity of phase 0 depolarization smaller than normal conductivity Cardiac arrhythmias due to increased excitability, shortened ERP, prolonged SNP, increased autorhythmicity and decreased conductivity The conducting system of the heart RMP and AP of a Ventricular Muscle Cell of the Heart a: effective refractory period; b: relative refractory period c: supranormal period conductivity and cardiac arrhythmias —— reentry of excitation (2) conduction slowed down (1) normal stalk stalk ventricular muscle stalk ventricular muscle stalk (3) monodirectional block stalk branch A branch B monodirectional block ventricular muscle Ventricular premature excitation resulted from reentry of excitation action potential ECG ventricular muscle (4) conduction slowed down + monodirectional block reentry of excitation Schematic diagram showing reentry of excitation in a Purkinje’s fiber-ventricular muscle circuit 4.Effects on contractility increased in acute hypokalemia, decreased in chronic hypokalemia Effects on the Kidney functional and mosphological changes Effects on Metabolism carbohydrate metabolism, protein metabolism, acid-base balance Effects on the Nervous System documented symptoms, contradictory reports Principles of Prevention and Treatment Ⅰ. Measures against the causes Ⅱ. Replacement therapy with potassium 1.Oral replacement: 40~120mmol of K/day 2.IV instillation: KCl≤40mmol/L, ≤10mmol of K/h Never inject! Monitor serum [K+] and ECG Hyperkalemia serum [K+]>5.5mmol/L, a medical emergency Etiology and Pathogenesis Inadequate excretion of K Renal failure, hypoaldosteronism, K sparing diuretics Redistribution of K in the body tissue injury, acidosis, insulin deficiency, familial hyperkalemic periodic paralysis Increased intake of K—rapid IV K administration Effects on the Body Ⅰ.Effects on neuromuscular excitability In mild to moderate hyperkalemia the ratio of [K+]i to [K+]e RMP less negative than normal, excitability abnormal sensibility (paresthesia), diarrhea Severe hyperkalemia, RMP decreased to level of TMP, depolarization block muscle weakness, paralysis, dizziness, coma Effects on the Body Ⅰ.Effects on neuromuscular excitability Ⅱ.Effects on the heart 1.Effects on excitability In mild to moderate cases, excitability , phase 0 upstroke smaller and slower; In severe cases, no AP can be induced cardiac arrest Phase 2 plateau prolonged, phase 3 repolarization shortened Effects on the Body Ⅰ.Effects on neuromuscular excitability Ⅱ.Effects on the heart 1.Effects on excitability 2. Effects on autorhythmicity K channel conductance , autorhythmicity Effects on the Body Ⅰ.Effects on neuromuscular excitability Ⅱ.Effects on the heart 1.Effects on excitability 2. Effects on autorhythmicity 3.Effects on conductivity a smaller and slower phase 0 upstroke conductivity Effects on the Body Ⅰ.Effects on neuromuscular excitability Ⅱ.Effects on the heart 1.Effects on excitability 2. Effects on autorhythmicity 3.Effects on conductivity 4.Effects on contractility high serum [K+] inflow of [Ca2+] contractility Effects Effects on on Acid-Base the BodyBalance ECF [K+] secretion of insulin and Ⅰ. Effects on neuromuscular excitability + aldosterone ECF [K ] shifted into cells +] move out while [H Ⅱ. Effects on the heart ECF [K+] Na+-K+ exchange in renal Ⅲ. Effects on acid-base balance + distal tubules and secretion of H ECF [K+] renal NH4 production, acid retention metabolic acidosis Principles of Prevention and Treatment Restriction of K intake, control of underlying diseases, insulin + glucose, use of Ca2+ and Na+ to counteract K, bicarbonate infusion, ion-exchange resin, dialysis