Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
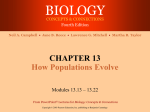
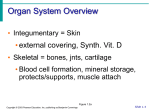
POWERPOINT® LECTURE SLIDE PRESENTATION by LYNN CIALDELLA, MA, MBA, The University of Texas at Austin Additional Text by J Padilla Exclusively for physiology at ECC UNIT 3 15 PART A Blood Flow and the Control of Blood Pressure HUMAN PHYSIOLOGY AN INTEGRATED APPROACH DEE UNGLAUB SILVERTHORN Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings FOURTH EDITION Overview: Cardiovascular System Arteries take blood away from the heart and veins return it. Arteries connect to arterioles, that connect to capillaries, that connect to venules, that connect to veins Two portal systems shown here have two sets of capillaries connected Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 14-1 Functional Model of the Cardiovascular System Systemic Arteries maintain pressure during ventricular relaxation by changing vessel diameter Arteries and veins are for travel and capillaries for exchange Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-1 Blood Vessel Structure Blood vessels vary in diameter and wall thickness. Veins have a larger diameter and thinner walls than arteries. Capillaries are thin enough to allow for diffusion and narrow to restrict RBC to flow in single file Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-2 Metarterioles Capillaries lack smooth muscle and elastic tissue reinforcement which facilitates exchange The walls are thin enough to allow WBC and plasma to scape. Plasma that leaves the capillaries and bathes the tissues will be called lymph and will be collected by lymphatic capillaries. Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-3 Precapillary Sphincters Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-15a Capillaries: Exchange Plasma and cells exchange materials across thin capillary wall Capillary density is related to metabolic activity of cells Capillaries have the thinnest walls Single layer of flattened endothelial cells Supported by basal lamina Bone marrow, liver and spleen do not have typical capillaries but sinusoids Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Two Types of Capillaries Continous Capillary Fenestrated Capillary Sinusoidal Capillary Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Angiogenesis New blood vessel development- after birth, happens to accommodate tissue growth like when one gains weight Necessary for normal development- growth needed during childhood Wound healing and uterine lining growth- blood vessel formation needed in adulhood Controlled by cytokines- chemical signal that induce mitosis Mitogens: VEGF and FGF- vascular endothelial growth factor and fibroblast growth factor Inhibit: angiostatin and endostatin- these natural occuring chemicals are being used to treat cancer and coronary disease Coronary heart disease Collateral circulation- natural formation of additional blood vessels to supplement flow of blocked vessels Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Velocity of Blood Flow Velocity of flow depends on total cross-sectional area of the vessels. The greater the total cross-sectional area the slower the velocity. Velocity is slowest at the capillaries. Although the diameter of a capillary is smaller than any other vessel its total cross-sectional area is greater than any other. Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-17 Review of Blood Flow Flow is inversely proportional to resistance. Resistance is influenced by vessel diameter. The larger the diameter the slower the speed as long as the flow rate is constant. Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Pressure Differences in Static and Flowing Fluids Pressure falls over distance as energy is lost because of friction. In circulation the further away the blood is from the heart the lower the pressure. Pressure is lower is veins than in arteries Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 14-3a Fluid Flow through a Tube Flow ∆P Pressure gradient cause a fluid to flow . Blood vessels create pressure gradients by altering diameter size Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 14-4 The Role of Radius in Determining Resistance to Flow A small change in diameter can use a great change in resistance and flow. Thus blood vessels can dramatically alter blood flow when they vasoconstrict or vasodialate Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 14-5 Fluid Rate Versus Velocity of Flow The velocity of flow is influenced by cross-sectional area. Although a large cross-sectional area may allow more fluid to pass at one time, it also causes it to slow down. Don’t think of cross-sectional area as the diameter of the blood vessel. Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 14-6 Pressure throughout the Systemic Circulation Blood pressure is highest in the arteries and decreases continuously as it flows through the circulatory system. Systolic pressure is exerted on vessel walls when the heart contracts Diastolic pressure is pressure during heart relaxation. Pulse pressure measures strength of pressure wave systolic P – diastolic P Mean arterial pressure measures driving pressure diastole P + 1/3 pulse pressure. Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-5 Elastic Recoil in Arteries This process explains how pressure is transferred to blood vessels when the heart contracts (a) Ventricular contraction Arterioles 1 2 3 1 Ventricle contracts. 3 2 Semilunar valve opens. Aorta and arteries expand and store pressure in elastic walls. Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-4a Elastic Recoil in Arteries This process explains how pressure is maintained in blood vessels while the heart relaxes (b) Ventricular relaxation 1 2 3 1 Isovolumic ventricular relaxation occurs. 3 2 Semilunar valve shuts, preventing flow back into ventricle. Elastic recoil of arteries sends blood forward into rest of circulatory system. Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-4b Measurement of Arterial Blood Pressure Pulse Pressure = systolic P – diastolic P Valves ensure one-way flow in veins MAP = diastolic P + 1/3(systolic P – diastolic P) Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-7 Pressure Change Pressure created by contracting muscles of the heart and blood vessels is transferred to blood Driving pressure is created by the ventricle. Thus usually blood pressure reading focus on left ventricular systole and diastole and arterial pressure not venous pressure. If blood vessels constrict, blood pressure increases because the diameter decreases and the muscle exerts more pressure on the blood. If blood vessels dilate, blood pressure decreases because the opposite happens. Blood volume changes are major factors for blood pressure in CVS. Drinking a lot of fluid increases blood volume, blood loss and dehydration decreases blood volume. The kidneys try to regulate blood volume via fluid loss or retention. The CV system cause changes in diameter to help compensate when posible. Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Blood Pressure Blood pressure control involves both the cardiovascular system and the renal system Increase or decrease in blood volume is compensated by CV and kidney changes Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-9 Stroke Volume and Cardiac Output Stroke volume Amount of blood expelled by one ventricle during a contraction EDV – ESV = stroke volume Force of contraction Stroke volume increases of decreases based on contraction force Affected by length of muscle fiber and contractility of heart Frank-Starling law Stroke volume increase as EDV increases EDV determined by venous return Skeletal muscle pump Respiratory pump Sympathetic innervation Cardiac output Volume of blood pumped by one ventricle in a given period of time CO = HR SV (heart rate times stroke volume) Average = 5 L/min Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Factors that Affect Cardiac Output Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 14-31 Blood Pressure Mean arterial pressure is a function of cardiac output and resistance in the arterioles= the volume produced by the heart times vessel radius (vasodilation/vasoconstriction) Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-8 Arteriolar Resistance (vasoconstriction) Sympathetic reflexes- control blood distribution as needed to maintian homeostasis such as body temperature Local control of arteriolar resistance- based on metabolism of tissue and tissue needs for blood flow, can override CNS control in heart and muscle Hormones- those that bind to kidney cells and control salt and water levels. Myogenic autoregulation- increased blood flow causes increase pressure that stretches the walls. The smooth muscle responds by contracting thus increasing resistance and reducing flow. Therefore, no neural input is needed Paracrines –secreted by endothelium, allows for local control Active hyperemia- increase blood flow accompanies increased metabolic activity. As more paracrines accumulate, they call for more blood. Reactive hyperemia- increase blood flow after a state of abnormally low metabolic rate due local hypoxia. Nitric oxide is made for vasodilation Sympathetic control SNS: norepinephrine; tonic release maintains myogenic tone, increase release causes vasoconstriction Adrenal medulla: epinephrine: heart, liver, and skeletal muscle vasodilate Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Hyperemia Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-11a Norepinephrine Tonic control of arteriolar diameter Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-12 Factors that Influence Mean Arterial Pressure Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-10 Blood Pressure Components of the baroreceptor reflex KEY Stimulus Sensor/receptor Integrating center Efferent pathway Effector Medullary cardiovascular control center Change in blood pressure Carotid and aortic baroreceptors Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-21 Blood Pressure KEY Medullary cardiovascular control center Stimulus Sensor/receptor Integrating center Efferent pathway Change in blood pressure Effector Parasympathetic neurons Carotid and aortic baroreceptors Sympathetic neurons Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-21 (5 of 10) Blood Pressure KEY Medullary cardiovascular control center Stimulus Sensor/receptor Integrating center Efferent pathway Change in blood pressure Effector Parasympathetic neurons Sympathetic neurons Carotid and aortic baroreceptors SA node Ventricles Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-21 (8 of 10) Blood Pressure KEY Medullary cardiovascular control center Stimulus Sensor/receptor Integrating center Efferent pathway Change in blood pressure Effector Parasympathetic neurons Sympathetic neurons Carotid and aortic baroreceptors SA node Ventricles Veins Arterioles Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-21 (10 of 10) Blood Pressure The baroreceptor reflex: the response to increased blood pressure Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-22 Blood Pressure The baroreceptor reflex: the response to orthostatic hypotension Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-23 Distribution of Blood Distribution of blood in the body at rest Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-13 Cardiovascular disease (CVD): Risk Factors Risk factors that are not controllable Gender Age Family History Risk factors that are controllable Smoking Obesity Sedentary lifestyle Untreated hypertension Uncontrollable genetic but modifiable lifestyle Blood lipids Leads to atherosclerosis HDL-C versus LDL-C Diabetes mellitus Metabolic disorder contributes to development of atherosclerosis Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings LDL and Plaque The development of atherosclerotic plaques Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-24 Hypertension Graph shows the relationship between blood pressure and the risk of developing cardiovascular disease Essential hypertension has no clear cause other than hereditary Carotid and aortic baroreceptors adapt Risk factor for atherosclerosis Heart muscle hypertrophies Pulmonary edema Congestive heart failure Treatment Calcium channel blockers, diuretics, beta-blocking drugs, and ACE inhibitors Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15-25