Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Electrocardiography wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Jatene procedure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiac surgery wikipedia , lookup
Myocardial infarction wikipedia , lookup
Heart failure wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
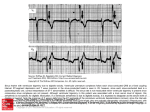
Congestive Heart Failure Eric J. Milie, D.O. Objectives: Recognize the different causes of right and left sided heart failure Understand the different diagnostic modalities used to evaluate patients with heart failure Explain the various therapeutic options available for patients with heart failure Definition: A pathopysiologic state characterized by congestion in the pulmonary or systemic circulation. It is caused by the heart’s inability to pump sufficient oxygenated blood to meet the metabolic needs of the tissues Preload: Degree of end-diastolic fiber stretch For clinical purposes, the end-diastolic pressure, especially if above normal, is a reasonable indicator of preload Conditions that may effect preload include: LV dilatation, hypertrophy, and changes in distensibility or compliance Afterload Force resisting myocardial relaxation after stimulation from the relaxed state Determined by chamber pressure, volume, and wall thickness at the time of aortic valve opening Clinically, approximates systolic BP at or neat the time of aortic valve opening and represents peak systolic wall stress Frank-Starling Principle Degree of end-diastolic fiber stretch (preload) within a physiologic range is proportional to the systolic performance of the ensuing ventricular contraction In effect in CHF, but suboptimal response because the ventricle function is abnormal Frank-Starling cont. The effects of myocardial compliance and contractility on the Frank-Starling mechanism. Figure reproduced from Internal Medicine, 4th edition, 1994, W.B. Saunders Frank-Starling cont. If Frank-Starling curve is depressed, fluid retention, vasoconstriction, and a cascade of neurohormonal responses lead to CHF Over time, LV remodeling, with hypertrophy and dilatation further compromises the heart’s function Left Ventricular Failure Characteristically develops in association with CAD, HTN, and most forms of cardiomyopathy and congenital defects (i.e. VSD, PDA) Right Ventricular Failure Most commonly caused by prior LV failure ( pulmonary venous pressure and leads to pulmonary artery HTN) and tricuspid regurgitation May be seen in the face of polycythemia, overtransfusion, acute renal failure, or vena caval obstruction Systolic Dysfunction Failure to provide the tissues with adequate circulatory output Most commonly caused by HTN, CAD, and dilated cardiomyopathy More than 20 viruses shown to be causal Diastolic Dysfunction Resistance to ventricular filling (20-40% of cases) Seen in hypertrophic cardiomyopathy, marked ventricular hypertrophy, and amyloid infiltration of the myocardium High Output Failure Persistently elevated cardiac output, resulting in ventricular dysfunction Conditions include anemia, beriberi, thyrotoxicosis, pregnancy, Paget’s disease, and AV fistula Treatment is aimed at the underlying cause Etiology: Left Ventricular Failure Right Ventricular Failure Systemic Hypertension Valvular Hear Disease (AS, AR, MR) Cardiomyopathy Myocarditis Bacterial Endocarditis Myocardial Infarction IHSS Valvular Heart Disease (MS) Pulmonary Hypertension Bacterial Endocarditis (right sided) Right Ventricular Infarction Clinical Manifestations Dyspnea: First on exertion, then with progressively less strenuous activity Orthopnea: Increased venous return in the recumbent position PND: multiple factors Nocturnal Angina: Increased cardiac workload, 2º to increased venous return Cheyne Stokes Respiration: Alternating phases of apnea and hyperventilation Fatigue: low cardiac output Peripheral Edema Physical Exam Left Sided Failure Right Sided Failure • • • • • Jugular Venous Distention • Peripheral Edema • Peripheral/ Perioral cyanosis • Hepatomegaly • Ascites • Hepatojugular Reflux Pulmonary Rales Tachypnea S3 Gallop Cardiac Murmurs (AS, AR, MR) • Paradoxical Splitting of S2 Assessment of JVD Shasham, Fadi, and Judith Mitchell, M.D. “Essentials of the Diagnosis of Heart Failure.” American Family Physician, March, 2001. Kortakoff’s Sounds with Valsalva Arterial blood pressure response and Korotkoff's sounds during Valsalva's maneuver. (A) Sinusoidal response in normal patient. (B) Absent overshoot in patient with heart failure. (C) Square wave response in patient with heart failure. The red lines indicate when Korotkoff's sounds are heard. (BP = blood pressure) Framingham Criteria for Diagnosis of CHF Major Criteria Minor Criteria • Paroxysmal Nocturnal Dyspnea • Neck Vein Distention • Rales • Cardiomegaly • Acute Pulmonary Edema • S3 Gallop • Increased Venous Pressure • + Hepatojugular reflux • • • • • • Extremity Edema Night cough Dyspnea on exertion Hepatomegaly Pleural Effusion Vital Capacity ↓ ⅓ from normal • Tachycardia (>120bpm) Major or Minor: Wt loss >4.5 kg over 5 days of treatment To establish a clinical diagnosis of CHF by these criteria, at least 1 major and 2 minor criteria are required Diagnosis: CXR Findings • • • • • • Cardiomegaly (Cardiothoracic ratio >0.5) Large Hila with indistinct margins Prominence of superior pulmonary veins Fluid in intralobar fissures Kerley B lines Alveolar edema Classic CXR Echocardiogram Two view and Doppler echocardiography is useful to assess blood flow, global and left ventricular function, and ejection fraction Transesophageal echo offers higher quality images, but is invasive and is best reserved for when the quality of the 2D images are unacceptable Echocardiography: Two-dimensional echocardiogram showing a four-chambers view of the heart in a patient with systolic dysfunction. Note dilated LV. Shasham, Fadi, and Judith Mitchell, M.D. “Essentials of the Diagnosis of Heart Failure.” American Family Physician, March, 2001. Echocardiography Two-dimensional echocardiogram showing a four-chambers view of the heart in a patient with diastolic dysfunction. Note the normal LV size with hypertrophy. EKG Should be performed on all patients with new diagnosis of CHF. No specific findings are indicitive of heart failure, but atrial and ventricular arrhythmias are common fidings. Atrial Fibrillation is found in roughly 25% of individuals with cardiomyopathy, especially elderly individuals with advanced failure Low voltage with conduction disturbances may be associated with amyloidosis Angiography Noninvasive method for assessing systolic and diastolic function May be used when echo findings not consistent with the clinical picture Ectopic activity and Atrial Fibrillation may adversely effect accuracy B-type Natriuretic Peptide New diagnostic test superior to diagnostic decision making of the primary care physician Has reduced clinical indecision from 43-11% Median BNP levels in NYHA classes I, II, III, and IV were 244, 389, 640, and 817 pg/ml, respectively. Values of 50 pg/ml or less had a negative predictive value of 96% Maisel, A et al. Rapid Measurement of B-Type Natriuretic Peptide in the Emergency Diagnosis of Heart Failure. New England Journal of Medicine. 2002 347(3):161-7. Functional Classification: New York Heart Association Class I: Symptomatic only with greater than normal activity Class II: Symptomatic with ordinary activity Class III: Symptomatic with minimal activity, asymptomatic at rest Class IV: Symptomatic at rest Treatment 1. Removal of the precipitating cause 2. Correction of the underlying cause 3. Prevention of deterioration of cardiac function 4. Control of the congestive heart failure state Drug Treatment of Systolic Dysfunction Diuretics ACE inhibitors ARBs Β-blockers Digitalis Most patients treated with at least two of the above Diuretics Diuretics continued Loop diuretics are preferred, usually furosemide by mouth In resistant cases, Bumetanide 0.5 – 2.0mg or Metazolone PO may have additive effects Overuse may cause electrolyte imbalances (hyponatremia, hypomagnesemia, and profound hypokalemia) or volume deficits, so routine monitoring of serum electrolytes is warranted May induce renal failure in some patients Adding K sparing diuretics may be used to offset the K-losing effects of loop diuretics Spironolactone may be beneficial in advanced (NYHA Class III or IV) cases of CHF, decreasing total morbidity and mortality. Pitt B, Zannad F, Remme WJ, Cody R, Castaigne A, Perez A, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med 1999;341:709-17. Diuretics cont. Clinical efficacy of diuretics is heavily dependant on dietary sodium restriction Log of daily weights should be maintained ( in greater than 2# needs to be evaluated) No overall decrease in mortality, but relief of symptoms Konstam MA. Heart failure: evaluation and care of patients with left-ventricular systolic dysfunction. Rockville, Md.: U.S. Dept. of Health and Human Services, Agency for Health Care Policy and Research, 1994; Clinical Practice Guideline no. 11, AHCPR publication no. 94-0612. ACE Inhibitors Peripheral and arterial vasodilatation ↓ left ventricular filling pressure at rest and during exercise Favorable effects on remodeling Negative inotropic effect on the failing heart Decrease in overall mortality by 25-35% Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). The CONSENSUS Trial Study Group. N Engl J Med 1987;316:1429-35. ACE Inhibitors cont. Most common side effect is cough (520% of patients) probably 2º to build-up of bradykinin Caution in renal impairment, especially with concomitant use of diuretics ASA reduces the effects of ACE Inhibitors in CHF patient (inhibits the effects of kinins) ARBs Theoretically as effective as ACEInhibitors No associated cough (no effect on kinins) Losartan shown to decrease overall mortality in patients with heart failure No comparison trials (though ONTARGET is ongoing) Sharma D, Buyse M, Pitt B, Rucinska EJ. Meta-analysis of observed mortality data from allcontrolled, double-blind, multiple-dose studies of losartan in heart failure. Losartan Heart Failure Mortality Meta-analysis Study Group. Am J Cardiol 2000;85:187-92. Hydralazine/ Oral Nitrate Used in patients with increased serum creatinine levels, or those who cannot tolerate ACEI Decrease overall mortality by 25-30% Benefit in overall mortality not as pronounced as in ACEIs, and not as easy to take or tolerate Cohn JN, Archibald DG, Ziesche S, Franciosa JA, Harston WE, Tristani FE, et al. Effect of vasodilator therapy on mortality in chronic congestive heart failure. Results of a Veterans Administration Cooperative Study. N Engl J Med 1986;314:1547-52. Digitalis Weak inotrope Blockade of AV Node Weak vasoconstrictor Improves renal blood flow Modestly improves LV function Lowers dosage needed of diuretics Reduces need for hospitilization Digitalis cont. Digitalis Investigation Group (DIG) study showed no decrease in mortality, but significant reduction in the number of hospitalizations in patients treated with digitalis The Digitalis Investigation Group. The effect on digoxin in mortality and morbidity in patients with heart failure. N Eng J Med 1997;336:525-533 Digitalis Toxicity 1st degree AV block, which may progress to Wenkebach. May also see life threatening arrhythmias (V. Fib., V. Tach.) Nausea, Vomiting, Anorexia, Diarrhea, Confusion, Amblyopia, and Xerophthalmia (yellow vision) Digitalis Effect- EKG American Society of Consultant Pharmacists, Inc. β-Blockers Increase ejection fraction Reduce mortality by roughly 30%, if used properly Improved myocardial function achieved in 6-12 months of therapy CIBIS II: Bisoprolol reduced cardiac deaths and hospitalizations compared to control The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial. Lancet 1999;353:9-13. Heidenreich PA, Lee TT, Massie BM. Effect of beta-blockade on mortality in patients with heart failure: a meta-analysis of randomized clinical trials. J Am Coll Cardiol 1997;30:27-34 β-Blockers cont. Carvedilol (Coreg) is the only β-blocker specifically labeled for the treatment of heart failure Found to be more effective than other βblockers in patients without ischemic heart disease Bonet S, Agusti A, Arnau JM, Vidal X, Diogene E, Galve E, et al. Beta-adrenergic blocking agents in heart failure: benefits of vasodilating and non-vasodilating agents according to patients' characteristics: a meta-analysis of clinical trials. Arch Intern Med 2000;160:621-7. Ca-Channel Blockers Use in patients with decreased LV function has been disappointing Some Ca-Channel blockers have deleterious effect in systolic dysfunction (Verapimil, Nifedipine, Diltiazem) Diastolic Dysfunction Treatment May not tolerate reduced volume or blood pressure (vasodilators, diuretics relatively contraindicated) ACEIs and ARBs may decrease LV mass and stiffness Valve replacement may improve LV function Treatment of underlying dominant systolic dysfunction Definitive Treatment Heart transplant only treatment that potentially alters the long term course of the disease 1- and 3-year survival rates 80% & 75%, respectively Dynamic cardiomyoplasty: experimental; wrap the latissimus dorsi muscle around heart to stimulate contractility (reported functional status in 80% of pts, no long term data) Implantable ventricular assist devices are being studied, no long term data at this time Case Study Mr. Balaban, a 63-year-old Filipino man, has recently been traveling in the Philippines. He has a long history of hypertension and usually takes one aspirin, Lisinopril, and hydrochlorothiazide (HCTZ). He admitted that he ran out of these when he was traveling. After he returns home, he tells his daughter that he is "very tired", gets short of breath while walking around the house, and can't put his shoes on. As he talks with his daughter, she notices that he is having trouble talking, as if it is hard for him to breathe. She becomes alarmed and takes him to the emergency room where the physician finds the following: - 3+ pitting edema in both ankles - faint crackles in both lung fields - extreme fatigue- jugular vein distention when sitting - moderate shortness of breath - ten-pound weight gain in the last week- B/P 170/110; pulse 88 and irregular; EKG shows sinus tachycardia with nonspecific ST/T changes Question One: Based on the patient’s presentation in the emergency department, what would you expect his BNP level to be? A. 27 B. 250 C. 350 D. 500 E. 775 Answer: E. BNP value for Class III Heart Failure is above 640 pg/ml, Class IV above 817 pg/ml. Pt getting SOB with walking around the house, talking on the phone. No mention of dyspnea at rest. Most likely Class III-IV Question Two: While under your care, a routine BMP shows the patient to have a serum Creatinine of 2.3. Which of the following pharmacological agents will have the greatest benefit towards decreasing this patient’s risk of mortality? A. Lanoxin B. Verapimil C. Increasing dose of HCTZ D. Hydralazine/ Isosorbide E. Nifedipine Answer: D. VACS trial showed a decrease in the overall mortality in patients receiving this medication roughly 20-25%. Question Three: You evaluate the patient two months after his hospital discharge. He is complaining of generalized malaise, with nausea and vomiting over the past two to three days, and has noted things have taken on a yellowish tint while looking at them over the past week. The family notes that he has been increasingly confused since his discharge. On physical exam, the patient has a pulse rate of 72. An EKG recorded in the office shows a sinus rhythm, with a PR interval of 0.22 and “scooped out” appearing ST segments. Which of the following medications was the patient most likely discharged from the hospital on? A. Lasix B. Losartan C. Digoxin D. Coreg E. Norvasc Answer: D. The patients clinical presentation is classical for digoxin toxicity/ In addition, the EKG findings of scooped out ST segments and 1st degree heart block are commonly seen on patients treated with digitalis. Resources: Beers, et al. The Merck Manual of Diagnosis and Therapy. Seventeenth edition. Ch 261. 2004. Braunwald, et al. Harrison’s Principles of Internal Medicine. Fifteenth edition. Pp 1316-1332. 2001. Marino, Paul. The ICU Book. Pp 242-246. Rose Tree, Maryland. 1998.