Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Coronary artery disease wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Jatene procedure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
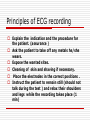
ECG Dr. Amal Al Maqadma Teaching assistant IUG MI When myocardial blood supply is abruptly reduced to a region of the heart, a sequence of injurious events occur : Ischemia ( subendocardial or transmural) Injury Necrosis, and eventual fibrosis (scarring) if the blood supply isn't restored in an appropriate period of time Hyperacute T wave is the earliest sign of acute myocardial infarction Precordial Septal Leads V1 – V2 – Look at the Septum of the heart – The septal branch of the LAD Precordial Anterior Leads V3 – V4 –anterior wall of the left ventricle –The LAD diagonal branch) Anterior-Septal Terminology Lateral Precordial Leads I,AVL,V5 – V6 lateral of the left ventricle The left circumflex Inferior border leads II, III and aVF the Inferior wall of the RV Posterior Descending Branch of the RCA. Posterior MI No leads look at the posterior wall. usually associated with inferior and/or lateral wall MI. The changes of posterior myocardial infarction are seen indirectly in the anterior precordial leads. Leads V1 to V3 face the endocardial surface of the posterior wall of the left ventricle. As these leads record from the opposite side of the heart instead of directly over the infarct, the changes of posterior infarction are reversed in these leads. The R waves increase in size, becoming broader and dominant, and are associated with ST depression and upright T waves. This contrasts with the Q waves, ST segment elevation, and T wave inversion seen in acute anterior myocardial infarction. ST depression is considered reciprocal ECG changes in what should be ST elevation for acute posterior wall injury. ECG Leads - Views of the Heart lead V3 & V4 V1 & V2 a VL,V5 & V6 II+III+AVF border Arterial supply anterior Right RCA Ventricle Septum LAD Lateral Left LCX Ventricle inferior RCA borderof right ventricle Principles of ECG recording Explain the indication and the procedure for the patient. (assurance ) Ask the patient to take off any metals he/she wears. Expose the wanted sites. Cleaning of skin and shaving if necessary. Place the electrodes in the correct positions . Instruct the patient to remain still (should not talk during the test ) and relax their shoulders and legs while the recording takes place (1 min) See video How to comment on ECG Name.Age ,Date and time. Calibration and Speed of paper RAWIHI : RAWIHI R: rate, regularity,rhythm(sinus or asinus), A: axis. W:waves. I :intervals. H: hypertrophy. I: ischemia Normal Sinus Rhythm Rate = 60-100 beat / minute. The rhythm is regular All intervals are within normal limits There is a P for every QRS and a QRS for every P. P : QRS ratio = 1 : 1. The P waves all look the same Presence of P, QRS, T in each cycle. Normal shape, time of waves, segments and intervals Interfering factors Inaccurate placement of the electrodes Electrolyte imbalances Poor contact between the skin and the electrodes Movement or muscle twitching during the test Drugs that can affect results include digitalis, quinidine, and barbiturates