Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Cardiac surgery wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
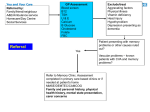
Heart Failure: From Failure to Success Dr. Alison Seed Consultant Cardiologist Failures? • In diagnosis • In routine management • In advanced management ₤ To address the personal AND financial burden Diagnosis........... Prevalence >45yrs National (expected) National Blackpool PCT (recorded) 2.3% 1.8% (0.19-5) 1.Pushing the boundaries: Improving services for people with heart failure. HCC(CHAI ) 2007 2. State of healthcare: Improvements and challenges for services in England and Wales. HCC (CHAI) 2007 3. Blackpool GP HF register data: Brian Harrop, Blackpool PCT Routine management.......... MORTALITY BENEFIT OF BETA-BLOCKERS AND ACE-INHIBITORS IN CHF TRIALS 16 S SOLVD (1991) CIBIS II MERIT-HF (1999) 14 % death at 1 year 12 10 8 6 4 2 0 diuretic digoxin diuretic digoxin ACE-I diuretic digoxin ACE-I diuretic digoxin ACE-I beta-blocker Advanced management........ Implant rate / million population / year Lancs. UK UK South target average Cumbria 2006 USA average EU average ICD 610 160 100 46 28 Bi V PPM 275 75 140 56 58 Personal and financial burden... Poor prognosis – 10-50% mortality per year Poor quality of life – Poor exercise tolerance – >30% depressive illness Frequent hospital admission – 5% of acute medical admissions – 40% death /readmission in one year Long length of stay – > 8 days – 2% of in patient bed days 2% total annual NHS expenditure Cost Hospital admission length of stay Healthcare Commission 2007 • HF diagnostic services poor − Diagnosis difficult because symptoms non specific and physical signs not obvious − Early diagnosis leads to appropriate life saving and symptom reducing treatment • Limited access to heart failure specialists − Need to target advanced treatments at high risk patients ₤ Rates of hospitalisation remain high Healthcare Commission. Pushing the boundaries: improving services for people with heart failure. London Healthcare Commission, 2007 Are we offering.......... Advanced Care or Palliative Care ........... to our Patients with Heart Failure? Currently (2009)…. Inequitable care Only for the symptomatic patient seeking help No more than Crisis management for the majority Palliative Care that could be better !! National drivers Quality Outcomes Framework ‘Advancing Quality’ (NW SHA) National HF database Darzi report – Equitable, efficient, patient centred care – Health improvement (outcomes and quality) – Adherence to best practice (NICE, NSF) Financial climate – Avoid hospital admission – Manage chronic disease in primary care Our aim…. ‘Best care’ whenever and wherever patients require it ............ Not currently seeking attention – Not yet diagnosed – With confirmed diagnosis New presentation − In Primary Care with symptoms Hospital admission(s) − With severe heart failure Our aim.... To demonstrate that optimal care is cost saving................... Failures? • Diagnosis • Routine management • Advanced management Definition: The first problem European society of Cardiology: ‘typically breathlessness or fatigue, either at rest or during exercise, or ankle swelling; and objective evidence of cardiac dysfunction at rest (usually on echocardiography)’ BLACKPOOL FYLDE AND WYRE HOSPITALS NHS FOUNDATION TRUST LANCASHIRE CARDIAC CENTRE Improving Diagnosis and Outcomes in Chronic Heart Failure PROPOSAL 1 Patients presenting with breathlessness and patients on the listed chronic disease registers, attending for routine review, should be asked to complete an NYHA questionnaire while waiting to see the practice Nurse / doctor. Those whose answers suggest that they are in NYHA II or above should have a BNP test and be considered for referral to the one stop Heart Failure Diagnostic Clinic (HFDC) or open access echocardiography service. Class New York Heart Association NYHA > II Further investigation required Symptom 1 No limitation Ordinary physical activity does not cause tiredness, breathlessness, chest discomfort or palpitation (an unexpected awareness of your heartbeat). 2 Slight limitation You are comfortable at rest but physical activity causes some tiredness, breathlessness, chest discomfort or palpitation (an unexpected awareness of your heartbeat). 3 Marked limitation You are comfortable at 4 Inability to carry out any physical activity without discomfort rest, but everyday activities cause marked tiredness, breathlessness, chest discomfort or palpitation (an unexpected awareness of your heartbeat). You have significant breathlessness or chest discomfort at rest. Any physical activity causes your symptoms to get worse. BNP Brain-type Natriuretic Peptide (BNP) is a hormone, secreted in the ventricular myocardium during periods of increased Atrial and ventricular wall tension It is the most powerful marker of cardiovascular morbidity and mortality including sudden death An elevated BNP indicates that the heart or kidneys are not working well but does not tell exactly why NICE Guidance 2010 Symptoms of HF Previous MI? NO YES Check BNP HIGH (>100) ‘VERY HIGH’ (>400) poor prognosis Refer for urgent Echo and Specialist assessment (within 2 weeks) Refer for Echo and specialist assessment routinely REFERRAL FORM AND CHECKLIST Please fax this referral and blood results if required to : Heart Failure Team Fax no: 01253 657845 or referral form initially to [email protected] Heart Failure Diagnostic Clinic HEART FAILURE DIAGNOSTIC CLINIC IS A ONE STOP DIAGNOSTIC CLINIC FOR ANY PATIENT WITH SYMPTOMS/SIGNS SUGGESTIVE OF HEART FAILURE BUT NO PREVIOUS DIAGNOSIS In addition to echocardiogram and in accordance with NICE guidelines the following will be considered : The aetiology of heart failure and treatment if required of this condition The need for additional diagnostic tests eg. stress echo, transoesophageal echo, angiogram Pharmacological and non pharmacological therapy The role of device therapy Diagnosis and management plan will be discussed with a view to increasing patient engagement / compliance A ‘patient held’ record of diagnosis / management will be produced and recorded on a National HF database This single visit to hospital will better support the subsequent management of the majority of pts in Primary Care The management and surveillance of the most complex/at risk patients will be undertaken by the hospital HF team in consultation with their General Practitioner and the Community HF team Patient details Referring GP Name : Name : Address : Address: Postcode : Tel. no : Tel.no : Fax. no: DOB : One stop Within 2 weeks NHS no : Hospital no : Referral date: PCT area : If the patient does not meet one of the following criteria or has had echocardiogram in the last twelve months – please do not refer to One Stop HFDC Refer to cardiology via usual channels or to the HF team directly by letter if previously known to them Yes Details The patient has symptoms suggestive of HF and history of myocardial infarction in the past The patient has symptoms suggestive of HF and an elevated BNP or BNP is unavailable to your practice BNP result : Hospital where assay performed: we are working with Cardiac Network to improve access APPOINTMENT AT HFDC WILL BE OFFERED WITHIN 2 WEEKS OF CHOOSE AND BOOK REFERRAL, RECEIPT OF COMPLETED REFERRAL FORM and if required (see above) BNP result All patients should have had blood taken for U&E and FBC – result need not delay referral REFERRAL TO HFDC WILL BE ACCEPTED WITHOUT BLOODS FOR THOSE WITH ALARM FEATURES THIS IS OFFERED ONLY AS AN ALTERNATIVE TO HOSPITAL ADMISSION IF FELT APPROPRIATE (please tick) Heart Failure Diagnostic Clinic Comprehensive specialist assessment History/ examination Echocardiogram Consideration of need for further investigation – Angiogram, TOE, stress test Management plan - Lifestyle Pharmacological Non pharmacological Device therapy Patient education / engagement • HF referral poster • AQ data Failures? • Diagnosis • Routine management • Advanced management Failures? • Diagnosis • Routine management • Advanced management Biventricular Pacemakers Right Atrial Lead Right Ventricular Lead ECG • P wave • QRS duration 37 38 Biventricular Pacemakers Right Atrial Lead Left Ventricular Lead Right Ventricular Lead Biventricular Pacemakers Biventricular Pacemakers 36% reduction in All Cause Death / CVS death /Hospitalisation CARE – HF: Cleland et al, NEJM, 2005 • Referral for CRT from North Lancs/ Blackpool Transplant vs. medical Rx Butler et al. J Am Coll Cardiol, 2004 Cardiopulmonary exercise testing Survival following cardiac transplant • 1 year: 85% • 5 years: 73% • 10 years: 58% www.uktransplant.org.uk Mechanical support: Ventricular assist devices Outflow: Ao Inflow: LV/LA • Bridge to transplant • Bridge to recovery • Destination therapy Who should receive a VAD as bridge to transplant? Heart Failure Service - Blackpool Timely and accurate diagnosis One stop diagnostic clinic Appropriate/safe/rapid referral pathways Identify high risk patients BNP Efficient and effective clinical care Treatment optimisation (NICE) Non pharmacological intervention (CRT / ICD, LVAD, Tx) Communication , Communication, Communication New presentation to GP Hospital Discharge HIGH RISK GROUP In order to reduce risk of readmission all inpatients will be seen during admission or early post discharge by specialist team Known diagnosis in Primary Care Previous MI? • Community Heart Failure Service No • Uptitration to maximal tolerated medical therapy BNP ? Yes > threshold Heart Failure One stop Diagnostic clinic • See referral form • Seen within 2 weeks • Aim discharge with management plan for majority • HF helpline • • • Ongoing surveillance / management of those at high risk of readmission Acute Trust HF nurse also available for advice / to facilitate seamless care HF helpline: 01253 303269 * Specialist Consultant led clinic to see all high risk patients ie. : • LBBB on ECG • New AF • Angina • Any ongoing symptoms despite maximal tolerated medical therapy • Uptitration to maximal tolerated medical therapy • Ongoing surveillance All patients should have routine 6 monthly review of: • Symptoms • Medication • ECG: LBBB, AF, HR • UE, FBC Specialist Consultant led HF clinic HIGH RISK GROUP Referral by: • Direct letter • HF helpline 01253 657865 • Discharge to GP of stable patients GP follow up Advice required High risk (see markers below) Unable to achieve target dose of medication Key ___ * Attached Patient numbers to be continually audited and reported by Acute Trust Final achievement of target medical therapy doses to be periodically audited and reported by Acute Trust HFDC referral form Discharge report (example) Uptitration advice form Thank you Any questions?