Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
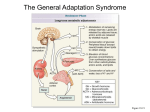
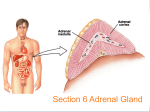
Adrenal cortex hormones Adrenal cortex Glucocorticoid secretion Aldosterone secretion Androgen secretion Adrenocortical hyperfunction Adrenocortical hypofunction Adrenal cortex Adrenal cortex, in fact, synthesizes dozens of different types of steroid molecules, but only a few of them have got biological activity. They have been classified into 3 categories: 1) Glucocorticoids. 2) Mineralocorticoids. 3) Androgens (sex hormones). These hormones initiate their action by combining with specific intracellular receptors, and this complex bind to specific regions of DNA to regulate gene expression. The morphological zonation of the adrenal cortex, showing the three types of cells with their particular structural arrangement. and hormone producing capability. The hypothalamic anterior pituitary–adrenal axis and the fate of cortisol following its release. CBG = cortisolbinding globulin. Glucocorticoid secretion Glucocorticoids have widespread metabolic effects on carbohydrate, fat and protein metabolism. Glucocorticoids are also involved to some extent in regulating sodium and water homeostasis and the inflammatory and stress responses. In the liver, cortisol In the circulation, stimulates gluconeogenesis, glucocorticoids are mainly amino acid uptake and protein bound (∼90%), chiefly to degradation,and ketogenesis. CBG (cortisol-binding globulin or transcortin). Lipolysis is increased in Plasma [CBG] is increased in adipose tissue, and pregnancy and with oestrogen proteolysis and amino acid treatment (e.g. oral contraceptives). release promoted in muscle. ACTH is the main stimulus to cortisol secretion. 3 factors regulate ACTH (and therefore cortisol) secretion: • Negative feedback control. • Stress. (e.g. major surgery, emotional stress) leads to a sudden large increase in CRH (and ACTH) secretion. • The diurnal rhythm of plasma [cortisol]: Patients with Cushing’s syndrome lose this diurnal variation. Aldosterone secretion The principal physiological function of aldosterone is to conserve Na+, mainly by facilitating Na+ reabsorption and reciprocal K+ or H+ secretion in the distal renal tubule and in other epithelial cells. Although its rate of production is less than 1% of the rate of cortisol production, aldosterone is a major regulator of water and electrolyte balance, as well as blood pressure. The renin–angiotensin system is the most important system controlling aldosterone secretion. The renin–angiotensin system Renin is released from the renal juxtaglomerular cells (JC) in response to hypotension, low blood volume or sodium depletion. Renin catalyses the conversion of angiotensinogen in plasma to angiotensin I. During passage through the lung, angiotensin-converting enzyme (ACE) catalyses the production of angiotensin II from angiotensin I. The angiotensin II stimulates release of aldosterone from the adrenal glomerulosa and the mineralocorticoid then promotes reabsorption of sodium in the distal tubules of the kidney. The renin–angiotensin system is the most important system controlling aldosterone secretion. Renin is a proteolytic enzyme produced by the juxtaglomerular apparatus of the kidney . And released into the circulation in response to a fall in circulating blood volume or renal perfusion pressure, and by loss of Na+ . Renin then acts on angiotensinogen (a 248 amino acid peptide produced by the liver) in plasma to produce angiotensin I (AI), a decapeptide which is then converted by ACE in the lung to the octapeptide angiotensin II (AII). AI and particularly AII stimulate aldosterone production in the adrenal glomerulosa. Androgen secretion The most potent androgen is testosterone, but the ones, dehydroepiandrosterone (DHEA) and dehydroepiandrosterone sulphate (DHEAS) are converted by peripheral tissues into testosterone. The measurements of these androgens are important in the investigation of hirsutism and virilism and CAH ( Congenital adrenal hyperplasia). The pathways for the production of the various adrenal steroids are shown below. Adrenocortical hyperfunction Cushing’s syndrome. This can be ACTH dependent or ACTH independent then the condition is caused by tumours that release either ACTH or cortisol. Approximately 70% of cases are due to a pituitary adenoma secreting ACTH (this is known as Cushing’s disease). Ectopic ACTH secretion (often from a small-cell carcinoma of the bronchus or a carcinoid tumour) is the cause of approximately 10% of the cases. Glucocorticoid- secreting adrenal adenoma or carcinoma are each responsible for about 10% of the cases. Adrenocortical hypofunction (Addison’s disease) Adrenocortical insufficiency may be primary (e.g. destruction of the gland itself by tuberculosis or autoimmune disease) or secondary (e.g. hypothalamic or pituitary disease leading to ACTH deficiency or after long-term steroid therapy). In primary adrenal failure, patients present with lethargy, weakness, nausea and weight loss. They are typically hypotensive, with characteristic hyperpigmentation affecting the buccal mucosa, scars and skin creases. Patients with primary adrenal failure usually have deficiencies of both glucocorticoids and mineralocorticoids. Often there is hypoglycaemia with hyponatraemia, hyperkalaemia, raised serum urea levels and acid–base disturbance.