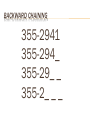
Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
MULTIPLE SCLEROSIS AND NEUROPSYCHOLOGICAL FUNCTIONING: MANAGING COGNITIVE DEFICITS Dr. Lesley Ritchie, C.Psych. Ms. Jodie Gawryluk, B.A. Department of Clinical Health Psychology University of Manitoba OVERVIEW 1. 2. 3. 4. 5. 6. 7. Introduction to the brain Understanding MS The treatment team What is neuropsychology? Neuropsychological assessment Cognitive domains Neuropsychological profile of MS Managing neuropsychological deficits Specific strategies Special considerations OVERVIEW 1. 2. 3. 4. 5. 6. 7. Introduction to the brain Understanding MS The treatment team What is neuropsychology? Neuropsychological assessment Cognitive domains Neuropsychological profile of MS Managing neuropsychological deficits Specific strategies Special considerations INTRODUCTION TO THE BRAIN The brain monitors and controls nearly everything that we do from our breathing and heart beats to our senses (e.g., vision, hearing), to our movements, speech, and personality INTRODUCTION TO THE BRAIN • The brain is divided into left and right cerebral hemispheres Left Hemisphere is important for: • language (thinks in words) • math • logical abilities • movement of the right side of the body Right Hemisphere is important for: • visual information (thinks in pictures) • organization • creativity • movement of the left side of the body INTRODUCTION TO THE BRAIN Frontal Lobes • Movement • Speaking • Planning • Organizing • Reasoning • Decision making • Judgment • Personality INTRODUCTION TO THE BRAIN Temporal Lobes • Memory • Recognition Hearing • Understanding Language • Emotions INTRODUCTION TO THE BRAIN Parietal Lobes • Sensations • Reading and Writing • Ability to use Numbers • Spatial Reasoning • Perception Occipital Lobes • Seeing objects • Locating objects in space • Recognizing the things we see INTRODUCTION TO THE BRAIN Cerebellum • Maintaining balance • Coordination of movement • Timing of movement INTRODUCTION TO THE BRAIN Brain Stem • Connection between brain and body • Breathing • Blood pressure • Swallowing • Appetite • Body temperature • Digestion • Sleeping INTRODUCTION TO THE BRAIN Brain Anatomy The brain is made up of two types of tissue: Grey matter (where information is processed) White matter (the highways that take information to the processing stations) White matter Grey matter INTRODUCTION TO THE BRAIN Functional Analogy OVERVIEW 1. 2. 3. 4. 5. 6. 7. Introduction to the brain Understanding MS The treatment team What is neuropsychology? Neuropsychological assessment Cognitive domains Neuropsychological profile of MS Managing neuropsychological deficits Specific strategies Special considerations MULTIPLE SCLEROSIS Multiple = more than one Sclerosis = area of stiffening/damage Autoimmune disorder Immune system attacks the CNS Demyelination White matter tissue is white because of myelin, a fatty covering that helps information travel to brain areas quickly MULTIPLE SCLEROSIS Symptom onset btwn 20 – 40 years of age 2-3x more common in women Increased prevalence in northern latitudes MULTIPLE SCLEROSIS Affects brain and spinal cord Altered motor, sensory, and cognitive functioning Common presenting symptoms Symptoms vary according to disease course (Olek 2005) Symptom Frequency (%) Sensory disturbance - limbs 30.7 Visual loss 15.9 Motor disturbance (subacute) 8.9 Diplopia 6.8 Gait disturbance 4.8 Motor (acute) 4.3 Balance problems 2.9 Sensory disturbance (face) 2.8 MULTIPLE SCLEROSIS Disease course 1. Relapsing and remitting MS (RRMS): – – 2. Secondary progressive MS (SPMS): – 3. 80% with initial RRMS show declines between attacks w/o periods of remission; most common Primary progressive MS (PPMS): – – – 4. Clearly defined attacks and periods of remission Triggers: warm weather, infections, stress 10% who do not have period of remission following 1st attack Continuous decline Older at onset Progressive relapsing MS (PRMS): – steady decline with attacks Bobholz & Gremley (2011) OVERVIEW 1. 2. 3. 4. 5. 6. 7. Introduction to the brain Understanding MS The treatment team What is neuropsychology? Neuropsychological assessment Cognitive domains Neuropsychological profile of MS Managing neuropsychological deficits Specific strategies Special considerations TREATMENT TEAM GP: manages all medical concerns Neurologist: manages concerns about MS or other brain conditions Radiologist: collects images of the brain Neuropsychologist OVERVIEW 1. 2. 3. 4. 5. 6. 7. Introduction to the brain Understanding MS The treatment team What is neuropsychology? Neuropsychological assessment Cognitive domains Neuropsychological profile of MS Managing neuropsychological deficits Specific strategies Special considerations CLINICAL NEUROPSYCHOLOGY … is an applied science concerned with the behavioural expression of brain dysfunction (Lezak, 1995) Normal Distribution - Test Interpretation Average AVERAGE Low average Low Ave Borderline Impaired 2.14% 13.59% 0.13% 0.13% Z -3 -2 -1 34.13% 34.13% 13.59% X 0 High Ave High average 1 2 Superior 2.14% 3 V. Superior 0.13% Normal Distribution - Test Interpretation Average AVERAGE Low average Low Ave Borderline Impaired 2.14% 13.59% 0.13% 0.13% Z -3 -2 -1 34.13% 34.13% 13.59% XX 0 High Ave High average 1 2 Superior 2.14% 3 V. Superior 0.13% Normal Distribution - Test Interpretation Average AVERAGE Low average Low Ave Borderline Impaired 2.14% 13.59% 0.13% 0.13% Z -3 -2 -1 34.13% 34.13% 13.59% XX 0 High Ave High average 1 2 Superior 2.14% X 3 V. Superior 0.13% CLINICAL NEUROPSYCHOLOGY What neural mechanisms underlie various cognitive abilities and different emotional states? How do these mechanisms work ? What are the effects of brain damage on behaviour ? Application of appropriate intervention strategies OVERVIEW 1. 2. 3. 4. 5. 6. 7. Introduction to the brain Understanding MS The treatment team What is neuropsychology? Neuropsychological assessment Cognitive domains Neuropsychological profile of MS Managing neuropsychological deficits Specific strategies Special considerations CLINICAL NEUROPSYCHOLOGY Neuropsychological Assessment Specific nature of the injury Pre-injury history strengths / weaknesses Specific situation demands of life / work Supports available Personality factors Emotional response to injury & limitations Adaptive & coping skills Beliefs / expectations of client & family Psychometrics CLINICAL NEUROPSYCHOLOGY All neuropsychological tests are developed through research Administered in a standardized manner Results are compared to normative data CLINICAL NEUROPSYCHOLOGY Cognitive domains Estimated premorbid ability General Intellectual ability Attention Speed of information processing Sensory – motor function Language Visual Perception & Construction Executive functions Memory Mood / Psychopathology / Personality Validity & Effort OVERVIEW 1. 2. 3. 4. 5. 6. 7. Introduction to the brain Understanding MS The treatment team What is neuropsychology? Neuropsychological assessment Cognitive domains Neuropsychological profile of MS Managing neuropsychological deficits Specific strategies Special considerations NEUROPSYCHOLOGICAL PROFILE OF MS 45-65% of people with MS have cognitive symptoms 80% of those are mildly affected Even mild problems can interfere with everyday activities Cognitive deficits increase with prolonged disease duration 20-30% of patients develop more severe impairments, such as dementia Cognitive deficits don’t tend to fluctuate Greater deficits associated with Progressive disease courses (PPMS, SPMS) Duration of disease Increased prevalence of cognitive decline in men Quantity of MR abnormalities COGNITIVE IMPAIRMENT IN MS Processing speed Attention/concentration Sustained Complex Abstract reasoning Problem-solving Language Verbal fluency Naming Memory (40-60%) Episodic/recent memory Working memory Executive functioning (EF) Visuospatial skills Table 20.3; Bobholz & Gremley (2011) PROCESSING SPEED Speed of mental activity Most common Underlying factor Memory Working memory http://www.mountsinai.on.ca/ care/ebffrc/ms ATTENTION Attention = vigilance, capacity for information, switching attention, selective attention 20-25% of MS patients Deficits in rapid and complex info processing Working memory Attentional switching Rapid visual scanning Intact attention span INFORMATION ABOUT ATTENTION Focused Attention is the ability to focus on something in the moment. For example, focused attention can be for things you see, such as watching television or for things you hear, such as listening to the radio. INFORMATION ABOUT ATTENTION Sustained Attention allows you to focus on something over a long period of time For example, watching a movie or reading a book. INFORMATION ABOUT ATTENTION Selecting Attention allows you to pick out important information from unimportant or distracting information For example, listening to a conversation in a noisy cafeteria. INFORMATION ABOUT ATTENTION Shifting Attention allows you to switch back and forth between two different tasks. For example, when you are cooking you may need to shift your attention back and forth between watching for a pot boil and preparing vegetables to put in the pot. INFORMATION ABOUT ATTENTION TYPES OF ATTENTION Divided Attention allows you to work on two different tasks at the same time, and is sometimes referred to as multi-tasking. For example, singing along to the radio while driving home. INFORMATION ABOUT ATTENTION Symptoms of Attention Difficulties • Becoming easily distracted • Having trouble keeping track of what is being said and done or have trouble making sense of things • Having trouble focusing on one person, thing or conversation in crowded environments • Having trouble keeping track of more than one thing at a time • Having difficulty doing more than one task at a time • Having difficulty learning and remembering information • Becoming easily frustrated with yourself and others • Feeling confused and overwhelmed • Avoiding contact with care givers, friends and family MEMORY Ability to learn and recall information about previous experiences. E.g., favorite song and the look of our home Different types of memory are stored in different places in the brain. Verbal information (such as words) are typically stored on the left side of the brain Visual information (such as pictures) are typically stored on the right side of the brain FACTS ABOUT MEMORY TYPES OF MEMORY Different types of memory based on time. Short term memory, Working memory, Recent memory, and Long term memory FACTS ABOUT MEMORY SHORT TERM MEMORY •This is the ability to remember something in the moment or that you only need to remember for a few minutes •Remembering a phone number you have just been told •Short term memory is often impaired after a brain injury FACTS ABOUT MEMORY WORKING MEMORY • This is the ability to remember in the moment or for a few minutes while you focus on something else or are distracted • An example is keeping a phone number in mind while looking for a pen and paper to write it down. • Working memory is often affected by brain injury FACTS ABOUT MEMORY HOW ARE MEMORIES MADE? 1. Attention You must pay attention to what you are learning 2. Recording Your brain needs to 'take in' and record information The 3 R’s of Memory 3. Retain The information needs to be stored in the right spot 4. Retrieve Information needs to be recalled when it is needed again If problems occur anywhere in these steps, then memory difficulties will occur EXECUTIVE FUNCTIONING Cognitive abilities required to complete goal-directed behaviors that are not automatic, overlearned, or routine (Sohlberg & Mateer, 2001). EXECUTIVE FUNCTIONING Initiation Inhibition Set-switching Judgment/Reasoning Goal identification Working memory Speed of processing Cognitive flexibility/problemsolving Sequential processing Planning Self-Monitoring Perseveration Prioritizing Multi-tasking Emotional control Insight/Awareness EXECUTIVE FUNCTIONING 15-20% of patients with MS exhibit executive dysfunction Impaired goal-directed behavior Verbal disinhibition Poor self-monitoring (e.g., tangential speech) Reduced insight Deficits in planning and prioritizing Problems with abstraction and conceptualization LANGUAGE AND VISUOSPATIAL Language Mild confrontation naming deficits Speech abnormalities (dysarthria, hypophonia) Poor verbal fluency (retrieval deficit/speed) 20-25% Visuospatial Angle matching Face recognition impact of changes in vision/diplopia Visual miscalculations OVERVIEW 1. 2. 3. 4. 5. 6. 7. Introduction to the brain Understanding MS The treatment team What is neuropsychology? Neuropsychological assessment Cognitive domains Neuropsychological profile of MS Managing neuropsychological deficits Specific strategies Special considerations MANAGING NEUROPSYCHOLOGICAL DEFICITS MANAGING NEUROPSYCHOLOGICAL DEFICITS Neuropsychological rehabilitation Interventions aiming to enhance or support cognitive abilities following brain injury, with an emphasis on achieving functional changes (Sohlberg & Mateer, 2001) Target: reductions in cognitive, emotional, psychological functioning that encumber everyday functioning Goal: increase independent functioning by means of enhanced knowledge and skill, behavior change, or implementation of compensatory strategies MANAGING NEUROPSYCHOLOGICAL DEFICITS Foundation of cognitive intervention Tx based on current level of function Build on strengths to support weaknesses Collaborative Goal-oriented Education SPECIFIC STRATEGIES Processing speed Attention Memory Executive functioning Language PROCESSING SPEED Complete one activity at a time Schedule more time to complete tasks Limit distractions Record information for later review SPECIFIC STRATEGIES Processing speed Attention Memory Executive functioning Language ATTENTION Orienting procedures “What am I doing?” Minimizes gaps in attention Pacing Realistic expectations Elongated performance times Minimize frustration Vary according to time of day Schedule adequate rest ATTENTION Environmental modification Work in a quiet environment Reduce clutter Limit distractions Refer to checklists to complete tasks Set timers to prevent going overtime Work on one task at a time Double/triple check work to minimize errors Have a significant other check work ATTENTION Top Ten tips to help you manage attention difficulties: Practice Check in Modify your environment Pace yourself. Take care of yourself. Monitor your mood. Double check Break tasks down Do difficult tasks at your best time of day. Use your family and friends for support. Take care of yourself. Fatigue, hunger, and/or thirst all adversely affect your attention. Taking care of yourself will help maintain optimum attention. SPECIFIC STRATEGIES Processing speed Attention Memory Executive functioning Language MEMORY Repetition - Repeat the information over and over and over again. •Looking at something one time is never enough. •For example, if you are trying to learn someone’s name, repeating it over and over to yourself can help you remember it. MEMORY Multimodal learning – It helps to learn the same information in different ways. For example, to learn a new recipe, it helps to read over the steps in the recipe, listen to someone telling you the steps, and practice the recipe by doing it. See it, hear it, do it! MEMORY Break it down - Break up what you want to remember into smaller steps. If you have something really tough to learn, try to break it down into small bits and then learn one bit at a time. MEMORY Write it down - When something is important to remember, write it down, and keep it in a safe place. Remember to check your notes regularly. Writing information down also allows for repeated exposure to the information (Hear, Write, Read – 3x exposure) • Calendar • Daytimer • PDA or cell phone • Notebook MEMORY Learn it right the first time - New skills are easier to remember if you learn them the right way (mistakes are hard to correct later) Helpful Hints for Errorless Learning 1. Break the task down into smaller steps. 2. Learn each step at a time and avoid making errors that may confuse you later . 3. Complete the task you are trying to learn together with someone who has done it before. Ask this person to talk through the steps as you learn the task (this will help you to avoid errors) 4. Use hints that will help you remember the steps (you can ask someone for hints or make up notes for yourself that guide you to the next step) 5. Only try to do the new skill when you are sure you know the steps and can do it error-free MEMORY Elaboration – This is a technique that you can use to make information more meaningful and easier to remember. Information can be easier to remember if you think through all of the details. Here are some questions to help you elaborate: Can you link this with anything or anyone you know? Do you link this with any feelings? Is there anything about it that is unique or special? Can you link this with things in your daily life? How does it look? How does it feel? How does it sound? How does it smell? How does it taste? MEMORY Space out your attempts to retrieve information - Try to recall new information several times in a row. If you can recall it correctly, then gradually increase the time (from minutes to hours) between attempts. For example, recall information the first time after 20 seconds, then space out your attempts to recall – 30 sec, 1 minute, 5 minutes, 10 minutes, 30 minutes, 1 hour, 4 hours, later that day, and the next day. Set up a Routine - Follow a daily or weekly routine to help you remember events and times to get regular tasks done each day. SPACED RETRIEVAL Brooke Smith BACKWARD CHAINING 355-2941 355-294_ 355-29_ _ 355-2_ _ _ WHO IS THIS? MEMORY External Aides (portable memory) • Labels on the outside of boxes, drawers, and cupboards to help you find things. • Post-it notes to leave yourself reminders in places around your home. • A notepad beside the phone to write down messages and reminders • Checklists or shopping lists. • Diary for storing and planning • Alarm clock, or timer to help you remember when you are supposed to do something • A calendar to keep track of appointments • A tape recorder to leave messages for yourself • A pill reminder box to keep track of medications MEMORY Get Organized – It is easier to remember where things are if they are kept in one place. For example, if you are constantly losing your wallet, you will find it faster if you always leave it in the same spot. Make A 'To Do' List – Making a list of things that you need to do can help you remember all that you need to get done. For example, you can make a list of chores to remind yourself of what needs to be done. MEMORY Mnemonics Consciously leaned Require considerable effort Verbal or visual Richard of York gives battle in vain Red, orange, yellow, green, blue, indigo, violet My very elderly mother just sat upon a new pin Mercury, Venus, Earth, Mars, Jupiter, Saturn, Uranus, Neptune, Pluto SPECIFIC STRATEGIES Processing speed Attention Memory Executive functioning Language EXECUTIVE FUNCTIONING Structure and Routine! Do things that require the most initiation in the morning or after a rest Set a small number of goals for each day Set up (with assistance) organizational practices Large family calendar Online bill payment Use labels Schedules Simplify activities Prioritize Checklists EXECUTIVE FUNCTIONING Meta-cognitive strategies To regulate behavior and increase goaloriented behavior Self-talk Tracking behaviors Self-monitoring Tracking errors and attention lapses Goal Management Training GOAL MANAGEMENT TRAINING Maintaining intentions in goal-directed behavior is reliant on intact executive functioning GMT based on theory of goal neglect resulting in disorganized behavior following frontal lobe injury Levine et al. (2000). SPECIFIC STRATEGIES Processing speed Attention Memory Executive functioning Language LANGUAGE Language Communication skills training Group interventions Modeling and generalization Building social networks In MS, many language deficits are due to physical changes (i.e., dysphagia) and reduced speed of processing. Allow more time for communication CAVEAT Neuropsychological interventions should be person-specific Different presentations Attention Processes Selective Attention Executive Processes Memory Processes Working Memory Divided Attention Prospective Memory Alternating Attention Awareness Task Performance Solberg & Mateer (2001), Figure 8.3 SPECIAL CONSIDERATIONS Common symptoms of MS Emotional and psychological difficulties Depression Fatigue Pain EMOTIONAL DIFFICULTIES Can impact neuropsychological functioning Healthy Brain 25% 50% 25% Nurse Cells Life Support Cognitive EMOTIONAL DIFFICULTIES Brain Injury 17% 25% 33% 25% Nurse Cells Cognitive Life Support Brain Injury EMOTIONAL DIFFICULTIES Brain Injury + Stress/Anxiety 11% 25% 17% 25% 22% Nurse Cells Brain Injury Life Support Stress/Anxiety Cognitive DEPRESSION Patients with MS have a 50% lifetime risk for depression Higher prevalence than the general population and higher than in other brain disorders Depression is treatable! Prevalence of anxiety is 25% - usually associated with diagnostic uncertainty and decreases over time DEPRESSION Common Symptoms Feelings of helplessness and hopelessness Loss of interest in daily activities. Appetite or weight changes Sleep changes Psychomotor agitation or retardation Loss of energy Self-loathing Concentration problems DEPRESSION Self-management strategies Schedule in activities each day Make plans to see supportive friends/family Consider joining a support group Try a new hobby Try activities that make you think (this will help with your recovery too!) Stay away from drugs/alcohol Exercise (e.g., go for a short walk) Referral to a Clinical Psychologist Psychotherapy DEPRESSION RISK OF SUICIDE When feelings of depression are severe, it is important for family members/friends to be aware of suicide risk. If your family member/friend talks about wanting to end their life or makes statements such as "It would have been better if I had died" he/she may be thinking about suicide. It is important not to ignore these comments and to contact a member of the healthcare team immediately. For support from the mental health crisis team (available 24 hours a day all week) Call 1-877-435-7170 (MANITOBA SUICIDE LINE) FATIGUE Why does MS cause fatigue? The brain has to work harder to do the same activities it did before. Because the brain has to work so hard, it can become tired more quickly. The brain may be trying to heal as you recover from a relapse and this takes more energy than usual, which can lead to fatigue. MS can lead to problems with sleeping, which can leave you feeling exhausted. FATIGUE When you have fatigue, you may feel suddenly exhausted and lack the energy to do basic tasks. Mental Fatigue Increased forgetfulness Lack of motivation to plan your day Lack of interest in things you enjoy Withdrawal Slower speech Giving short answers in a quiet/dull voice Increased irritability or anxiety Slurred speech Difficulty finding words Poor concentration Physical Fatigue Shortness of breath Slower movement Withdrawal Cramps or weak muscles Poor coordination or balance Falls Poor vision FATIGUE It can help to figure out what triggers your fatigue, and how long it takes you to become fatigued. Keeping track of these factors can help you tailor coping strategies to suit you best. Once you know how fatigue affects you, there are a number of strategies that can be used to help you manage the fatigue that so often results from a brain injury. What makes fatigue worse? • Doing too many things. • Not taking breaks during the day. • Stress • Illness • Too little exercise. • Poor nutrition, such as eating junk food. • Alcohol and caffeine • Feeling depressed or anxious. • Poor sleep. FATIGUE What are some strategies that can make fatigue better? 1. Following a Routine 2. Environmental aids 3. Timing of activities 4. Pace Yourself 5. Sleep 6. Eat properly 7. Exercise your body 8. Exercise your mind 9. Plan ahead 10.Seek support How to cope with Fatigue When should you ask for help? Talk with someone on your health care team if….. You are having trouble using strategies to cope with fatigue Your fatigue gets worse over time You are too fatigued to get out of bed during the day You have trouble sleeping and aren't functioning properly You feel sadness and lack of motivation along with fatigue You are having trouble taking care of yourself Your ability to think through daily activities is affected by fatigue PAIN Like emotional difficulties, pain can negatively impact cognitive functioning by: Stealing one’s attention/focus Reducing processing speed Attention and processing speed deficits can negatively impact memory Exacerbating psychological and emotional difficulties PAIN Coping strategies Psychotherapy Relaxation strategies Abdominal breathing Imagery Progressive muscle relaxation Cognitive restructuring Behavior management Planning Prioritizing Pacing Learning how to communicate about pain FINAL CONSIDERATIONS Potential obstacles to successful interventions Diminished insight Poor engagement/motivation to change Significantly compromised cognitive functioning Poor generalization Sohlberg & Mateer (2001) FINAL CONSIDERATIONS - Solutions Include significant others Build generalization into the treatment program. - Collaborative relationship with the patient and family - Homework - Real world examples - Work with patient to identify barriers to complete homework - Over-learning - Relapse planning and management Sohlberg & Mateer (2001)