Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Herpes simplex virus wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Rocky Mountain spotted fever wikipedia , lookup
Plasmodium falciparum wikipedia , lookup
Cryptosporidiosis wikipedia , lookup
Gastroenteritis wikipedia , lookup
Onchocerciasis wikipedia , lookup
Leptospirosis wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Hepatitis C wikipedia , lookup
Marburg virus disease wikipedia , lookup
Trichinosis wikipedia , lookup
Antibiotics wikipedia , lookup
Staphylococcus aureus wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Hepatitis B wikipedia , lookup
Schistosomiasis wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
Neisseria meningitidis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Mycoplasma pneumoniae wikipedia , lookup
Candidiasis wikipedia , lookup
Lymphocytic choriomeningitis wikipedia , lookup
Anaerobic infection wikipedia , lookup
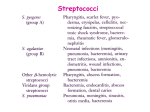
Streptococci Morphology and Identification Gram-positive cocci arranged in chains or pairs. Most group A, B, and C strains produce capsules. Most strains grow as discoid colonies, 1-2 mm in diameter. Catalase-negative. Grow better in media enriched with blood or tissue fluid. Most are facultative anaerobic and some are capnophilic. For most species growth and hemolysis are aided by incubation in 10% CO2. Classification Hemolysis a-hemolysis: incomplete lysis of RBC with the formation of green pigment. b-hemolysis: complete hemolysis No hemolysis Lancefield classification: a serologic classification (A to V) Biochemical reactions are used for species that can not be classified into the Lancefield classification (nongroupable), e.g. viridans streptococci. Antigenic Structure Capsule: antiphagocytosis. The capsule of group A streptococci is composed of hyaluronic acid. The group B streptococci contain type-specific capsular polysaccharides. Group-specific cell wall antigens (Lancefield groups A-V) Carbohydrates Specificity is determined by a dimer of N-acetylglucosamine and rhamnose. M protein T protein: type-specific; function unknown. M-like proteins: binds IgM, IgG and a2-macroglobulin; interfere with phagocytosis. Lipoteichoic acid: binds to epithelial cells. F protein: a major adhesin of S. pyogenes, binding with fibronectin. Pathogenesis Pathogenesis of group A streptococci Adherence to the epithelial cells; >10 adhesion molecules invasion into the epithelial cells; mediated by M protein and F protein important for persistent infections and invasion into deep tissues avoiding opsonization and phagocytosis; M protein, M-like proteins, and C5a peptidase producing enzymes and toxins Enzymes and toxins Streptokinase (fibrinolysin) Can lyse blood clots and may be responsible for the rapid spread of the organism. Used (IV injection) for treatment of pulmonary emboli, coronary artery thrombosis and venous thrombosis. Streptodornase (DNases A to D) Decreases viscosity of DNA suspension. A mixture of this and streptokinase is used in enzymatic debridement-liquifies exudates and facilitates removal of pus and necrotic tissue. Hyaluronidase (spreading factor): Destroys connective tissue and aids in spreading infecting bacteria. C5a peptidase Prevents streptococci from C5a-mediated recruitment and activation of phagocytes, and is important for survival of S. pyogenes in tissue and blood. Streptococcal pyrogenic exotoxins (Spe): Produced by both the scarlet fever strains and new invasive S. pyogenes strains. More than four serologically distinct toxins (SpeA, B, C and F). Biological activities (except SpeB, which is a cysteine protease): Pyrogenicity Cytotoxicity Immunosuppression Superantigen Spe is associated with toxic shock-like syndrome or other invasive S. pyogenes diseases. Hemolysins Streptolysin O: O2-labile; causes hemolysis deep in blood agar plates. ASO (antistreptolysin O) titer >160-200 units suggests recent infection or exaggerated immune response to an earlier respiratory infection. However, skin infection does not induce ASO. Streptolysin S: O2-stable. Causes b-hemolysis on the surface of blood agar plates. Cell-bound, not antigenic. Produced in the presence of serum. Kills phagocytes by releasing the lysosomal contents after engulfment. Epidemiology S. pyogenes can transiently colonize the oropharynx and skin. Diseases are caused by recently acquired strains that can establish an infection of the pharynx or skin. S. pyogenes causes pharyngitis mainly in children of 5 to 15 years old. The pathogen is spread mainly by respiratory droplets. Crowding increases the opportunity for the pathogen to spread, particularly during the winter months. Soft tissue infections are preceded by skin colonization and the organisms are introduced into the superficial or deep tissue through a break in the skin. Clinical Diseases 1. Local infection with S. pyogenes Streptococcal sore throat (pharyngitis), and scarlet fever. Streptococcal pyoderma (impetigo, local infection of superficial layers of skin). Strains that cause skin infections are different from those that cause pharyngitis. 2. Invasion by S. pyogenes Invasion from respiratory tract: otitis media, sinusitis, pneumonia, meningitis, osteomyelitis, and arthritis. Invasion from skin: erysipelas, cellulitis, and necrotizing facitis. Diffuse and rapidly spreading infection that extends along lymphatic pathways with only minimal local suppuration. Sepsis (streptococcal toxic shock syndrome or toxic shock-like syndrome, TSLS): the organism is introduced into the subcutaneous tissue through a break in the skin cellulitis necrotizing faciitis systemic toxicity, multiple organ failure, and death (mortality > 40%). 3. Poststreptococcal diseases (occurs 1-4 weeks after acute S. pyogenes infection, hypersensitivity responses) Rheumatic fever: most commonly preceded by infection of the respiratory tract. Inflammation of heart (pancarditis), joints, blood vessels, and subcutaneous tissue. Results from cross reactivity of anti-M protein Ab and the human heart tissue. This disease can be reactivated by recurrent streptococcal infections, whereas nephritis does not. Acute glomerulonephritis: preceded by infection of the skin (more commonly) or the respiratory tract. Symptoms: edema, hypertension, hematuria, and proteinuria. Initiated by Ag-Ab complexes on the glomerular basement membrane. S. agalactiae (group B, b-hemolytic, contains type-specific capsular polysaccharides which is the most important virulence factor and can induce protective antibodies; may colonize at lower gastrointestinal tract and genitourinary tract) Neonatal sepsis or meningitis Early-onset (during the first week of life): infection acquired in utero or at birth. Pneumonia is common in addition to meningitis. Late-onset (older infants): infection acquired from an exogenous source. (Premature infants are at greater risk.) Infection of pregnant women Urinary tract infections, amnionitis, endometritis, and wound infections Infection in men and nonpregnant women Patients are generally older and have underlying conditions. Bacteremia, pneumonia, bone and joint infections, skin and soft tissue infections. Mortality is higher. Viridans streptococci (a-hemolytic or nonhemolytic, most are nongroupable; except for S. suis, they are divided into 5 subgroups based on the specific diseases they cause) These streptococci colonize the oropharynx, GI tract, and GU tract; rarely on the skin surface. Diseases: Subacute endocarditis (group: Mitis) Intra-abdominal infections (group: Anginosus) Dental caries (group: Mutans) Cariogenicity of S. mutans is related to its ability to synthesize glucan from fermentable carbohydrates as well as to modify glucan in promoting increased adhesiveness. S. pneumoniae Laboratory Diagnosis Smears: useful for soft tissue infections or pyoderma, but not for respiratory infections. Antigen detection tests: commercial kits for rapid detection of group A streptococcal antigen from throat swabs. Detection of group A streptococci by molecular methods: PCR assay for pharyngeal specimens. Culture: Specimens are cultured on blood agar plates in air. 10% CO2 although speeds hemolysis, the growth of inhibitory bacteria is also enhanced. Identification: serological and biochemical tests. Antibody detection ASO titration for respiratory infections. Anti-DNase B and antihyaluronidase titration for skin infections. Antistreptokinase; anti-M type-specific antibodies. Identification of Gram-positive cocci None CAMP test Christie R, Atkins NE, and Munch-Peterson E. 1944. A note on a lytic phenomenon shown by group B streptococci. Aust. J. Exp. Biol. Med. Sci. 22:197-200 Treatment All S. pyogenes are sensitive to penicillin G. Effective doses of penicillin or erythromycin for 10 days can prevent poststreptococcal diseases. Drainage and aggressive surgical debridement must be promptly initiated in patients with serious soft tissue infections. Group B streptococci are also susceptible to penicillin G. Antibiotic sensitivity test is helpful for treatment of bacterial endocarditis. Prevention and Control Most streptococci are normal flora of the human body. Source of S. pyogenes and S. agalactiae is a person harboring these organisms (carrier). Control: 1. Prompt eradication of streptococci from early infections. 2. Prophylactic antibiotic treatment for rheumatic fever patients. 3. Eradication of S. pyogenes from carriers. 4. Dust control, ventilation, air filtration, UV irradiation and aerosol mists are of doubtful efficacy. 5. Intrapartum penicillin to mother at risk of giving birth to an infant with invasive group B disease. S. pneumoniae Morphology and Physiology Gram-positive lancet-shaped diplococci for typical organisms. a-hemolytic (pneumolysin is similar to streptolysin O). Form small round colonies on the plate, at first dome-shaped and later developing a central plateau with an elevated rim. Autolysis is enhanced in bile salt. Growth is enhanced by 5-10% CO2. Capsular polysaccharide: type-specific, 90 types. Smooth (capsular polysaccharideproducing) vs. rough colonies *Quellung reaction (for rapid identification or typing of the bacteria) S. pneumoniae Pathogenesis and Immunity Pneumococci produce disease through their ability to multiply in the tissues (invasiveness). Virulence factors: capsule, cell wall polysaccharide, phosphocholine, pneumolysin, IgA protease, etc. 40-70% of humans are at sometimes carrier of virulent pneumococci. Major host defense mechanisms: ciliated cells of respiratory tract and spleen. The normal respiratory tract has natural resistance to the pneumococcus. Loss of natural resistance may be due to: 1. Abnormalities of the respiratory tract (e.g. viral RT infections). 2. Alcohol or drug intoxication; abnormal circulatory dynamics. 3. Patients undergone renal transplant; chronic renal diseases. 4. Malnutrition, general debility, sickle cell anemia, hyposplenism or splenectomy, nephrosis or complement deficiency. 5. Young children and the elderly. S. pneumoniae Clinical diseases Pneumococcal pneumonia develops when the bacteria multiply rapidly in the alveolar space after aspiration. The affected area is generally localized in the lower lobes of the lungs (lobar pneumonia). Children and the elderly can have a more generalized bronchopneumonia. Resolution occurs when specific anticapsular antibodies develop. Sudden onset with fever, chills and sharp chest pain. Bloody, rusty sputum. Empyema (mostly caused by type 3) is a rare but significant complication. Complications caused by spreading of pneumococci to other organs: sinusitis, middle ear infection, meningitis, endocarditis, septic arthritis. S. pneumoniae Laboratory diagnosis Examination of sputum Stained smears of sputum: a rapid diagnosis. Quellung test with multivalent anticapsular antibodies. Culture Specimen: sputum, aspirates from sinus or middle ear, CSF. cultured on blood agar plate in 5-10% CO2. Identification: bile solubility, optochin sensitivity, etc. for differentiation from other a-hemolytic streptococci. Additional biochemical, serologic or molecular diagnostic tests for a definitive identification. Antigen detection: detect pneumococcal C polysaccharide (teichoic acid; type-specific) in urine or CSF. S. pneumoniae Treatment, Prevention, and Control Penicillins are the drugs of choice. However, strains resistant to penicillin and other antibiotics are common nowadays. Healthy carriers are the source of dissemination. In the development of illness, predisposing factors are more important than exposure to the bacteria. Vaccination of high-risk population (too old, too young, and people losing natural resistance) with vaccines containing multiple capsular polysaccharide types. 7-valent conjugate vaccine for infants <2 years. 23-valent vaccine for older children and adults. Enterococci (E. faecalis, E. faecium) Physiological properties are similar to the streptococci. Form large colonies on blood plate; most are nonhemolytic. Microscopic morphology is similar to S. pneumoniae. Resistant to 6.5% NaCl, 0.1% methyl blue and grow in bile-esculin agar. More resistant to antibiotics than the streptococci. Colonize the large intestine of humans and animals. An opportunist. Enterococci Clinical Diseases One of the leading causes of nosocomial infections. Urinary tract (UTI), peritoneum (peritonitis) and heart tissue (endocarditis- a severe complication) are involved most often. Particularly common in patients with intravascular or urinary catheters, and in hospitalized patients with prolonged broadspectrum antibiotic treatment. Intra-abdominal abscess and wound infections: generally polymicrobial. Many strains are completely resistant to all conventional antibiotics. Vancomycin-resistant strains have been isolated (first reported in England and France in 1987). Laboratory Diagnosis Enterococci can be differentiated by simple biochemical tests (e.g., resistant to optochin and bile, hydrolyze PYR, etc.) Enterococci Treatment, Prevention, and Control Resistance in enterococci to aminoglycosides and vancomycin is mediated by plasmids and can be transferred to other bacteria. Combined antibiotic therapy: an aminoglycoside and a cell-wallactive antibiotic. New antibiotics have been developed for treatment of enterococci resistant to both ampicillin and vancomycin. It is difficult to prevent and control enterococcal infections. Control: careful restriction of antibiotic treatment and appropriate infection-control practices (isolation of infected patients; use of gowns and gloves by anyone in contact of patients.) M protein Forms hair-like projections (fimbriae) from the cell membrane. Major virulence factor of S. pyogenes. Enhances degradation of C3b, and phagocytosis by PMNs is prevented. Promotes adherence to epithelial cells. Induces type-specific protective immunity (>100 serotypes). May be a virulence determinant for rheumatic fever. Back Erysipelas Back High risk population for TSLS: patients with HIV infection, cancer, diabetes mellitus, heart or pulmonary disease, varicella-zoster virus infection, and intravenous drug abusers and alcoholic. Back S. pneumoniae virulence factors Back