Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Oesophagostomum wikipedia , lookup
Sarcocystis wikipedia , lookup
Anaerobic infection wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Hepatitis B wikipedia , lookup
Neonatal infection wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
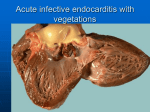
Pneumonia & Other Patterns of Acute Lung Injury Pneumonia • Definition: – Inflammatory consolidation of the lung parenchyma caused by formation of intra-alveolar inflammatory exudate resulting from lung infection • Normal defence mechanisms: – Nasal clearance – Tracheobronchial clearance – Alveolar clearance Predisposing Factors Local Factors • Loss / impairment of cough reflex (e.g. altered consciousness) • Impaired mucociliary elevator (e.g. smoking) • Impaired function of alveolar macrophages (e.g. smoking, alcohol) • Accumulated / stagnant secretions (e.g. CF) • Oedema or congestion Predisposing Factors Impaired Host Resistance • • • • Chronic Disease Malignancy Immune Deficiency Iatrogenic – immunosuppressive Rx Pathogenesis • Inhalation of air droplets • Aspiration of infected secretions or objects • Haematogenous spread Classification • Anatomic distribution • Aetiology (microbiology) • Clinical classification • Nature of host inflammatory reaction Anatomic Classification • Bronchopneumonia – patchy consolidation, usually extension of preexisting bronchitis / bronchiolitis • Lobar (less frequent) – widespread fibrinosuppurative consolidation of a large portion of a lobe or an entire lobe Aetiology • Infectious: – – • Acute Bacterial Pneumonia • • • • NB Streptococcus pneumoniae = pneumococcus (>60%) Staphyllococcus aureus Haemophilius Influenza Legionella pneumophilus • Klebsiella, Pseudomonas, E. coli, Proteus (Hospital-acquired) Viral, Mycobacterial, Fungal, Parasitic (immunocompromised) Aspiration (chemical & bacterial) Nature of Host Response • • • • • Acute fibrinous Granulomatous Organizing Interstitial Eosinophilic Bronchpneumonia • Infection centred on bronchi but extends into alveoli - patchy consolidation – Streptococcus pneumoniae, Haemophilus influenza, Staphylococcus aureus • Successive infection of conductive airways • Infants, debilitated young children, elderly, postoperative – ‘Old man’s friend’ • Widespread patchy areas of inflammation spreading from bronchitis and bronchiolitis • Lower lobes – larger and more numerous foci • Pale, slightly raised areas above the surface of the surrounding lung parenchyma Bronchopneumonia Gross appearance of lung at autopsy scattered, discrete yellowish areas of lung consolidation centred around the bronchioles Acute Pneumonia Alveolar Spaces filled by acute inflammatory cells (neutrophils) Acute Pneumonia Acute Inflammatory cells within alveolar spaces Lobar Pneumonia • Alcoholics • Poor social/medical care • Otherwise healthy adults (20-50 yrs) • Usually Pneumococcus (90%) or Klebsiella • Abrupt onset – Pleuritic chest pain, rusty sputum – High fever, rapid & shallow breathing Classic Stages of Lobar Pneumonia 1. Congestion 2. Red hepatisation 3. Grey hepatisation 4. Resolution • Congestion: – – – – Vascular engorgement Intra-alveolar fluid Small numbers of neutrophils Often numerous bacteria – Gross: heavy and hyperaemic lung • Red hepatisation: – Vascular congestion persists – Extravasation of RBCs into alveolar spaces – Alveolar fibrinosuppurative exudate – Gross: solidification (consolidation) of the lung parenchyma with similar appearance to liver. • Grey hepatisation: – Red cells disintegrate – Persistence of the neutrophils and fibrin. – Gross: The alveoli still appear consolidated, but grossly the color is paler (grey/brown). • Resolution: – Exudate is digested by enzymatic activity, and cleared by macrophages or by cough mechanism. Primary Atypical Pneumonia • Inflammation of alveolar septa & interstitium • Fever, dry cough, dyspnoea but NO CONSOLDATION = atypical • Mycoplasma pneumoniae commonest • Others: viruses (e.g. Influenza virus), Chlamydia & Rickettsia. Gross appearance and mechanism of localisation of aspiration pneumonia in the lung R>L a (a) supine (b) on side b Complications of Pneumonia • • • • • Abscess Formation Organisation (fibrosis) Empyema – suppurative pericarditis Bronchiectasis Bacteraemic dissemination to other organs (metastatic abscesses) – Endocarditis, Meningitis, Peritonitis & Suppurative arthritis N.b. pneumonia is 6th leading cause of death (USA) Lung Abscess • Localized suppurative necrosis – Collection of pus that is walled off by chronic inflammatory / granulation tissue and fibrous tissue • Organisms commonly cultured: – – – – – Staphylococci Streptococci Gram-negative Anaerobes Frequent mixed infections • Pathogenesis: – Preceding pneumonia – Bronchial obstruction – tumour, foreign body, aspiration – Septic embolism Empyema Pus filled pleural cavity is lined by thick granulation tissue (peeled back on left side of photograph). This loculation of pus allows ongoing bacterial proliferation because access of antibiotics is denied. Empyema therefore must be drained before it can heal. Diffuse Alveolar Damage (DAD) • Pathologic manifestation of Adult Respiratory Distress Syndrome (ARDS) / ‘Shock Lung’ – Rapid onset respiratory failure and arterial hypoxaemia refractory to O2 therapy • End result of acute alveolar injury – Caused by a variety of toxic insults • Diffuse = damage to all parts of the alveolus: epithelium, endothelium and interstitium Clinical Syndrome • Acute onset of dyspnoea • Diffuse pulmonary infiltrates • Rapid development of respiratory failure • High mortality (50-60%) Diffuse alveolar damage • Basic lesions: injury to pneumocytes & endothelial cells by: – Oxygen-derived free radicals – Activated neutrophils and macrophages – Loss of surfactant • Etiology: – – – – Infections (viral) Gas inhalation or liquid aspiration Drugs, chemical, radiation Shock, sepsis, trauma, idiopathic Exudative stage • Pathology: – Acute (exudative) stage – Proliferative or organizing stage Proliferative stage Stages of DAD Early / Acute / Exudative Phase: Day 1: Day 3-7: Week 1: Interstitial / alveolar haemorrhage & fibrin Hyaline membranes Type II pneumocyte hyperplasia Interstitial inflammation Late / Organizing / Proliferative Phase: 1-2 weeks: Fibroblast proliferation Organization & fibrosis Treatment & Prognosis • ICU – Continuous positive airway pressure (CPAP) ventilation? • Overall 50-60% mortality • 20% morbidity in survivors