Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
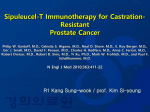
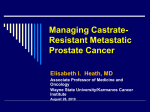
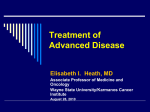
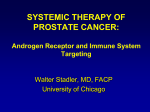
MANAGEMENT OF ADVANCED PROSTATE CANCER Daniel Shevrin, MD Division Hematology/Oncology Northshore University Healthsystem Pritzker School of Medicine University of Chicago ARS 1-G Androgen Ablation Androgen Ablation & Prostate Ca • The androgen receptor is the most important therapeutic target in PCa – Targeting AR is effective in >90% – The AR is critical even in the “hormone refractory” state – Targeting AR is not curative • Androgen ablation has toxicity – Bone, muscle, sex – Toxicity minimal in comparison to other cancer therapies Prostate Ca System Therapy Philosophy • Natural history can be very long – Chronic disease management – Competing mortality/morbidity – Therapy toxicity can have significant functional signficance • Natural history is highly variable – Some patients have rapid disease progression – Disease mortality and morbidity not insignificant • Care is often fragmented – Urologists – Medical oncologists – Primary care ANDROGEN DEPRIVATION THERAPY FOR ADVANCED DISEASE • LHRH agonist + casodex • Degaralix (antagonist) or orchiectomy for immediate drop in testosterone • PSA nadir prognostic • Time to progression varies greatly – Depends on biology: grade, bone vs visceral – Favorable biology: 3 – 5+ years – Unfavorable biology: 1-3 years Intermittent vs. Continuous • Phase II and early phase III data – Intermittent therapy better tolerated and not associated with worse outcome – Fixed on-phase (6-8 months) of ADT – Variable off-phase depends on recovery of testosterone and biologic behavior of cancer – Must monitor T and PSA levels and clinical – Data for less bone density loss – Suggestion of improved sexual function and QOL – Intermittent therapy is a reasonable option for patients requiring androgen deprivation Castrate Resistant Disease • • • • Not really “hormone refractory” Disease actually “hormone hypersensitive” AR still a relevant target Mechanisms of castrate resistance – – – – – AR amplification AR mutation AR modification Ligand availability AR interactions What we know… • Prostate cancer requires AR signaling for development and sustenance. • AR activation is required throughout the natural history of prostate cancer. • AR activation in CRPC occurs via many mechanisms. • Successful blockade of the receptor pathways will confer greater therapeutic control on metastatic prostate cancer. Second-Line Hormonal Agents • Anti-androgen addition – Casodex® – Flutamide® – Nilutamide® • • • • • Anti-androgen withdrawal Ketoconazole 17,20-lyase inhibitors Estrogen Corticosteroids Small and Vogelzang, JCO, 1997 Ketoconazole • Inhibits cytochrome P-450 enzymes – Blocks testicular and adrenal androgenesis • 200 - 400 mg TID – – – – Acid environment improves absorption Expensive Replacement hydrocortisone required 20 mg in morning, 10 mg evening • PSA response rate 40% • Nausea, LFT abnormalities, rash (rare) • Drug interactions – statins, coumadin Abiraterone/TAK-700 NEW INHIBITORS OF ADRENAL ANDROGENS • Abiraterone and TAK700 more potent and selective inhibitors of CYP17lyase • Further inhibition of T levels in blood • Reduction in intra-tumoral T levels • No cortisone requirement • No drug-drug interactions • Nausea, rash, fatigue Castrate Resistant Disease Non-Hormonal Treatment Options • Good prognosis (asymptomatic, “low volume”) – – – – Standard Taxotere® chemotherapy Antiandrogens, ketoconazole Immunotherapy (Provenge, sipuleucel-T) Investigational therapy • Poor prognosis – Standard Taxotere® chemotherapy – Investigational chemotherapy combinations WHAT ABOUT TAXOTERE®? • • • • Treatment improves survival (22 vs 18 months) Treatment improves symptoms Treatment usually decreases PSA Side-effects are manageable – Low WBC, anemia – Hair loss, fatigue, neuropathy • Infusion q 3 weeks for 6-10 cycles • Necessary if disease is aggressive and symptomatic Sipuleucel-T: Autologous APCs Cultured with Antigen Fusion Protein Recombinant Prostatic Acid Phosphatase (PAP) fusion antigen combines with resting antigen presenting cell (APC) APC takes up the antigen Antigen is processed and presented on surface of the APC Fully activated, the APC is now sipuleucel-T INFUSE PATIENT Inactive T-cell Active T-cell T-cells proliferate and attack cancer cells sipuleucel-T activates T-cells in the body The precise mechanism of sipuleucel-T in prostate cancer has not been established. 17 Sipuleucel-T: Logistics of Therapy Day 1 Leukapheresis Apheresis Center Day 2-3 sipuleucel-T is manufactured Central Processing Day 3-4 Patient is infused Doctor’s Office COMPLETE COURSE OF THERAPY: Weeks 0, 2, 4 18 Randomized Phase 3 IMPACT Trial (IMmunotherapy Prostate AdenoCarcinoma Treatment) Asymptomatic or Minimally Symptomatic Metastatic Castration Resistant Prostate Cancer (N=512) Sipuleucel-T Q 2 weeks x 3 2:1 Placebo Q 2 weeks x 3 P R O G R E S S I O N Treated at Physician Discretion S U R V I V A L Treated at Physician Discretion and/or Salvage Protocol Primary Endpoint: Overall Survival Secondary Endpoint: Objective Disease Progression 19 IMPACT Overall Survival Final Analysis (349 events) 36.5 mo median f/u HR = 0.759 (95% CI: 0.606, 0.951) p = 0.017 (Cox model) Sipuleucel-T (n = 341) Median Survival: 25.8 mo. 36 mo. survival: 32.1% Placebo (n = 171) Median Survival: 21.7 mo. 36 mo. survival: 23.0% No. at Risk Sipuleucel-T 341 274 142 56 18 3 Placebo 171 123 59 22 5 2 20 Adverse Events More Commonly1 Reported in Sipuleucel-T Group Sipuleucel-T N = 338 % Placebo N = 168 % Chills 54.1 12.5 Pyrexia 29.3 13.7 Headache Influenza-Like Illness Myalgia Hypertension Hyperhidrosis Groin Pain 16.0 9.8 9.8 7.4 5.3 5.0 4.8 3.6 4.8 3.0 0.6 2.4 Preferred Term 1 Reported by ≥ 5% of sipuleucel-T patients and having a ≥ 2-fold difference from placebo. The majority of the most common AEs were mild or moderate in severity. Safety results obtained from primary analysis did not substantively change with additional data obtained after study closure. 21 Challenges • Why no effect on prostate cancer progression? – – – • Ability to measure disease progression limited Effect on tumor growth “takes time” Minimal effect on PSA or symptoms Cost – • $93,000 not include all apheresis and infusion costs Logistics – – Limited apheresis capacity Limited processing capacity IS THERE ANYTHING AFTER TAXOTERE®? • Cabazitaxel (Jevtana®) – – – – – – – – A novel drug designed for Tax resistance TROPIC study: Jevtana vs Mitoxantrone Infusion every 3 weeks for ~ 6 cycles Improvement in survival (15.1 vs 12.7 months) Much greater decrease in PSA Neutropenia (low WBC) most frequent serious side-effect FDA-approved An important new weapon for advanced prostate cancer Conclusions • Advanced prostate cancer pts can have a long history – Opportunity for multiple therapies – Toxicities and quality of life important – Issues of co-morbid disease and aging • • • • • Philosophy of chronic disease management Androgen receptor pathway targeting is key DNA targeted chemotherapy plays a role Immunotherapy may play a role New therapies need to be identified MANAGEMENT OF ADVANCED PROSTATE CANCER Daniel Shevrin, MD Division Hematology/Oncology Northshore University Healthsystem Pritzker School of Medicine University of Chicago