Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
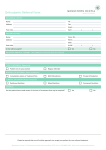
Oxford Inherited Eye Disease Referral Proforma for NGS Panel Testing 1. Patient Details: Forename: DOB: Address: Surname: NHS No.: Your Ref: Post Code: CLINICAL DETAILS DIAGNOSIS: Confirmed by EDTS (please circle) : Yes No Age at onset: Syndromic features (please tick) Hearing Loss Cardiac Neurological Skeletal Endocrine Dermatological Learning Difficulties Other (please specify) Location of Disease (optional) FAMILY HISTORY DETAILS Family History (please tick) Simplex Dominant X-linked Recessive Mitochondrial Male to male transmission Reduced penetrance Consanguinity Oxford Inherited Eye Disease NGS Referral Proforma v.1. (19/06/2015) Family Pedigree 2. Test Request Details: (please tick) Panel 1 – RP and RP-like phenotypes Panel 2 – Syndromic retinal dystrophies Panel 3 – Macular phenotypes Panel 4 – Non-progressive conditions Panel 5 – Stationary congenital night blindness Panel 6 – Optic nerve disease Panel 6+ – Optic nerve disease plus LHON mtDNA Mutations 3. Referral Details: Referrer Details 1 Name: Designation: (please tick) Ophthalmologist Address for report: Clinical Geneticist Genetic Counsellor Post code: Address for invoice: Post code: Referrer Details 2 Name: Designation: (please tick) Ophthalmologist Address for report: Clinical Geneticist Genetic Counsellor Post code: Address for invoice: Post code: In submitting this sample the clinician confirms that genetic counselling has been undertaken and consent for testing has been obtained. Signature: Name: Please send DNA (1µg) or EDTA blood (5mls) to: Oxford Regional Genetics Laboratories Churchill Hospital Old Road Headington Oxford OX3 7LJ Oxford Inherited Eye Disease NGS Referral Proforma v.1. (19/06/2015) Date: