Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
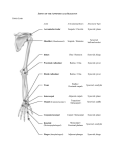
GLENOHUMERAL JOINT (SHOULDER JOINT) Daniel Harris Amanda House Rebecca Miller Ginny Rinaldi Ligaments What is a ligament? • A ligament most commonly refers to a band of tough, fibrous dense regular connective tissue that connects bones to other bones (not bones to muscles) to form a joint. Some ligaments limit the mobility of articulations, or prevent certain movements altogether. • Ligaments gradually lengthen when under tension, and return to their original shape when the tension is removed • The consequence of a broken/overstretched ligament can be instability of the joint. Over time instability of a joint can lead to wear of the cartilage which can eventually lead to osteoarthritis. Acromioclavicular Ligament The acromioclavicular ligament is at the top of the shoulder; it is part of the acromioclavicular joint, which lies between the acromion process and clavicle. The acromioclavicular ligament is divided into superior and inferior parts. This ligament provides horizontal stability to the Acromioclavicular joint. CORACOCLAVICULAR LIGAMENT • The coracoclavicular ligament is the combination of the conoid ligament, and the trapezoid ligament. Together these ligaments provide stabilization for the acromioclavicular joint. They are attached between the coracoid process of the scapula and the underside of the clavicle. SUPERIOR TRANSVERSE SCAPULAR LIGAMENT The superior transverse scapular ligament creates a small foramen from the scapular notch. This ligament is attached by one end to the base of the coracoid process, and by the other to the medial end of the scapular notch. The ligament will sometimes ossify. CORACOHUMERAL LIGAMENT • • • The coracohumeral ligament- a broad ligament which strengthens the upper part of the capsule of the shoulder joint. It arises from the lateral border of the coracoid process, and passes diagonally downward and laterally to the front of the greater tubercle of the humerus. Flexion, Extension TRANSVERSE HUMERAL LIGAMENT The transverse ligament of the humerus consists of a narrow sheet of connective tissue fibers that runs between the lesser and the greater tubercles of the humerus.Together with the intertubercular groove of the humerus, the ligament creates a canal through which the long head of the biceps brachi muscle passes. GLENOHUMERAL LIGAMENTS Three ligaments (seen in blue) on the anterior side of the glenohumeral joint. Together these ligaments reinforce the anterior glenohumeral joint capsule. The superior, middle, and inferior glenohumeral ligaments play different roles in the stability of the head of the humerus depending on arm position and degree of rotation. Abduction, Adduction, External/Internal rotation BURSAE WHAT DO BURSAE DO? • Bursae are flattened sacs made of synovial membrane that are filled with synovial fluid. These sacs function as cushions between your bones and the muscles (deep bursae) or bones and tendons (superficial bursae) • Bursae reduce friction and allow your soft tissue to slide over bone easily during muscle contraction. • The synovial fluid found in bursae comes form synovial cells and are rich in protein and collagen. This acts as the lubricant between areas in your body where friction is greatest. SUBDELTOID & SUBACROMIAL BURSAE Subdeltoid bursa- Located between the deltoid muscle and the shoulder joint cavity and is usually joined to the subacromial bursa. Subacromial bursa- Situated below the acromion process and above the greater tubercle of the humerus lessening the friction when you move your arm or raise it overhead. SUBSCAPULAR & SUBCORACOID BURSAE Subscapular bursa- Located between the joint capsule and the tendon of the subscapularis muscle. The subscapular bursa usually is continuous with the synovial cavity of the joint cavity. Subcoracoid bursa- sits between the coracoid process of the scapula and the shoulder joint capsule. The grey arrow shows subcoracoid bursa BURSITIS When pressure or friction is too great, excess fluid can build up in the bursa sac causing swelling and inflammation. When a bursa becomes inflamed, moving the shoulder becomes very painful and movement can be difficult. Any actions that put pressure on the inflamed bursa can increase irritation and cause further inflammation and pain. If the space becomes too crowded around the subacromial bursa, the acromion can begin to pinch the bursa or tendon causing an impingement (more commonly known as tennis shoulder) when your arm is raised in a forward reaching or overhead position. CARTILAGE • Cartilage serves several functions, including providing a framework upon which bone deposition can begin and also supplying smooth surfaces for the movement of articulating bones. Cartilage is found in many places in the body and is classified as either "hyaline," "elastic," or "fibrous" cartilage. • Cartilage is distinctive in that it has only one cell type, is avascular (lacks blood vessels), aneural (no neurons and nerves), and alymphatic (no lymphatic system). GLENOID LABRIUM • A fibrocartilaginous rim attached around the margin of the glenoid cavity in the shoulder blade. The glenoid fossa (the socket) of the scapula. Without the glenoid labrium only only one third of the head of the humerous would be covered (the ball) Therefore the socket is deepened by the glenoidal labrum. ARTICULAR CARTILAGE The term "articular cartilage" refers to the hyaline cartilage on the articular surfaces of bones. Hyaline cartilage (aka “Gristle") is a type of cartilage found on many joint surfaces. It is pearly bluish in color with firm consistency and considerable collagen. ARTICULAR CAPSULE • An articular capsule (or joint capsule) is an envelope surrounding a synovial joint. Each capsule consists of two layers: A fibrous layer and a synovail membrane. • On the inside of the capsule, articular cartilage covers the end surfaces of the bones that articulate within that joint. • The outer layer is highly innervated by the same nerves which go through through the adjacent muscles associated with the joint. FIBROUS LAYER • An outer layer (fibrous strarum) of the articular capsule composed of avascular white fibrous tissue. SYNOVIAL MEMBRANE • An inner layer (synovial stratum) of the articular capsule which is a secreting layer, and is usually described separately as the synovial membrane. Upper Trapezius Origin Occipital Bone, Nucal Ligament Insertion Outer Third of Clavicle, Acromion Process Action Scapular Elevation and Upward Rotation Middle Trapezius Origin Spinous Processes of C7-T3 Insertion Scapular Spine Action Scapular Retraction Lower Trapezius Origin Insertion Action Spinous Processes of Middle and Lower Thoracic Vertebrae Base of the Scapular Spine Scapular Depression and Upward Rotation Levator Scapulae Origin Transverse Processes of C1-C4 Insertion Vertebral Border of Scapula Between the Superior Angle and Spine Action Scapular Elevation and Downward Rotation Pectoralis Minor Origin: Anterior Surface 3rd-5th Ribs Insertion: Coracoid Process of Scapula Action: With ribs fixed: draws the scapula forward (abducts) and rotates scapula downward against the thoracic wall. With scapula fixed: elevated the rib cage. Serratus Anterior Origin Superior 8 Ribs Laterally Insertion Vertebral Border of Scapula, Anterior Surface Action Scapular Protraction and Upward Rotation Rhomboideus Major Origin Spinous Processes of T2 through T5 Insertion Vertebral Border of Scapula between the Spine and Inferior Angle Action Scapular retraction and Downward Rotation Rhomboideus Minor Origin Spinous Processes of C7 through T1 Insertion Vertebral Border of Scapula at the Spine Process Action Scapular Retraction and Downward Rotation Anterior Deltiod Origin Lateral Third of Clavicle Insertion Deltoid Tuberosity Action Shoulder Flexion, Medial Rotation, Horizontal Adduction Middle Deltoid Origin Acromion Process Insertion Deltoid Tuberosity Action Shoulder Abduction Posterior Deltoid Origin Scapular Spine Insertion Deltoid Tuberosity Action Shoulder Extension, Hyperextensio n, lateral Rotation, Horizontal Abduction Pectoralis Major Origin Insertion Action Medial Third of Clavicle, Sternum, Costal Cartilage of First Six Ribs Lateral Lip of Bicipital Groove of Humerus Shoulder Adduction, Medial Rotation, Horizontal Adduction Latissimus Dorsi Origin Spinous Processes of T7 through L5 (via dorsolumbar fascia), Posterior Surface of Sacrum, Iliac Crest, and Lower Three ribs Insertion Medial Lip of Bicipital Groove of Humerus Action Shoulder Extension, Adduction, Medial Rotation, Hyperextension Teres Major Origin Insertion Action Axillary Border of Scapula near the Inferior Angle Crest Below Lesser Tubercle Next to the Latissimus Dorsi Muscle Attachment Shoulder Extension, Adduction, Medial Rotation Teres Minor Origin Axillary Border of Scapula Insertion Greater Tubercle of Humerus Action Shoulder Lateral Rotation, horizontal abduction Supraspinatous Origin Insertion Action Supraspinous Fossa of the Scapula Greater Tubercle of the Humerus Shoulder Abduction Infraspinatous Origin Infraspinous Fossa of Scapula Insertion Greater Tubercle of Humerus Action Shoulder Lateral Rotation, Horizontal Abduction Subscapulais Origin Insertion Action Subscapular Fossa of the Scapula Lesser Tubercle of the Humerus Shoulder Medial Rotation Coracobrachialis Origin Coracoid Process Insertion Medial Aspect of Humerus Action Weakly Adducts Shoulder Joint Rotator Cuff Muscles S.I.T.S • Supraspinatus • Infraspinatus Teres Minor • Subscapularis Clinical Concerns R.O.M Normal Range of motion for the shoulder: Abduction Adduction Extension Flexion Internal rotation External rotation 180⁰ 45⁰ 45⁰ 90⁰ 55⁰ 40-45⁰ Rotator Cuff Injuries: • Rotator Cuff Conditions • Rotator cuff tear: An injury tears a rotator cuff tendon that’s been weakened by age or wear and tear. Weakness in the arm (and usually pain) are the symptoms. Rotator cuff tendinitis (tendonitis): Repetitive overhead use of the arms (such as painting or throwing) causes a painful strain injury. Rest, ice, and pain relievers are usually effective treatments. Rotator cuff impingement: The tendons of the rotator cuff are squeezed between the humerus and a nearby bone called the acromion. Symptoms and treatment of impingement are similar to tendinitis. Frozen shoulder (adhesive capsulitis): The humerus adheres to the shoulder blade, causing shoulder pain and stiffness. Symptoms usually resolve with time and exercise, or steroid injections. Subacromial bursitis: Inflammation of the small sac of fluid (bursa) that cushions the rotator cuff tendons from a nearby bone (the acromion). • • • • Treatments • • • • • • Pain medicines: Nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, or other medicines can be used to relieve the pain of rotator cuff injuries. Corticosteroid injections: Cortisone or another anti-inflammatory steroid medicine is injected into the shoulder. The reduction in inflammation helps relieve pain. Physical therapy: Various exercises can improve flexibility and strength of the other muscles in the rotator cuff. This increased strength can help compensate for a rotator cuff problem. Occupational therapy: Similar to physical therapy, occupational therapy for rotator cuff injuries focuses on daily tasks that require shoulder movements. Arthroscopic surgery: A surgeon operates through small incisions, using an arthroscope (a tube with a camera and tools on its end). The torn rotator cuff tendon is reattached to the bone. Traditional (open) surgery: Through a larger incision, a surgeon cuts through the muscles and other tissues to reach a torn rotator cuff tendon. The tendon can then be reattached to the bone. VEINS OF THE SHOULDER JOINT • CEPHALIC: The cephalic vein runs up the lateral side of the arm from the hand to the shoulder. In the shoulder, it pierces the tissues and empties into the axillary vein. After the cephalic vein joins the axillary vein, it becomes the subclavian vein and empties into the superior vena cava. • BASILIC: The basilic vein passes along the back of the forearm on the ulnar side for a distance and then curves to the surface below the elbow. It continues to move up the medial side until it reaches the middle of the upper arm. There, it enters deep into the tissues and joins the brachial vein. As the basilic and brachial veins merge, they form the axillary vein. • AXILLARY: The axillary vein is formed where the basilic and brachial veins come together, in the deep tissue of the upper arm. VEINS ARTERIES OF THE SHOULDER JOINT ARTERY MUSCLE Subclavian Transverse Cervical Trapezius: Upper, Middle, Lower Lateral Thoracic Pectoral Major, Serratus Anterior Deep Scapular Lattisimus Dorsi. Rhomboideus: Major and Minor Suprascapular Supraspinatus, Infraspinatus Brachial Coracobrachialis Axillary Pectoralis Minor Dorsal Scapular Levator Scapulae Posterior Circumflex Deltoid: Anterior, Middle and Posterior Circumflex Scapular Teres Major. Teres Minor Subscapular Subscapularis ARTERIES Muscles Nerve Supply ARTERY MUSCLE Subclavian Transverse Cervical Upper, Middle, Lower Trapezius, Lateral Thoracic Serratus Anterior, Pectoralis Major Deep Scapular Lattisimus Dorsi Suprascapular Supraspinatus, Infraspinatus, Brachial Coracobrachialis Axillary Pectoralis Minor Dorsal Scapular Levator Scapulae, Major and Minor Rhomboideus Posterior Circumflex Anterior, Middle, and Posterior Deltoids Circumflex Scapular Teres Minor and Major Subscapular Subscapularis NERVES SHOULDER JOINT NERVES: CERVICAL PLEXUS NERVE ORIGIN STRUCTURE INNERVATED Cervical Nerves C3, C4 Levator Scapulae SHOULDER JOINT NERVES: SPINAL ACCESSORY NERVE NERVE ORIGIN STRUCTURE INNERVATED Spinal Accessory Cranial Nerve XI Upper, Middle, and Lower Trapezius, Cervical Plexus and Spinal Accessory Nerve SHOULDER JOINT NERVES: BRACHIAL PLEXUS • The Brachial Nerve Plexus is made up of roots, trunks, divisions and cords, formed by combining the lower 4 cervical nerves (C5 – C8) and the first thoracic nerve (T1). The Brachial Plexus is responsible for the innervation of the muscles of the upper extremity (except the Levator Scapula and trapezius) BRACHIAL PLEXUS (C5 – T1) CADAVER of Brachial Plexus Brachial Plexus: With Muscle and Skin Brachial Plexus NERVE ORIGIN MUSCLE INNERVATED Dorsal Scapula C5, C4 Rhomboids, levator Scapulae Long Thoracic C5, C6, C7 Serratus Anterior Superior Trunk Suprascapular C4,C5,C6, Lateral Cord Lateral Pectoral C5, C6, C7 Medial cord Medial Pectoral C8, T1 Posterior Cord Axillary C5, C6 Lateral Cord Musculocutaneous C5 - C7 Posterior Cord Thoracodorsal C6, C7, C8 Posterior Cord Subscapular C5, C6 Supraspinatus and infraspinatus, shoulder joint Pectoralis major and minor Pectoralis minor and sternocostal of pectoralis major Glenohumeral Joint, teres minor, deltoid muscles, (sensory) skin of superolateral arm Coracobrachialias, biceps brachi, brachialias, (Sensory) skin of lateral forearm Lattissimus dorsi Subscapularis, Teres Major Surface anatomy Surface anatomy cont. • TIPS ACCEPTED • PLEASE APPLAUD • ANY QUESTIONS? • THE END