Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
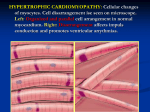
Prof. N. Sudhaya Kumar, AIMS, Cochin Primary cardiomyopathies Genetic HCM ARVD LV noncompaction Mitochondral myopathy Glyc.storage dis. channelopathies Mixed Acquired DCM RCM Inflammatory Tachycardiomyopathy Takotsubo Infants of IDDM mothers HCM Most common of the genetic CVD Mutation in genes coding proteins of sarcomere Autosomal dominant pattern of inheritance Heterogenous manifestation Unique pathophysiology Diverse clinical course HCM • most common cause of SCD in children •30 % of SCD in competitive athletes • LVH is a dynamic process • occasionally LVH appears at or slightly after birth • striking increase in LVH during adolescence HCM .. GENETICS • autosomal dominant • usually missense mutations in genes that encode sarcomere proteins • HCM mutant proteins are incorporated into cardiac myofilaments Hypertrophy, remodeling, fibrosis, dysfunction • 50% of first degree relatives are at risk of inheriting the mutation HCM .. GENETICS Mutations missense, deletions,insertions,nonsense In thick filament proteins thin filament proteins metabolic genes lysosomal proteins HCM .. GENETICS Protein chrom gene incidence clinical BMHC 14 MYH7 40% MYBPC 11 MYBPC3 Titin 2 TTN TropT 1 TNNT2I Trop I 19 TNNI 3 rare ?apical ; restrictive physio Actin 15 ACTC rare ? Apical TPM 1 < 5% variable degree LVH good prognosis > in Finland Thick filament 40% rare classical HCM ?regression with statin mild LVH, older age, good prognosis typical HCM Thin filament Tropomyosin 15 5% modest LVH ; high SCD ? Benefit with losartan/ spirono HCM .. Classification (Maron’s) Type 1 ..Hypertrophy confined to anterior IVS … 10% 2 .. Hypertrophy involving ant. & inferior IVS.. 20% 3 .. ,, IVS and lateral free wall 52% 4 .. ,, regions other than IVS 18% 5 .. Apical HCM HCM -- Pathophysiology • LV diastolic dysfunction pulm. congestion • LV outflow obstruction dynamic SAM , hypercontractile septum • myocardial ischemia inadequate capillary density abnormal microvasculature myocardial bridging of coronaries • arrhythmia ischemia ; LVH ; fibrosis ; cardiac failure HCM .. Clinical Asymptomatic / symptomatic .. Dyspnea, angina, SCD.. Pulse .. brisk, spike and dome pattern JVP .. A + Apex .. Double / triple Murmurs .. LVOT / MR any situation which reduces LV size increases the obstruction Apex cardiogram in HOCM ACG ACG Normal HOCM HCM .. hemodynamics HCM – Natural history • presentation at any age • overall mortality - 1% per year ; in children 2% • SCD -- more in adolescence and young adults rare < 10 yrs extremely uncommon in infancy commonly arrhythmia based - VT / VF > in early morning hours sedentary / modest activity during or just after vigorous activity HCM .. risk factors for SCD Major • prior cardiac arrest / sustained VT • family h/o HCM related SCD • syncope • repetitive nonsustained VT • massive LVH > 30 mm • fall in BP during exercise Possible • malignant genotype • LVOT gr > 50 mm Hg • myocardial ischemia • AF • competitive physical exertion HCM -- Management • Pharmacologic betablockers, verapamil , disopyramide antiarrhythmics .. ? Amiodarone anticoagulation antifailure measures • Pacing • PTSA • ICD • Surgery HCM …. Pacing DDD pacing …. ? Benefit 2 randomised studies • modest reduction in LVOT gr . 25 – 40 mm Hg • subjective improvement • treadmill time / max. O2 cons. didn’t improve ? Placebo effect Pacing In Cardiomyopathy trial …. Similar data Conclusion : can be an option for severely symptomatic patients refractory to medical treatment and not planned for other treatment modalities HCM -Surgery • for patients with drug refractory symptoms and LVOT gradient of > 50 mm Hg • septal resection (Morrow procedure) • operative mortality < 1% ; 0% in Mayo series • in 90% - abolition / reduction in LVOT gr • in 85% - symptom relief • 83 % 10 year survival HCM -- PTSA 1 – 3 ml of 96 –98 % alcohol is injected into the septal artery Necrosis and thinning of IVS Reduction in LVOT gradient • scar may enhance arrhythmic death • high incidence of heart block • procedure mortality of 2% Hence surgery is preferred in children HCM … PTSA Vs surgery myectomy PTSA Procedure mortality 1–2% 1–2% Gr. reduction (rest) to < 10mm Hg to < 25 mm Hg Symptoms less less PPI for AVB 1–2% 5 – 10 % Intramyocardial scar absent present Longterm SCD risk very low ? HCM … PTSA Vs surgery CMR after myectomy Vs PTSA HCM ..Prevention of SCD • drugs -- ? Role • ICD -- for primary and secondary prevention Primary … > 1 major risk factor Secondary .. SCD / sustained VT • study of 128 pts appropriate shock in 11% in secondary prevention and 5% in primary prevention HCM .. management Asymptomatic SCD risk high … ICD HCM Follow up AF………cardioversion,rate control anticoagulation paroxysmal AF.. ? amiodarone Progressive symptoms DRUGS BB ,verapamil, disopyramide Refractory Nonobstructive Tt of CHF Heart transplant obstructive Surgery … PTSA ?? DDD HCM - screening < 12 years – optional unless family h/o HCM death competitive athletes symptomatic 12 – 18 years -- every 12 –18 months > 18 years -- every 5 years HCM Vs athletes heart HCM Athletes heart Unusual pattern of LVH + _ LV cavity > 55 mm _ + LA enlargement + _ Bizarre ECG + _ Abnormal LV filling ++ ± LVH regression with deconditioning _ + Family h/o ++ _