Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
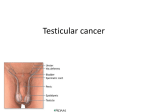
TESTICULAR CANCER GÖZDE AKAN BERFİN GİZEM USLU ANATOMY Paired, ovoid male reproductive organ 4 x 3 x 2.5cm approximately 25 ml 250-350 lobules Lies obliquely within the scrotum suspended by the spermatic cord FUNCTIONS Produce sperms and male hormones, primarily testosterone LYMPHATIC DRAINAGE On the right : along the IVC - interaortacaval region - preartic and paraaortic lymph nodes ,with possible crossover within the retroperitoneum On the left : preaortic and paraaortic nodes around the left renal hilum - interaortacaval nodes mostly without cross-over EPIDEMIOLOGY Uncommon malignancy, accounting for 1–2% of all tumours in men However, it is important because its incidence is increasing worldwide Most common malignancy in young men (aged 15–34 years) in many populations worldwide The peak age of men with seminomas is 30–40 years, compared with 20–30 years for nonseminomatous GCT Contrary to the trends in incidence, the testicular cancer mortality rate has been decreasing in most European countries, largely attributable to the advent of platinumbased chemotherapy regimens and multidisciplinary approach to testicular cancer management RISK FACTORS 1. Cryptorchidism -four to eight times greater risk 2. Prior Testicular Cancer- 500-fold higher rate than in the general population 3. Genetics- Klinefelter syndrome (47XXY) Down syndrome Androgen insensitivity syndrome 4. Family history 5. Infertility 6.Environmental exposure 7.Scrotal trauma 8.Inguinal hernia 9.Smoking 10.Race-more common among Caucasian males Highest rates in Scandinavia, Germany and New Zealand 11.HIV CLINICAL FEATURES • • • • • • • Due to metastasis; Due to primary tumor; • Abdominal or lumbar pain Painless testicular lump (lymphatic spread) Sensation of heaviness • Dyspnea, hemoptysis and Rarely pain (1/3rd cases) chest pain with lung May mimic metastasis epidedymoorchitis • Jaundice with liver metastasis Gynaecomastia appears in • Hydronephrosis by para-aortic 7% of cases lymph nodes enlargement • Pedal edema by IVC obstruction PHYSICAL EXAMINATION: • Enlarged testis (except choriocarcinoma) • Nodular testis • Loss of testicular sensation • Flat and difficult to feel epididymis • General examination for metastasis CLASSIFICATION OF TESTICULAR TUMORS Germ Cell Tumors (%90) A. Seminomas (%60) 1. Classical 2. Spermatocystic 3. Anaplastic B. Non-Seminomatous Tumors (%40) 1. Embryonal Carcinoma 2. Yolk Sac Tumor 3. Choriocarcinoma 4. Teratoma 5. Mixed Tumors Non-Germ Cell Tumors A. Sex-Cord Stromal Tumors (%2) 1. Leydig Cell Tumor 2. Sertoli Cell Tumor 3. Granulosa Cell Tumor 4. Mixed Type 5. Unclassified B. Mixed Germ Cell and Stromal Tumor C. Adnexal and Paratesticular Tumors D. Miscellaneous Tumors (%5) (Metastatic tumors, Carcinoid,Lymphoma) GERM CELL TUMORS 1) Seminoma testicular cancer • The commonest variety of testicular tumour • Adults are the usual target (4th and 5th decade); never seen in infancy • Patients present with painless testicular mass • 30 % have metastases at presentation, but only 3% have symptoms related to metastases • Serum alpha fetoprotein is normal • Beta HCG↑30% of patients with Seminoma • Highly sensitive to radiotherapy among testis tumors SEMINOMA CLASSICAL (%85) Middle age (30-50) ↑BetaHCG(10%) Very slow growth Spermatocytic(2% - 12% ) yrs ANAPLASTIC (5% - 10) Middle age Aggressive - lethal Greater mitotic activity Higher local invasion Higher metastatic potential Old age (> 50 yr) Most common GCT in men > 65 Higher rate of β-HCG production Extremely low metastatic potential Good prognosis 2)NON-SEMİNOMATOUS GERM CELL TUMORS 2. a) Embryonal Carcinoma: 2nd most common germ cell tumor 90% of NSGCT Present in majority of mixed germ cell tumours Most men present in their 20s to 30s with a testicular mass Highly malignant tumours; may invade the cord structures epididymis High degree of metastasis Serum AFP is positive in 30%, beta HCG is elevated in 20% of cases 2)NON-SEMİNOMATOUS GERM CELL TUMORS 2.b) Choriocarcinoma: • A rare and aggressive tumour (5years survival is 5%) Typically elevated B-Hcg > 99% Usually present with distant mets – lung and /or brain Primary is very small and often exhibit NO TESTICULAR ENLARGEMENT, small palpable nodule may be present. Hematogenous mets most common 2)NON-SEMİNOMATOUS GERM CELL TUMORS 2.c) Yolk sac tumor: • Most common prepubertal GCT in children. • Pure yolk sac tumor <2% of testicular tumors in adults • 40% of mixed germ-cell tumors. • AFP ↑ >90% of pts • Testicular mass the most usual presentation • Respond very well to chemotherapy, even if they have spread • Microscopically, Schiller-Duval bodies are a characteristic feature 2)NON-SEMİNOMATOUS GERM CELL TUMORS 2.d) Teratoma: Teratoma in greek means “monster tumor” Contain all three germ layers with varying degree of diffrentiation Occurs in its pure form in pediatric age group with a mean age of diagnosis at 20 months In adults, occur as a component of mixed germ cell tumor Normal serum markers. ◦ Mildly elevated AFP levels 3)SEX CORD STROMAL TUMORS 1. Sertoli cell: 3. Granulosa cell -Excess estrogen production 4. Mixed types -Gynecomastia in 1/3rd of cases -10 % are malignant -Androgen insensitivity syndrome -Peutz-Jeghers syndrome 2. Leydig cell: -Produces androgens -Reinke crystals -Klinefelter’s syndrome METASTATIC TUMORS OF TESTIS Lymphoma -most common secondary tumor -most common testicular tumor in patients above 50 years Leukemia Prostate cancer SPREAD 1. Direct Spread: This spread occurs by invasion. Tunica albuginea is rarely penetrated Scrotal skin involvement Spread to spermatic cord and epidedymis may occur : points towards bad prognosis 2. Lymphatic spread: Seminoma metastasize exclusively through lymphatics They drain primarily to para-aortic lymph nodes 3. Blood Spread NSGCT spread through blood route Lungs, liver, bones and brain are the usual sites usually involved TUMOR MARKERS AFP (alpha-fetoprotein): Trophoblastic Cells -upper limit of normal serum AFP<10-15 microg/L -serum AFP concentrations >10,000 microg/L are found almost exclusively in patients with (NSGCTs) or hepatocellular carcinoma B-HCG: Syncytiotrophoblastic Cells -most commonly elevated tumor marker in testicular cancer -normal value in men is less than 5 to 10 IU/L -Increased levels of beta-HCG can be found in seminoma or nonseminoma TUMOR MARKERS Lactate Dehydrogenase (LDH): -elevated in 40 to 60 percent of men with testicular germ cell tumors -less sensitive and less specific tumor marker than (beta-hCG) or (AFP) for men with NSGCTs - increased levels reflect tumor burden, growth rate, and cellular proliferation AFP, BHCG & LDH are included in TNM staging of testicular cancers DIAGNOSIS Painless swelling or a nodule in one testicle is the most common presenting sign In any man with a solid, firm mass within the testis, testicular cancer must be the considered diagnosis until proven otherwise Physical examination Scrotal USG Blood test: CBC + AFP , B-HCG , LDH CT Scan, MRI, PET Scan Radical inguinal orchiectomy Contralateral testicular biopsy Retroperitoneal lymph node dissection DDx Epididymo-orchitis Hematoma Torsion Paratesticular neoplasm (most commonly benign) Hernia Varicocele-spermatocele Tuberculosis and other testicular infections STAGING(for all patients) Serum tumour markers -AFP -hCG -LDH Abdominopelvic CT Chest X-ray/ CT Testis ultrasound (bilateral) TNM STAGING Testicular cancer is staged using the TNM system created by the American Joint Committee on Cancer (AJCC). T refers to how much the main (primary) tumor has spread to tissues next to the testicle. N describes how much the cancer has spread to regional (nearby) lymph nodes. M indicates whether the cancer has metastasized (spread to distant lymph nodes or other organs of the body). S indicates the serum (blood) levels of tumor markers that are made by some testicular cancers. ROYAL MARSDEN CLASSIFICATION Stage I: Cancer is found only in the testicle. Stage II: Cancer has spread to the retroperitoneal lymph nodes in the belly. -IIA: <2 cm in size or < 6 positive nodes -IIB: 2-5 cm in size or > 6 positive nodes -IIC: large and bulky abdominal mass, usually > 5-10 cm Stage III: Cancer has spread beyond the lymph nodes in the belly. There may be cancer in parts of the body far away from the testicles such as the lungs, brain, bones and liver. Stage IV: Hematogenous spread GENERAL MANAGEMENT After obtaining serum AFP & B-Hcg levels in suspected case of malignant germ cell tumour Radical inguinal orchietectomy with high ligation of spermatic cord is done, it is both diagnostic & therapeutic Further management depends on, pathology & stage of disease. Radical inguinal orchietectomy Testicular tumors are diagnosed, staged and locally controlled by inguinal orchiectomy. Scrotal biopsy is irrelevant and contraindicated. TREATMENT Radical Inguinal Orchiectomy Surveillance Retro Peritoneal Lymph Node Dissection(RPLND) Radiotherapy Chemotherapy SEMINOMAS TX 1. Early Stage Radiation therapy (gold standard) Surveillance (selected cases) 2. Advanced Stage Chemotherapy NONSEMINOMAS TX Early Stage (Stage I) Retroperitoneal Lymph Node Dissection Open / Laparoscopic Surveillance (low-risk patients) Chemotherapy (2 courses) (high-risk patients*) * angio-lymphatic invasion >%50 presence of embryonal cell carcinoma Absence of yolk sac component Advanced Stage (>IIB) Chemotherapy (BEP : Bleomycin/etoposide Cisplatin) PROGNOSIS High-risk prognostic features include any of the following: Mediastinal primary tumor Nonpulmonary visceral metastases AFP > 10,000 ng/mL hCG > 50,000 IU/L LDH > 10 times the upper limit A good prognosis can typically be expected in patients with the following: Testicular or retroperitoneal primary tumor No nonpulmonary visceral metastases Alpha-fetoprotein < 1000 ng/mL Human chorionic gonadotropin < 5000 IU/L Lactate dehydrogenase (LDH) < 1.5 times the upper limit FOLLOW-UP At least 5 years with: -periodic x-rays -CT scans -blood tests for tumor markers Also, since there is an increased risk (about 2%) of a second tumor, it is important to continue monthly testicular self-exams. REFERENCES "What Is Testicular Cancer?" American Cancer Society. N.p., n.d. Web. 01 Apr. 2017. <https://www.cancer.org/cancer/testicular-cancer/about/what-is-testicularcancer.html>. "Testicular Cancer." Background, Pathophysiology, Epidemiology. N.p., 13 Mar. 2017. Web. 01 Apr. 2017. <http://emedicine.medscape.com/article/279007overview>. "Testes and Epididymis Anatomy." Overview, Gross Anatomy, Microscopic Anatomy. N.p., 28 Oct. 2016. Web. 01 Apr. 2017. <http://emedicine.medscape.com/article/1949259-overview#a2>.